JR Ryder et al. N Engl J Med 2024;391:1656-1658. DOI: 10.1056/NEJMc2404054. Ten-Year Outcomes after Bariatric Surgery in Adolescents
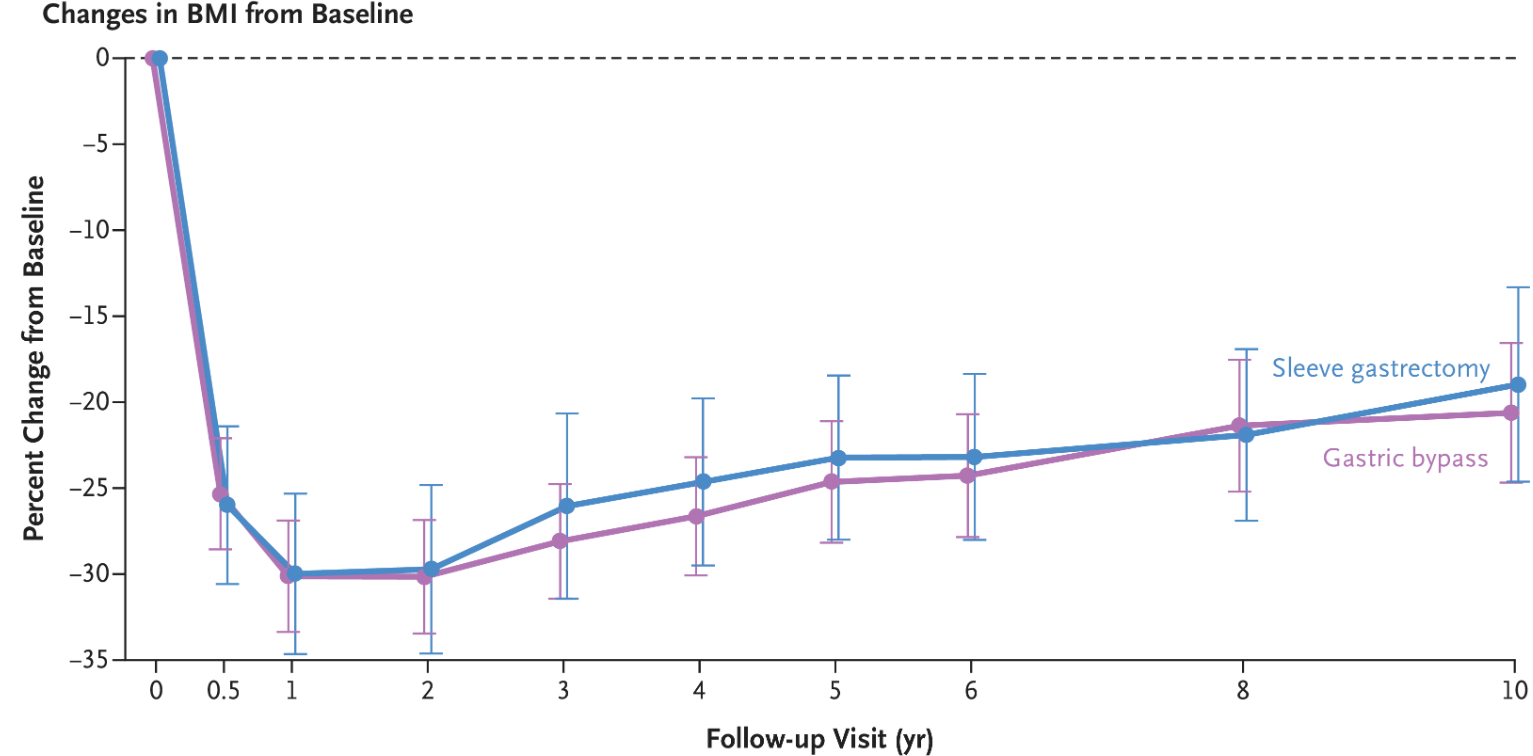
Methods: The Teen Longitudinal Assessment of Bariatric Surgery (Teen-LABS) is a prospective multicenter observational cohort study involving adolescents (13 to 19 years of age) undergoing bariatric surgery. Participating adolescents underwent either gastric bypass (161 participants) or sleeve gastrectomy (99 participants) at a mean age of 17 years. Overall, 83% of the 10-year postoperative visits were completed.
Key findings:
The changes in BMI were similar with gastric bypass (mean change, −20.6%) and sleeve gastrectomy (mean change, −19.2%)
Ten years after bariatric surgery, the modeled percentages of participants with remission of coexisting conditions (55% for type 2 diabetes, 57% for hypertension, and 54% for dyslipidemia)
My take (borrowed from authors): “These findings show the long-term durability of weight loss and remission of coexisting conditions after bariatric surgery, as well as the greater health benefits and durability of the effects in adolescents than would be expected in similarly treated adults.”
Related article: H Bliddal et al.N Engl J Med 2024;391:1573-1583. Once-Weekly Semaglutide in Persons with Obesity and Knee Osteoarthritis. Key finding: “treatment with once-weekly injectable semaglutide resulted in significantly greater reductions in body weight and pain related to knee osteoarthritis than placebo.”
The researchers found a 25.6% drop in people undergoing bariatric surgery in the final six months of 2023 compared with the number of surgeries people had during the same period the year before. During the latter half of 2023, the number of patients who took a glucagon-like peptide 1, or GLP-1 medication for weight loss, surged by more than 130%, according to a study published Friday in JAMA Network Open…Another popular weight loss drug, Eli Lilly’s Zepbound, was not included because the Food and Drug Administration did not approve it until November 2023…[And there are] anecdotal reports of hospitals that shut down bariatric surgery programs as the number of patients seeking operations slumped…
In 2022, nearly 280,000 metabolic and bariatric procedures were performed in the United States, according to the American Society for Metabolic and Bariatric Surgery. That represented about 1% of all U.S. residents eligible for weight loss operations…The CDC estimates that about 40% of U.S. residents have obesity and 1 in 10 have severe obesity.
Reference: Lin, K., et al. (2024). Metabolic Bariatric Surgery in the Era of GLP-1 Receptor Agonists for Obesity Management. JAMA Network Open. doi.org/10.1001/jamanetworkopen.2024.41380.
Methods: This cross-sectional study, we used 2022 to 2023 deidentified claims from 17 million unique deidentified adult patients with medical and pharmaceutical coverage through commercial and Medicare Advantage insurance in the OptumLabs Data Warehouse. We included only patients without diabetes and with obesity.
**Only 6% of patients with obesity in the study population received either GLP-1 drugs or surgery, suggesting that many more patients could be receiving treatment.
My take: The GLP-1 drugs have established a medical therapy with a good probability of effectiveness. This was lacking from prior medical treatments. It certainly is logical that their availability could reduce the use of bariatric surgery. The AAP may need to revise their bariatric surgery recommendations from 2020.
Methods: This retrospective cohort study analyzed electronic health record data of 603,051 adolescents aged 13 to 17 years between January 1, 2018, and December 31, 2021
Key findings:
4.4% (1 in 23) of all adolescents met the eligibility criteria for bariatric surgery.
22.2% had obesity (12.9% class 1, 5.4% class 2, and 3.9% class 3).
The most frequently diagnosed comorbid conditions were gastroesophageal reflux disease (3.2%), hypertension (0.5%), and nonalcoholic fatty liver disease (0.5%).
The authors estimate that ~1 million U.S. adolescents meet criteria for bariatric surgery though only ~1700 receive this treatment yearly
The study strongly demonstrates that the comorbid conditions associated with obesity are underdiagnosed. In some cases this is because the screening is not done; yet, in other cases, despite screening, comorbid conditions go undiagnosed. For example, the prevalence of hypertension based on having at least 3 elevated BP measurements was 10 times higher than the prevalence based on the diagnosis being made (ICD 10) codes
My take: A lot of kids meet criteria for bariatric surgery but few undergo this surgery. If effective anti-obesity medications become more widely adopted (affordable), this may be a preferable option to surgery, especially in the pediatric age group. Surgery could be deferred to those who did not respond. Also, immediate implications of the study are that we need to be more diligent about looking for associated health problems (eg. OSA, HTN, T2DM, MASLD).
This is a terrific review of obesity and current management options, including surgery and medications. The review provides a thorough explanation of some of the reasons why we are having so many more children with obesity. The article personalizes the problems by focusing on one teen, Alexandra, who underwent sleeve gastrectomy.
Here are a few excerpts (from this lengthy article):
In response to so many grim facts, the A.A.P. in January released its first “clinical practice guideline” for those who care for children who have obesity. The academy now recommends that they immediately start “intensive health behavior and lifestyle treatment,” which it labels “the foundation” of obesity management; this approach supersedes the former strategy of “watchful waiting.” For older youth in certain circumstances — those with a higher B.M.I., say — drugs and, in cases of severe obesity, surgery should be made available as options...
The tenacity ofbody weight can be traced to our biology. Humans evolved to resist losing body fat so that we don’t become extinct, says Rudolph Leibel, chief of the pediatric molecular genetics division at Columbia University’s medical center…
A small number of children with severe obesity are born with leptin deficiency, a gene mutation identified by Sadaf Farooqi, a professor at the University of Cambridge’s Institute of Metabolic Science. Their appetites seem to be bottomless. Though it’s rare, Farooqi cites the extreme effect of this mutation as a clear illustration of the “very strong” impact that biology has upon appetite….Ghrelin, a hunger hormone, increases when food intake is restricted, making us eat more. Insulin, another important hormone, helps turn the food we eat into energy and controls things like blood sugar that influence how much we eat…“We don’t decide whether we’re going to be hungry or not, whether we’re going to have a craving or not….
Genetics may determine more than 70 percent of children’s body weight…But if our genes didn’t change significantly in the last century, why, then, are children getting bigger?No one knows for sure. One likely explanation, however, is the evolutionary mismatch between our genes and our surroundings…
The amount of readily accessible food has expanded immensely, making it easier than ever to eat — open a phone app, say, or go to a drive-through. Plenty of Americans can consume as much as they want, whenever they want.
Today nearly 70 percent of what children eat is ultraprocessed food… Ultraprocessed foods appeal to parents too: They’re cheap, last for years in pantries and freezers and require little preparation. “All food companies are trying to sell products,” Nestle says. “That’s the system, and if the system makes kids fat, well, too bad. Collateral damage.”..Over the past few decades, the variety of food items in some supermarkets has risen to more than 40,000 from 7,000…
Adolescents who have had bariatric surgery — most of them white and female — experienced weight loss similar to what adults lost: around 25 percent of their B.M.I. And while nearly 90 percent of these teenagers needed diabetes medications before the operation, none did afterward…Only a tiny fraction of the teenagers with severe obesity who qualify actually receive the operation…
The latest glucagon-like peptide-1 receptor agonists — as a group, commonly referred to as Ozempic — are the true game changers, a class of drugs that are making possible a degree of weight loss not seen before with medications. The pharmaceutical company Novo Nordisk manufactures GLP-1s for weight loss, one of which is semaglutide and sold under the brand name Wegovy. (Ozempic is the brand name for a lower-dose version of semaglutide that is prescribed to treat diabetes)…
The major studies of children and these drugs have enrolled many fewer adolescent subjects than adults, but no new safety concerns have emerged. In addition to semaglutide’s principal side effects of nausea, vomiting and diarrhea — reported by two-thirds of study participants — more serious ones include gallstones and pancreatitis. Wegovy comes with a caution about possible thyroid cancer, and the F.D.A. mandates that it include a warning about the possibility of suicidal ideation, because it acts on the brain…If patients discontinue the medicines, the weight returns…older drugs in its class have been used to treat diabetes for nearly two decades. But for any new medicine, the long-term risks remain uncertain…
For now, most adolescents who qualify for semaglutide probably won’t be able to get the drug at all [due to cost and drug shortages]….
[At the same time] a greater awareness of the drawbacks that can accompany the medicalizing of obesity, have fueled popular body-positivity movements like Health at Every Size, which seek to disentangle weight from health…
But despite the risks that can accompany obesity treatments — and despite the fact that the data doesn’t always present a clear picture — the prevailing attitude within the medical establishment is that, on balance, the potential negative consequences of obesity are too evident to ignore
Methods: VEDOKIDS was a paediatric, multicentre, prospective cohort study done in 17 centres in six countries. We report the 14-week outcomes as the first analyses of the planned 3-year follow-up of the VEDOKIDS cohort
Key findings:
32 (42%) of 77 children with ulcerative colitis and 21 (32%) of 65 children with Crohn’s disease were in steroid-free and exclusive enteral nutrition-free remission at 14 weeks.
In children who weighed less than 30 kg, the optimal drug concentration associated with steroid-free and exclusive enteral nutrition-free clinical remission was 7 μg/mL at week 14, corresponding to a dose of 200 mg/m2 body surface area or 10 mg/kg
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
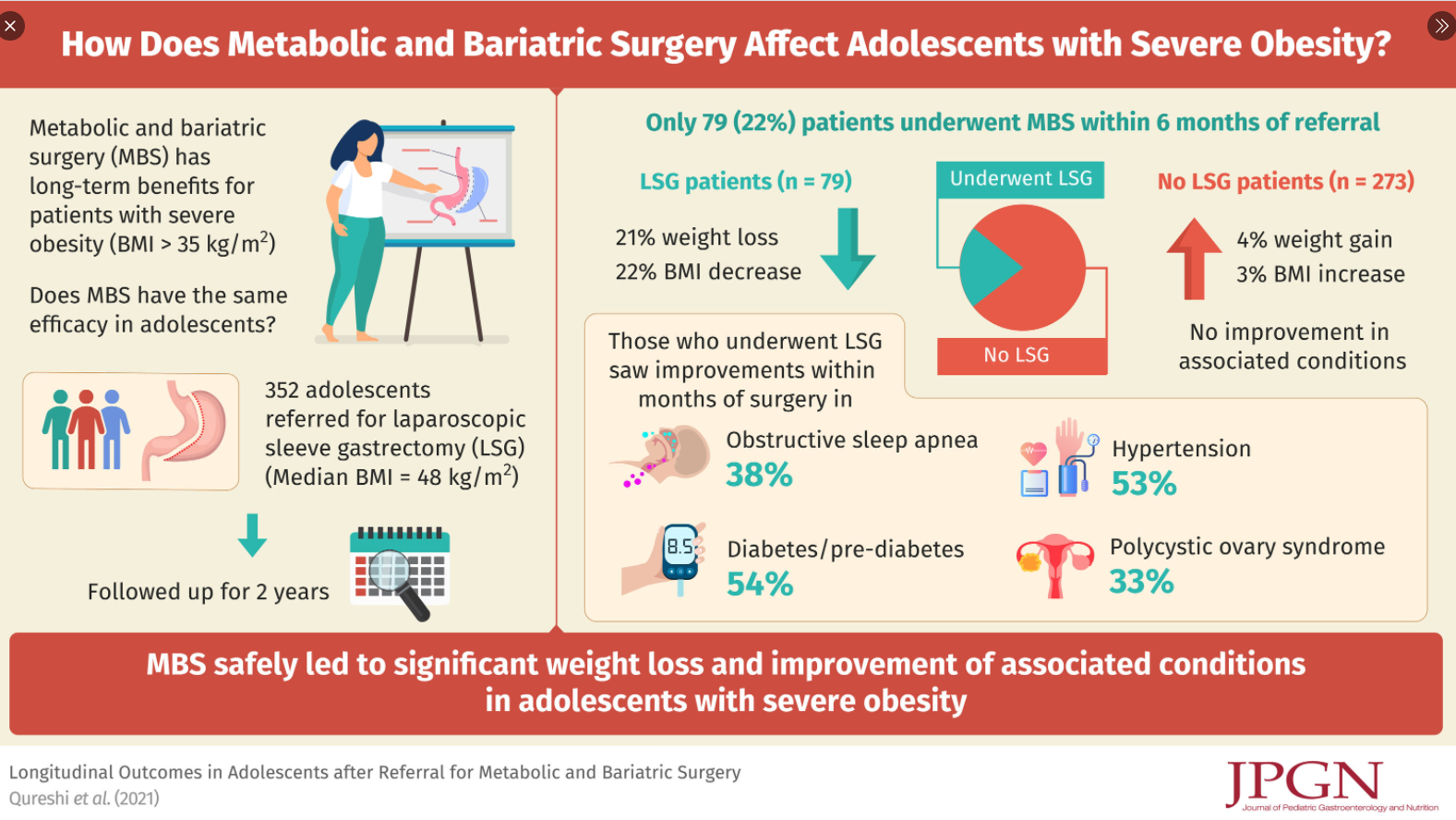
Only 22% underwent bariatric surgery (Laparoscopic sleeve gastrectomy (LSG)), mainly due to lack of interest in those referred
Reasons for NoLSG: 171 (62% of the NoLSG group) did not return for a 2nd visit, 28 (10%) were considered non-adherent to clinical recommendations, 14 (6%) had insurance denials, 16 (6%) had psychological contraindications including recent suicidal ideations, and 29 (11%) are still considering/pursuing LSG
Only 8 (2.3%) of entire cohort were self-pay
LSG patients had 21% total weight loss and 22% total BMI loss at 24 months whereas NoLSG patients had 4% total weight gain and 3% BMI gain (P < 0.01)
LSG group had improvement in obesity-associated conditions compared to group without surgery (P < 0.01)
Follow-up in both groups was poor (40% for LSG group and <20% for the NoLSG group) 1 year after bariatric referral. This is of particular interest in the LSG group b/c for surgery, patients are required to agree to a 5 year f/u period (though this lacks an enforcement mechanism). The authors note some improvement in f/u coincident with recent broader adoption of telemedine
My take: This single-center found that most patients referred for consideration of bariatric surgery did not have this surgery.
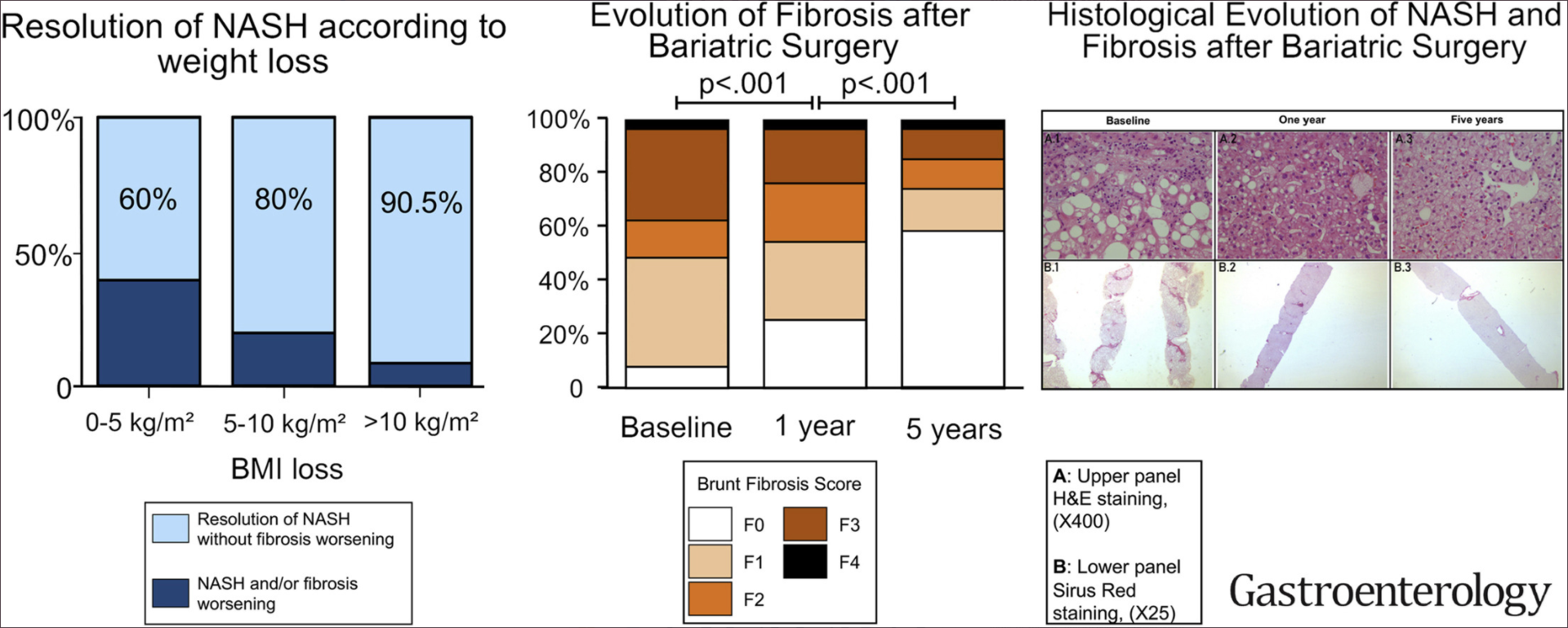
This was a prospective study of 180 severely obese patients with biopsy-proven NASH.
Key findings:
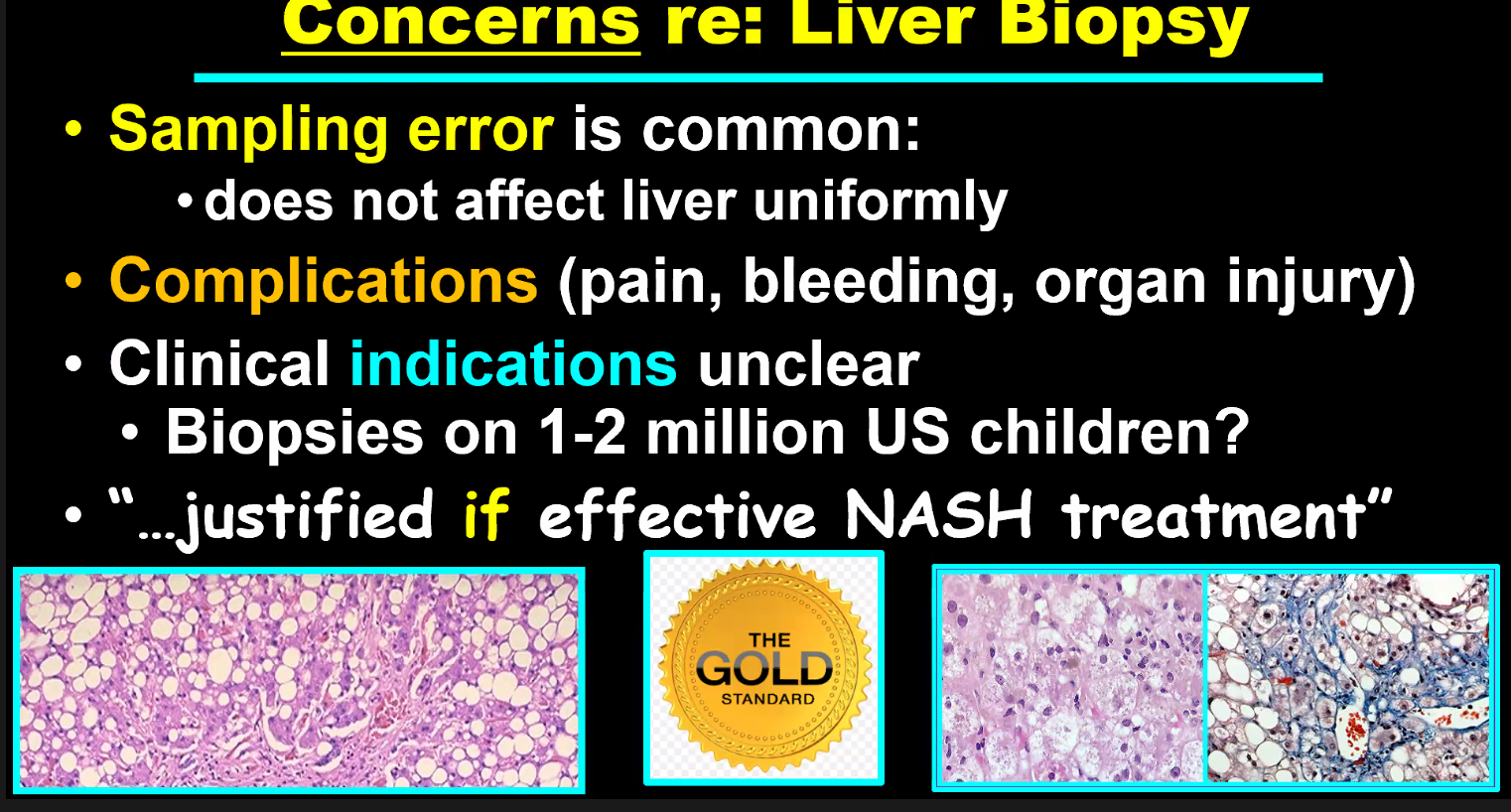
NASH: At 5 years after bariatric surgery, NASH was resolved, without worsening fibrosis, in samples from 84% of patients (n = 64; 95% confidence interval, 73.1%-92.2%).
Fibrosis: Fibrosis decreased, compared with baseline, in samples from 70.2% of patients (95% CI, 56.6%-81.6%). Fibrosis disappeared from samples from 56% of all patients (95% CI, 42.4%-69.3%) and from samples from 45.5% of patients with baseline bridging fibrosis.
Graphic Abstract
My take: This study showed that patients with NASH who underwent bariatric surgery had resolution of NASH in liver samples from 84% of patients 5 years later. The reduction of fibrosis was progressive, beginning during the first year and continuing through 5 years.
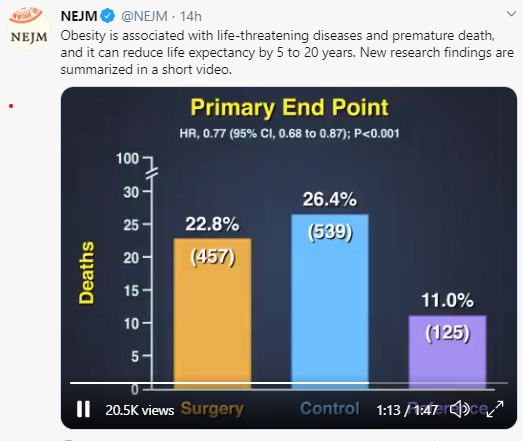
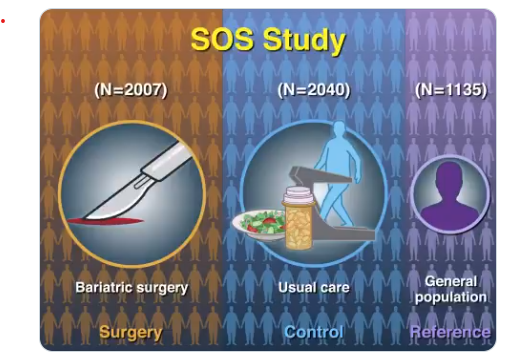
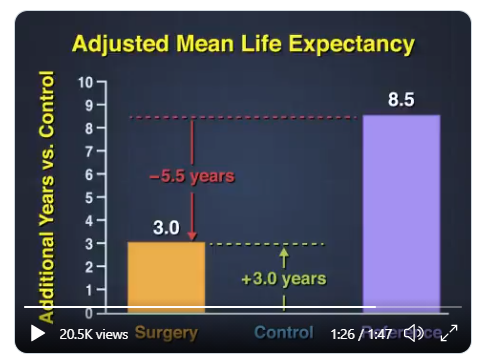
A recent study (LMS Carlsson et al. NEJM 2020; 383: 1535-43) was summarized in a quick take. Essentially, obese subjects who underwent bariatric surgery survived three years longer than a control group who had not undergone surgery but lived 5 years shorter than a reference group without obesity.
The authors speculate on the reasons why the bariatric subjects continued to have a lower life expectancy than controls after surgery:
Above-normal BMI even after surgery
Irreversible effects of obesity-related metabolic dysfunction
Surgical complications
Higher risk of alcohol abuse, suicide, and trauma (including fall-related); these factors were identified in the SOS study more often than in those who had not undergone bariatric surgery
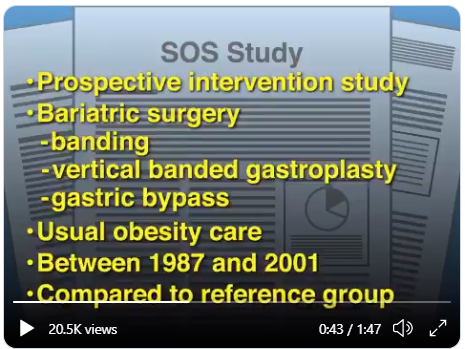
Since there have been improvements in bariatric surgery since the time of this cohort underwent surgery (1987-2001), it is possible that the average gain in life expectancy would be greater.
Rock artThis tweet was posted on 10/21/20Ful Text Link: COVID-19 Mortality Risk in Down Syndrome: Results From a Cohort Study Of 8 Million Adults15 min video Link: How America Helped Defeat the Coronavirus* (not in U.S.). an excerpt: We’ve all heard how U.S. leadership failed its citizens with its pandemic response. We had the playbooks, we had the money, we had the experts. We just … didn’t use them. But it turns out, other countries did. Because U.S. public health leaders and scientists have been planning for a catastrophe just like Covid-19 for decades, and, in typical American fashion, we didn’t just write the pandemic playbook — we exported it around the world.