
S Xanthakos et al. Clin Gastroenterol Hepatol 2020; 18: 1070-81. Full Text: Nutritional Risks in Adolescents After Bariatric Surgery
This was a multicenter prospective cohort study with 226 adolescents (mean age 16.5 years, mean BMI of 52.7) who had either Roux-en-Y bypass (RYGB, n=161) or vertical sleeve gastrectomy (VSG, n=67).
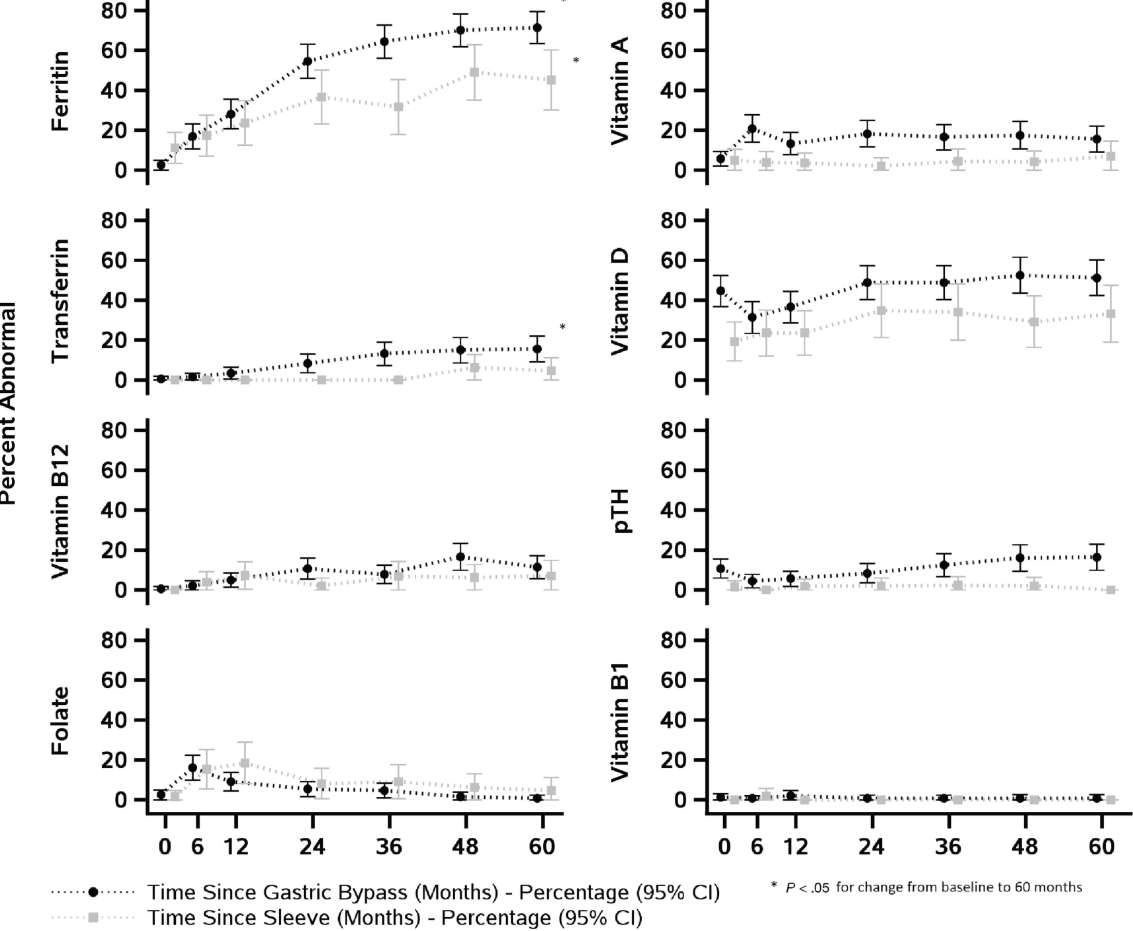
Key findings:
- At 5 years, 59% of RYGB and 27% of VSG had ≥2 nutritional deficiencies
- The most prevalent abnormality we observed was hypoferritinemia, which affected nearly twice as many RYGB recipients by Year 5 compared with VSG.
- Vitamin B12 status likewise worsened disproportionately after RYGB, despite similar trajectories of weight loss after VSG
- Image below shows the prevalence of abnormal values for vitamins over time
My take: This study shows that adolescents undergoing VSG had fewer nutritional deficiencies than RYGB and provides data supporting nutritional monitoring after bariatric surgery.
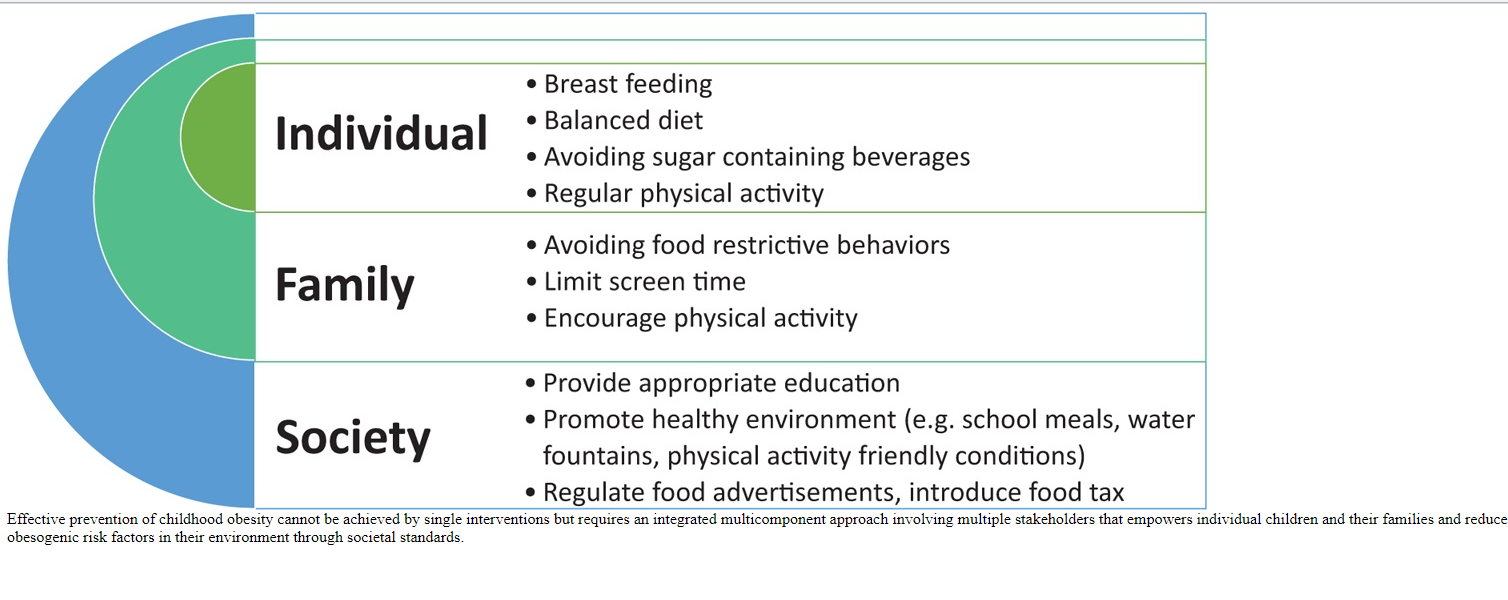
B Koletzko et al. JPGN 2020 70: 702-10. Full Text: Prevention of Childhood Obesity: A Position Paper of the Global Federation of International Societies of Paediatric Gastroenterology, Hepatology, and Nutrition (FISPGHAN)
Related blog posts (Bariatric Surgery):
- AAP Bariatric Surgery Recommendations (2020)
- Reaching Consensus on Bariatric Intervention in Children …
- 12 Year Data: Pros and Cons of Bariatric Surgery
- Bariatric Surgery Survival -5 Countries, 500,000 Participants
- Adolescent Bariatric Surgery Outcomes at 3 Years | gutsandgrowth
- Comparing Gastric Bypass Outcomes in Adolescents and Adults
- How Often Do Children with Obesity Have a Fatty Liver?
- Should teenagers with severe NAFLD undergo bariatric surgery?
- Is a Three Year-Old Too Young for Bariatric Surgery …
- Treating diabetes with surgery | gutsandgrowth
- NAFLD Guidance from American Association for the Study of Liver Diseases
- Psychology of obesity and food addiction | gutsandgrowth
- Staggering cost of obesity | gutsandgrowth
Related blog posts (Obesity):
- The Paramount Health Challenge for Humans in the 21st Century
- NY Times: “Our Food is Killing Too Many of Us”
- Bad diets –>High Mortality
- Better Diet, Lower Mortality
- Big Data for Personalized Diets
- Why Fiber Matters?
- Nutrition Week (Day 7) Connecting Epidemiology and Diet in Inflammatory Bowel Disease
- Life Cut Short by Obesity

