Methods: This was a retrospective single-center observational study which included children with IF and CVC who underwent GI endoscopy between 2019 and 2024. Intravenous antibiotic prophylaxis was used in 71.2% of the procedures.
Key findings:
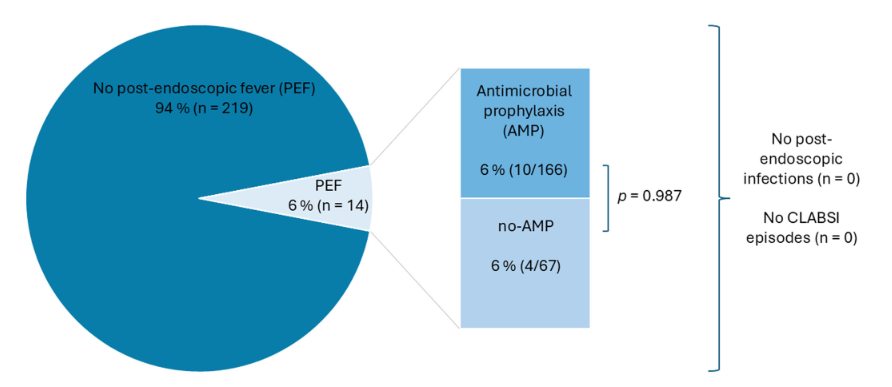
The overall post-endoscopic fever (PEF) rate was 6%, with no significant difference between the group that received prophylactic antibiotics and the group that did not. Specifically, there were 10 with PEF that had received prophylactic antibiotics and 4 that had PEF with no prophylaxis
No infections, including central line-associated bloodstream infections, were observed
5/14 of the cases with PEF had an interventional procedure. The remainder had a diagnostic EGD, colonoscopy or both.
Interventional Cases:
Discussion Points:
“PEF in children with IF was 6%, which is approximately 10 times higher than the recently published 0.55% in pediatric patients following endoscopic procedures by Boster et al.” (see: Must-Read: How to Handle Post-Procedure Fevers)
A strength of this study was that the comparison of children with IV antibiotics versus those without was due to an institutional policy change in 2022. This helps eliminate selection bias in the determination that IV antibiotics were not beneficial in preventing PEF
My take: The high rate (6%) of PEF should be discussed with families prior to endoscopic procedures. The rate was increased (36%) in those with interventional procedures. It is reassuring that no definitive infections were identified despite the fevers.
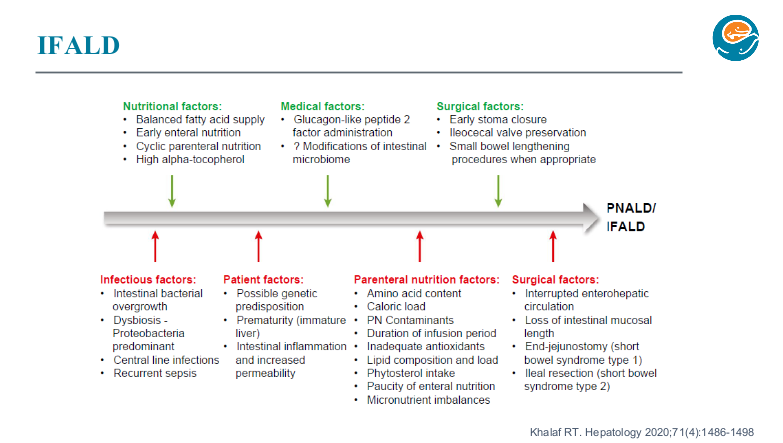
Background: “GLP-2 is a specific, endogenous, intestinal, pro-adaptive factor that plays a key role in enhancing intestinal mucosal morphology, function, and integrity under normal and pathophysiological conditions. The introduction of GLP-2 analogue treatment has been a paradigm shift in the treatment of SBS, targeting the pathophysiology of SBS by aiming to reinforce the structural and functional integrity of the remaining intestine. Exogenous GLP-2 induces significant hyperplasia of the small intestinal mucosal epithelium via stimulation of stem cell proliferation in the crypts and via inhibition of apoptosis in the villi…
The short half-life of 5–7 minutes for circulating native GLP-232 is a significant practical limitation for its use in a therapeutic setting. This is improved for the currently marketed GLP-2 analogue teduglutide, which has a half-life in circulation of approximately 2 hours.33 However, treatment is time-consuming due to the requirement for daily drug product reconstitution and dosing…
Glepaglutide is a novel, long-acting GLP-2 analogue in a stable, aqueous formulation for subcutaneous administration to treat patients with SBS. The stability in aqueous solution allows for dosing of glepaglutide as a ready-to-use liquid formulation. The mean effective half-life is 88 hours,34 which enables extension of the dosing interval beyond daily dosing.”
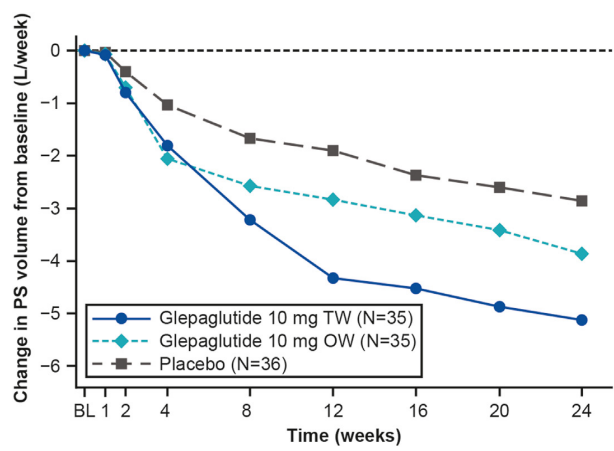
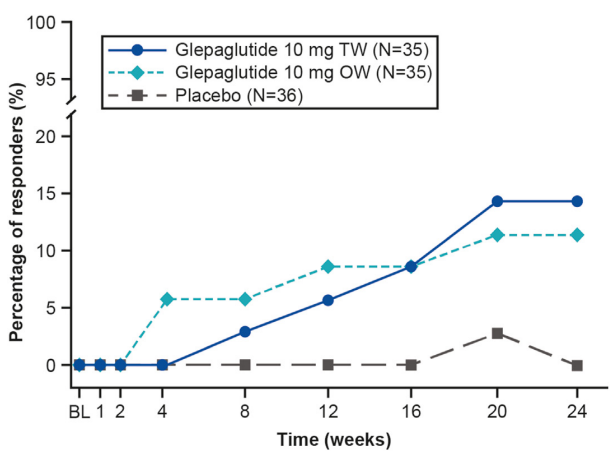
Methods: In this placebo-controlled, randomized, parallel-group, double-blind, phase 3 trial, adult patients (n=106) with SBS with intestinal failure requiring PS ≥3 d/wk were randomized 1:1:1 to 24 weeks of glepaglutide 10 mg twice weekly or once weekly or placebo
Key findings:
Glepaglutide twice weekly significantly reduced weekly PS volumes from baseline to week 24 vs placebo (mean change, −5.13 vs −2.85 L/wk; P = .0039; primary end point).
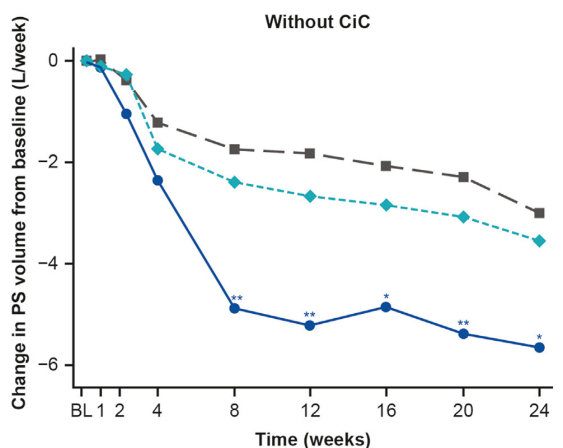
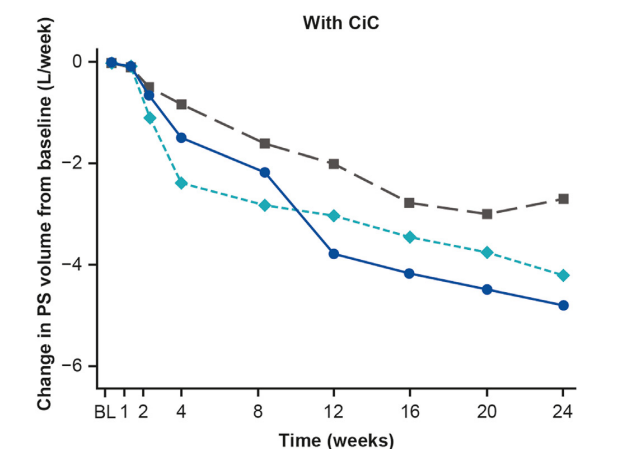
The improvement with glepaglutide was more prominent in those without a colon in continuity.
Mean concentrations of citrulline (a biomarker for enterocyte mass) increase 47% and 19% from baseline in the TW and OW treatment groups vs 5% in the placebo group
Serious adverse events were more common in both glepaglutide groups (28.6% and 11.4% for TW and OW respectively) compared to 5.6% for placebo. Specific risks of the active treatment included injection site reactions (common). Stoma complications (swelling of stoma nipple) along with GI events (nausea, vomiting and pain) were reported in more than 10% of patients. One patient developed cholecystitis and one developed a generalized rash in the active treatment group.
61 of 70 patients (87%) treated with glepaglutide developed anti-drug antibodies. However, the authors found no apparent association with glepaglutide pharmacokinetics.
The improvement in parenteral support was more notable in those without the colon in continuityDifference compared to placebo: 14.1% more of patients receiving twice weekly dosing and 11.2% more of patients receiving once weekly dosing of glepaglutide achieved enteral autonomy.
My take: This study shows that glepaglutide, like its GLP-2 analogue predecessor teduglutide, reduces the volume of parenteral support for patients with SBS. Due to its longer half-life, less frequent dosing is an added benefit compared to teduglutide.
Drawbacks for this group of medications include the potential for long-term adverse effects, endoscopic monitoring (possibly both upper endoscopy and colonoscopy), substantial costs, and reversion of intestinal failure severity when the medications are stopped.
This retrospective review identified 6 patients (out of 153) who were weaned off parenteral nutrition (PN) as part of an inpatient admission.
Key findings:
Except for one admission of 8 days, all of these patients required a prolonged admission 1-5 months.
Two of the patients were receiving PN primarily due to abdominal pain in the absence of a recognizable motility disorder.
Two of the patients had a suspected factitious disorder imposed on a medical disorder; one received this diagnosis.
All patients had chronic feeding intolerance despite favorable prognostic factors including underlying necrotizing enterocolitis (n=1), preserved ileocecal valve (n=5), longer bowel length (n=5), and retention of entire colon (n=5).
Post-pyloric feeds aided conversion to EN in 5 patients.
My take: In order to achieve enteral autonomy, hospital admission may be needed for patients who require long-term PN despite favorable prognostic factors.
Be prepared for a lengthy stay
Anticipate the need for an interdisciplinary team (eg. nutrition, social work, and others).
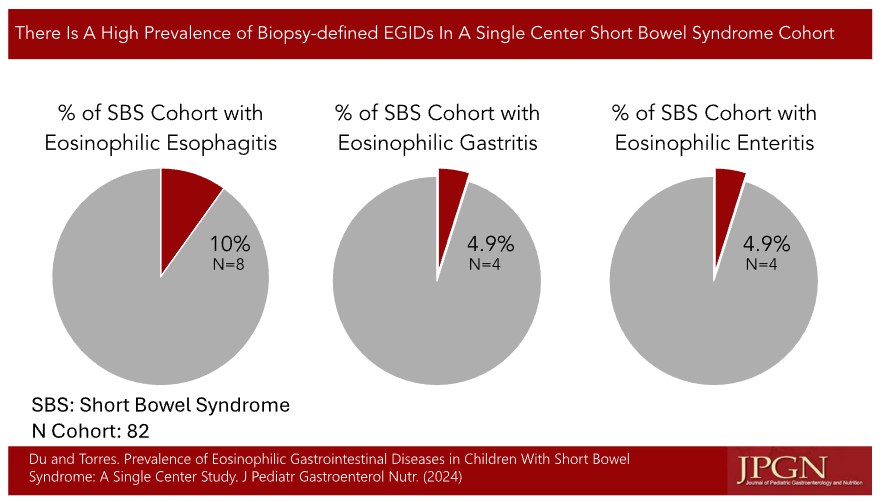
Methods: EoEdefined as ≥15 eosinophils per high powered field (HPF), eosinophilic gastritis (EoG) as ≥30 eosinophils per HPF, eosinophilic enteritis (EoGN) as >50 eosinophils per HPF, and eosinophilic colitis (EoC) as>80–100 eosinophils per HPF.
Key findings in this retrospective study (n=82):
The prevalence of eosinophilic esophagitis in our SBS cohort was10%, eosinophilic gastritis was 4.9%, and eosinophilic enteritis was 4.9%
SBS patients with history of allergy or atopy were more likely to have esophageal and intestinal eosinophilia on biopsy than patients without allergy
One patient had EoC
In their discussion, the authors speculate on the potential role for dysbiosis, possibly related to parenteral nutrition. They note that “rare SBS patients were on amino acid‐based formulas alone and almost all were exposed to food allergens around the same age as the general population.” I did not see any information about PPI use in this cohort.
My take: This report reinforces the fact that eosinophilic disorders are more frequent in SBS (see related post below). The exact role of altered diet/use of amino acid based formulas and the role of medications like PPIs in regards to the development of EGIDs remains unclear.
We had an brilliant lecture given to our group by Danielle Wendel who leads Seattle Children’s Intestinal Rehabilitation team. My notes below may contain errors in transcription and in omission. In addition, the information provided is based on what is done in Seattle. However, there is not a lot of evidence for much of what is done in intestinal rehabilitation. Thus, there is variation in practice at different centers and what works for one patient might not work for another. Following my notes, I have included many of her slides (same slides as yesterday’s post).
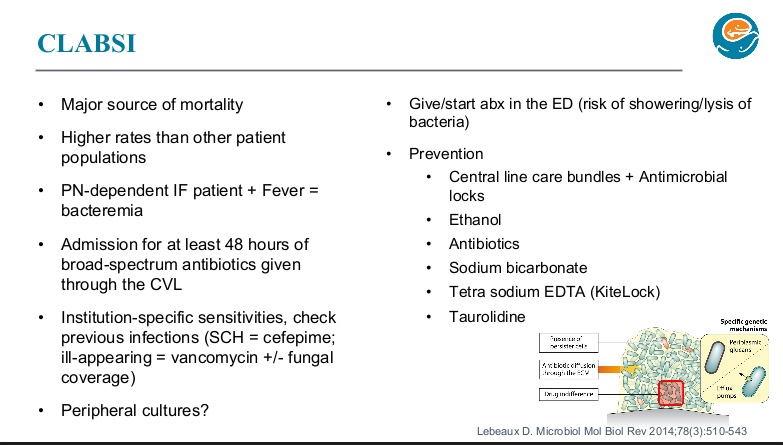
CLABSI Pointers:
-At Seattle, with suspected CLABSI, usually central blood culture obtained without peripheral blood culture. (Peripheral blood cultures have not helped their team improve management)
-Everyone with SBS and with fever (greater than or equal to 100.4) stays for at least 48 hrs on broad spectrum IV antibiotics (choice based on local sensitivities) through the central line until it is conclusively determined if they have a CLABSI (which still carry a significant mortality risk)
-Sodium bicarbonate lock experience has been good (8.4% solution, 1.5 mL lock for the entire time off PN in all tunneled CVL flushed in at the end of the dwell). It has become a good substitute for ethanol locks. Their experience will be published soon. Since sodium bicarbonate lock does not need to be withdrawn, it has been associated with less line breakage. Several lock solutions (KiteLock and Taurolidine) are not currently available in the U.S. KiteLock is about to be studied in Seattle.
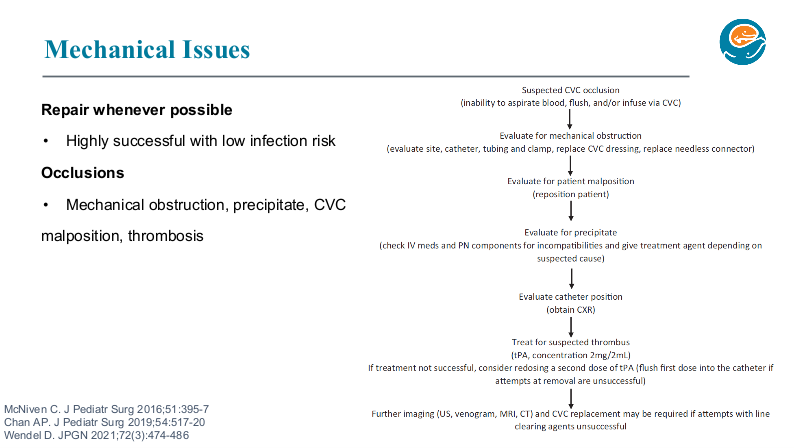
-At Seattle, all CLABSI are treated through the line and every effort is made to salvage and/or repair lines. Line replacement increases risk of losing central IV access.
-Line is removed for fungal infections
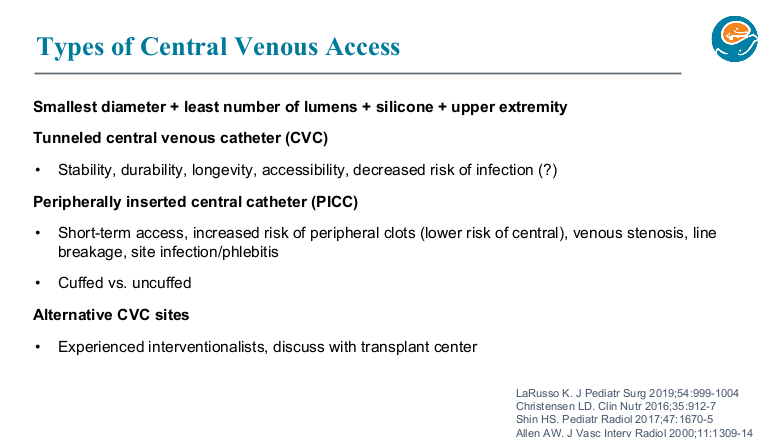
-The Seattle team prefers tunneled CVC
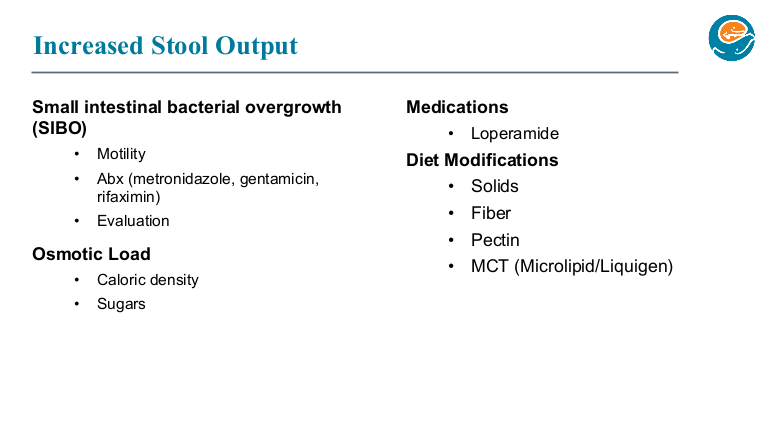
SIBO Pointers:
-Testing is problematic. Breath tests are not reliable in kids with SBS. Duodenal aspirates are often not helpful and have a number of technical difficulties; also, it is unclear whether a duodenal aspirate is representative of the bacteria in the more distal bowel.
-Metronidazole is their first line choice. Gentamicin (IV formulation given enterally) is their 2nd choice. Rifaximin is their 3rd line. Rifaximin would possibly be used earlier in treatment except for difficulty getting covered. When used, they crush up pills rather than have it compounded to avoid sweeteners.
Teduglutide
-Best to start if a patient is is > 1yo and on stable TPN (not able to wean)
-Make sure patient is using a tiny needle (not adult needle in package)
-Anticipate long-term treatment (?indefinite)
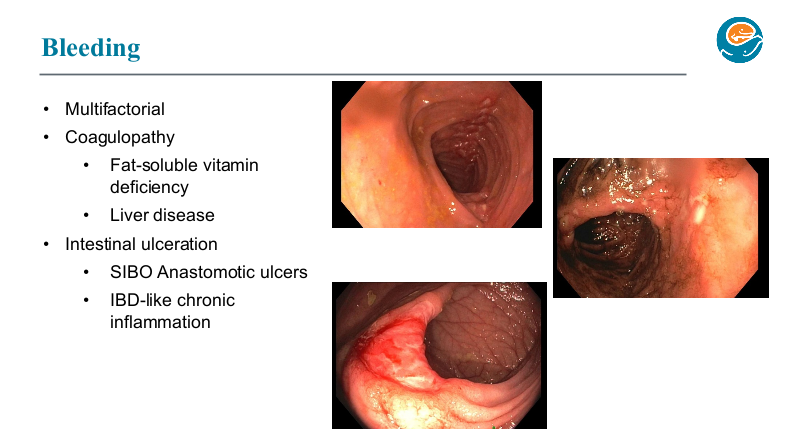
GI Bleeding Pointers:
This is being seen frequently.
Etiologies include anastomotic ulcers and IBD-like lesions. If a patient is not improving with standard approaches and possibly resection, could need an anti-TNF type agent.
At Seattle, they are very selective about patients appropriate for a STEP procedure as this may be associated with more frequent bleeding over time due to the many staples used. Hand-sewn tapering may be a better option for many patients.
With the challenging decisions required for these bleeding patients, discussion with an experienced intestinal rehab center may be helpful.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
We had an brilliant lecture given to our group by Danielle Wendel who leads Seattle Children’s Intestinal Rehabilitation team. My notes below may contain errors in transcription and in omission. In addition, the information provided is based on what is done in Seattle. However, there is not a lot of evidence for much of what is done in intestinal rehabilitation. Thus, there is variation in practice at different centers and what works for one patient might not work for another. Following my notes, I have included many of her slides.
Key points:
Enteral nutrition is key for adaptation. At Seattle, oral feeds rather than GT feeds are preferred.
Time is the thing that helps the most. Unclear which additives help.
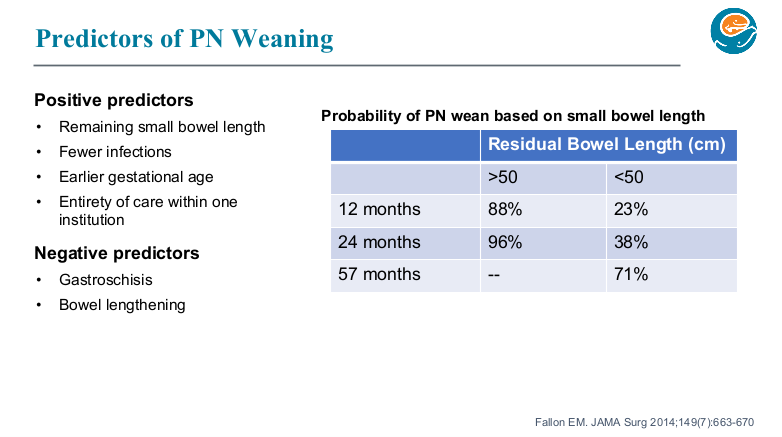
Though prediction models often look at >50 cm, it is important to counsel families, even with more bowel length, that the care is going to be quite challenging.
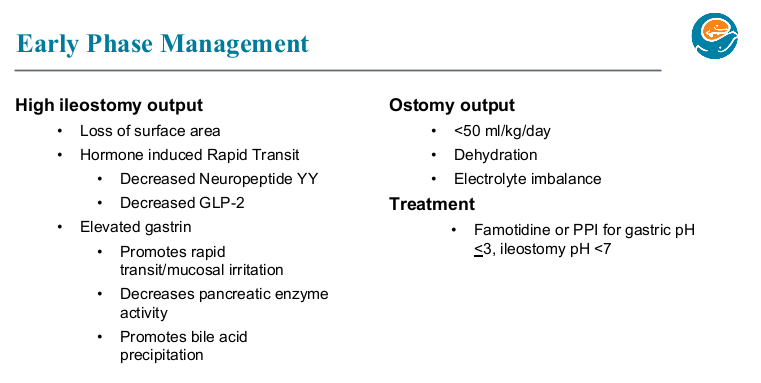
Acid suppression can be helpful in the early phase after resection especially if problematic high stoma output.
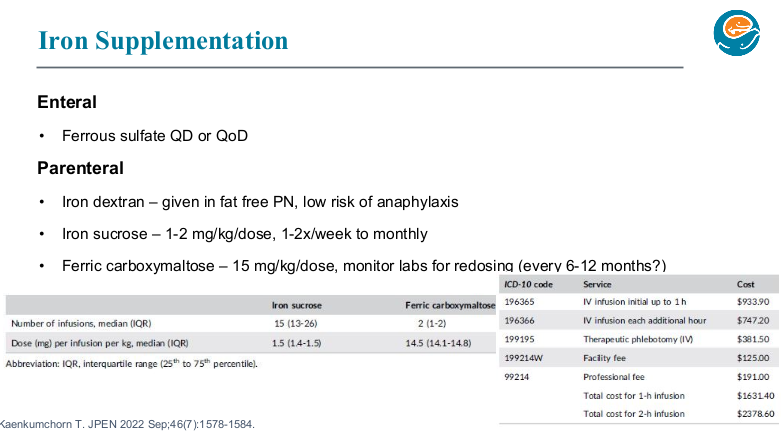
Iron: if given enterally, typically given everyday or every other day. Iron dextran can be given in TPN (cannot be given with lipids). Ferric carboxymaltose is a good choice for parenteral administration. Due to the need for few infusions (~1-2 per year), it is safer (less line entry) and cost-effective compared to iron sucrose.
Seattle shares an “Emergency Care Letter” with their patients (template available in EPIC)
Yearly doppler ultrasound is recommended to assess vascular access.
If a patient has more than one thrombosis, the Seattle team recommends long term prophylaxis, though it might take treatment levels to prevent further thrombosis.
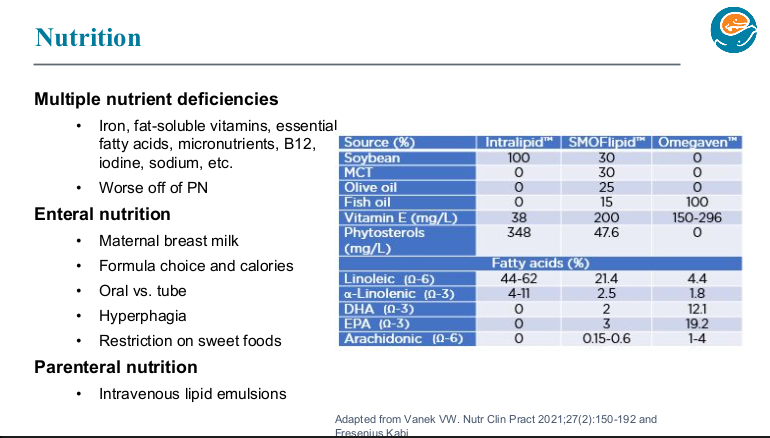
SMOFlipid is the most frequently used lipid at Seattle. It can be given in higher doses than Omegaven which is important nutritionally; omegaven is generally given at only 1 to 1.5 mg/kg/day and used for treatment of IFALD.
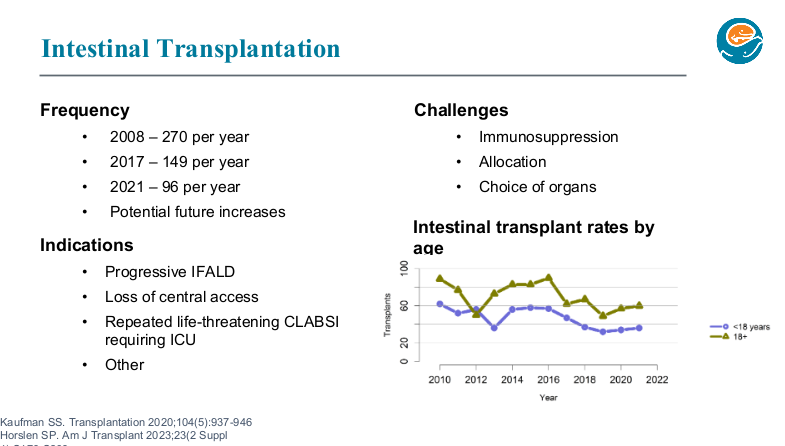
Long term outcomes are just as good with chronic TPN as with intestinal transplantation. So, referral generally needed based on complications like losing central access (3 of 4 upper central sites) or progressive liver disease.
Diet Pointers:
-In infancy, standard formula and breastmilk are preferred and thought to help with adaptation. Some infants need elemental diets but it is not routinely given across the board (some other institutions feel strongly about using elemental diets, but there is limited data)
-Kids with short bowel syndrome may tolerate volume better than concentration
-The Seattle program strictly restricts sweet tasting food/drink for first 3-4 years of life to help educate the child’s palate and recommends limiting these food/drink for IF patients in general.
-Addition of solid foods usually helps with stoma output
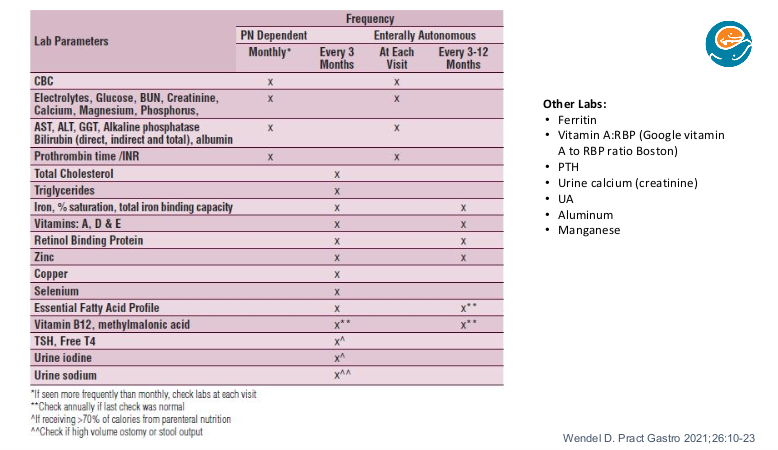
Nutrient Monitoring Pointers:
Usually best to batch them all lab tests for micronutrients [many micronutrients are affected by inflammation and this may affect timing of lab testing]
At Seattle, aluminum and manganese are not routinely checked as they are contaminants in PN that cannot be removed
Serum thyroid testing is a marker for iodine deficiency in patients receiving most of their calories from PN (>70) which may be more frequent now that betadine is not used for dressing changes. Their goal for urine iodine is >100 (can be treated with ultra-diluted potassium iodide which needs to be compounded by the pharmacy)
When testing for EFA (essential fatty acid) deficiency, lipids should be off for 4 hrs (or more). Urinalysis is checked to monitor for chronic kidney disease. Urine sodium goal is >30 and is checked quarterly in patients with high ostomy output or excessive rectal stool output with poor growth.
Hypokalemia may be a sign of total body sodium depletion due to the kidneys dumping potassium to conserve sodium
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
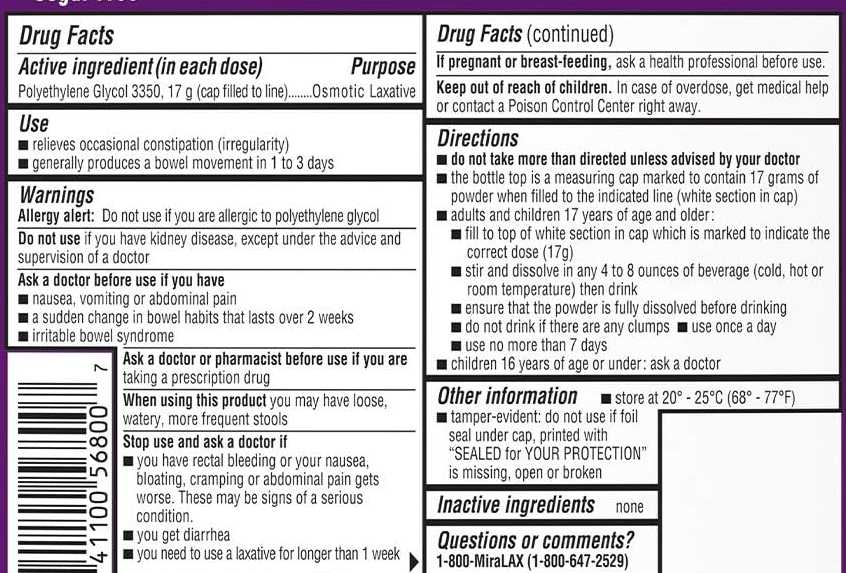
Clarification: Yesterday’s post on the safe use of polyethylene glycol (Long Term Use of Polyethylene Glycol (PEG 3350)) noted the labeling indicates “‘to not use these medications for more than 7 days.” However, Ben Enav pointed out that the label also states the following in bold: “do not take more than directed unless advised by your doctor.” The actual label is shown below.
Methods: The authors used the PediatricHealth Information System (PHIS) database to evaluate associations between neighborhood income and hospitalization data for children with short bowel syndrome (SBS). This included 4289 children with 16,347 hospitalizations from 43 institutions.
Key findings:
2153 of the 4289 (50%) patients were readmitted during the study period (2006-2015)
Children living in low-income neighborhoods were more likely to be Black, Hispanic, have public health insurance, and live in the Southern U.S.
Children from low-income neighborhoods had a 38% increased risk for all-cause hospitalizations (rate ratio [RR] 1.38), an 83% increased risk for CLABSI hospitalizations (RR 1.83) and increased hospital length of stay.
2.4% of patients in this cohort experienced 10 or more CLABSI hospitalizations
One of the study’s limitations is that ‘there is no singular ICD-9 code for SBS.’
My take: It is speculation about the reasons why children in low income neighborhoods have higher rates of hospitalizations and CLABSI hospitalizations. It could be that more parents in these households have less time and resources to manage a child with SBS. It is possible that these households have more chaotic environments. Regardless of the reason, it takes a lot of work and meticulous care to prevent CLABSI hospitalizations in children with SBS.
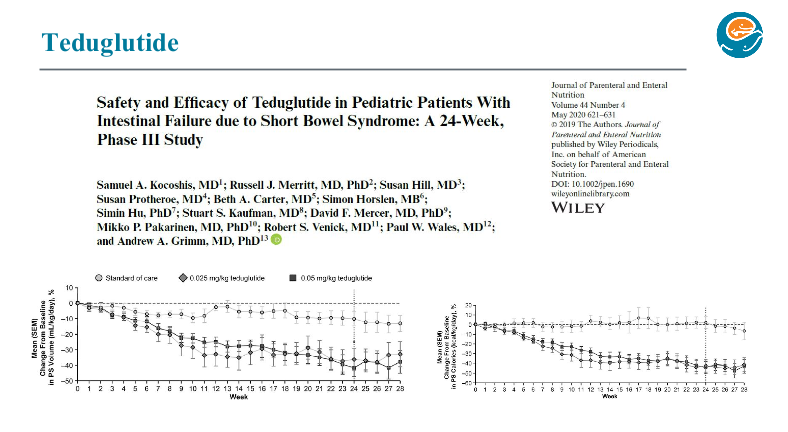
I have not been an enthusiastic early adopter of teduglutide. Though it has been shown to reduce HAL volumes in those with short bowel syndrome (SBS), this tends to revert with cessation of treatment. In addition, it has a very high cost and long-term adverse effects are unclear. Currently the manufacturer recommends a colonoscopy after 1 year of treatment.
This case report by Salazar et al identified two children who developed foveolar hyperplastic gastric polyps after receiving teduglutide.
Discussion points:
“There have been increasing reports of both benign and malignant small bowel polyp development. In trials of pediatric patients, limited to 12 and 24 weeks, initial upper endoscopy and colonoscopies were not required. In addition, postexposure upper endoscopy and colonoscopy was not the standard of care (9,13,16). Thus, the incidence of intestinal polyp formation on teduglutide treatment in pediatric patients remains unknown.”
“A recent retrospective review of adult patients with SBS showed increased small bowel polyp formation in 8 out of 35 patients (22.9%) on long-term teduglutide use… 3 were identified as adenomas with low-grade dysplasia… (14)”
“In general, isolated foveolar hyperplasia has not been identified as a premalignant lesion…The connection between foveolar hyperplasia and development of dysplasia, though, remains poorly understood, and further work delineating the natural history of foveolar polyps in the context of teduglutide is important.”
Related article: A Fifi et al. JPGN 2023; 77: 666-671. This is a post-hoc analysis showing improving stool consistency in 101 patients treated in open-label studies. Patients had mean drop of 20 mL/kg/day in parental fluid volume (compared to 7 mL/kg/day in the standard care treatment group).
My take: This case report indicates that endoscopic monitoring (possibly both upper endoscopy and colonoscopy) is needed in teduglutide-exposed patients. In addition, careful consent of the patients is prudent indicating the uncertain long-term effects. Finally, it would be a good idea to enroll all patients in a registry as well.
Jeff Lewis, one of my colleagues for the last 25 years, recently shared a story on The Moth Atlanta. For those of you who have not been to The Moth, you can hear many of these stories on NPR (The Moth Radio Hour) or The Moth Podcast. Each session has a topic and 10 people are invited to share their heartfelt and sometimes hilarious stories.
Jeff is a brilliant, innovative individual and a good friend. Some of his diverse accomplishments include helping start a camp for our celiac patients (Camp WeeKanEatit), starting our microbiome transplant program (FMT), advancing the health of special needs kids (given an award for this by the Georgia Department of Public Health) and starting a lecture series to honor our surgical colleague Donald Schaffner. He even prompted changes in the hospital’s advice line. In addition, he has been instrumental in making the business part of our office work and in initiating a whole host of research projects. One of his children has told me that Jeff has a calling as a clinician which is so true.
My take: It would be a great idea to have a Moth-type session at our national meeting. I enjoy listening to these stories particularly on long trips.
Per google search: “The Moth was founded in 1997 by the writer George Dawes Green — its name comes from his memories of growing up in St. Simons Island, Ga., where neighbors would gather late at night on a friend’s porch to tell stories and drink bourbon as moths flew in through the broken screens and circled the porch light.”
This retrospective study (n=263) examined the rate of venous thromboembolism (VTE) in pediatric patients who required parenteral nutrition for at least 90 consecutive days.
Key findings:
The cumulative incidence of VTE was 28.1%, with a rate of 0.32 VTEs per 1000 catheter-days
The number of catheters and early gestational age were noted to be independent risk factors for VTE
No patients had progression of thrombus while receiving therapeutic anticoagulation
Of those with acute DVTs (n=47), 24 (51%)resolved on repeat imaging, 14 (30%)were stable, and and 9 (19%) had decreased
4.4% (2 of 45) had a major bleed while on anticoagulation
The authors note that the true rate of VTE is likely even higher because only 42% categorized as not having a VTE had undergone dedicated venous imaging.
My take: A lot of patients with intestinal failure develop VTE. Given the risks of treatment, the role of prophylactic anticoagulation remains unclear. This is where a prospective study would be helpful.