Our local CCFA chapter provided a useful physician CME meeting. The following are my notes. My notes may include some errors in transcription and errors of omission.
Ashish Patel -Updates in Pediatric Inflammatory Bowel Disease Treatments
Key points:
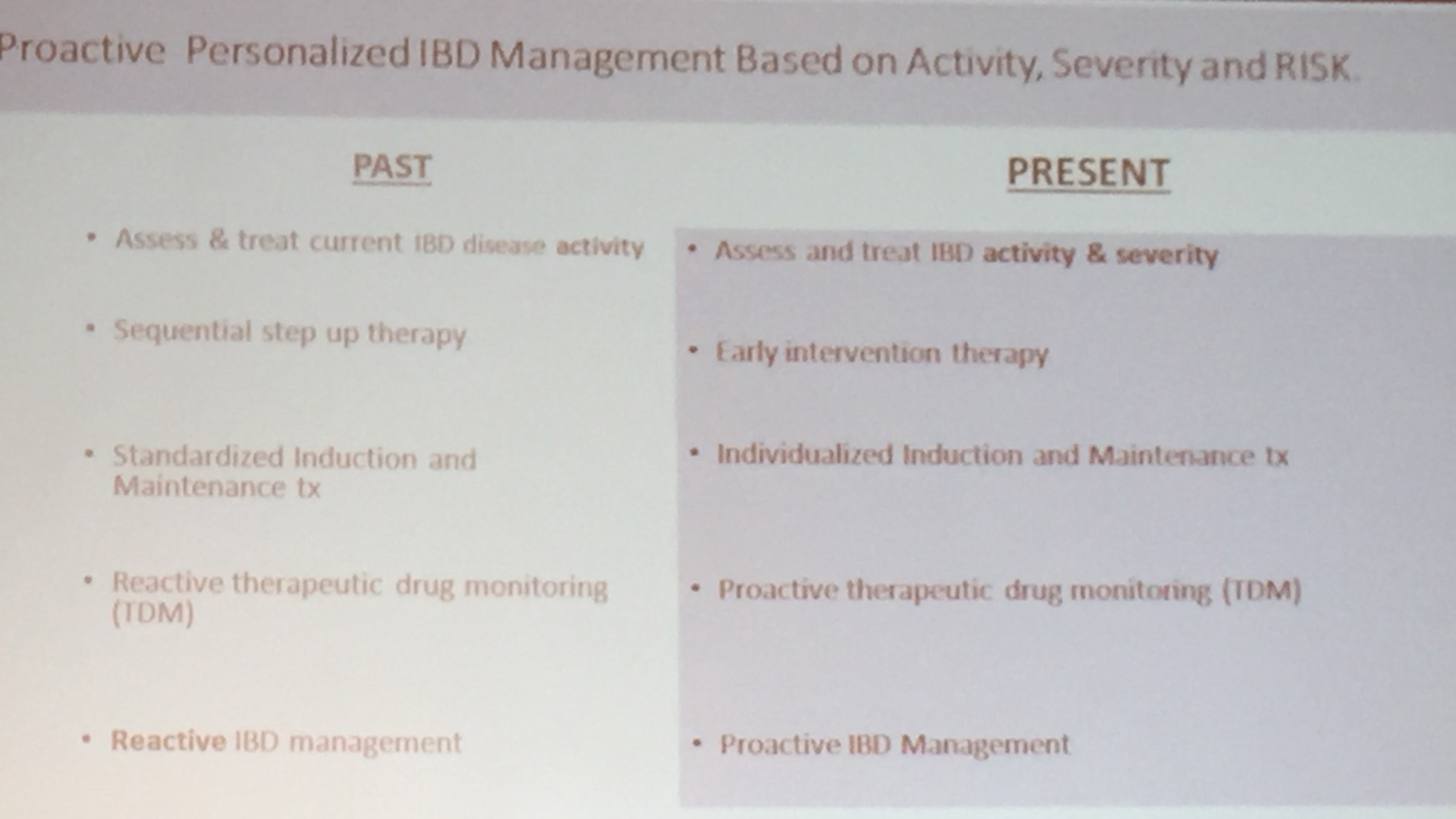
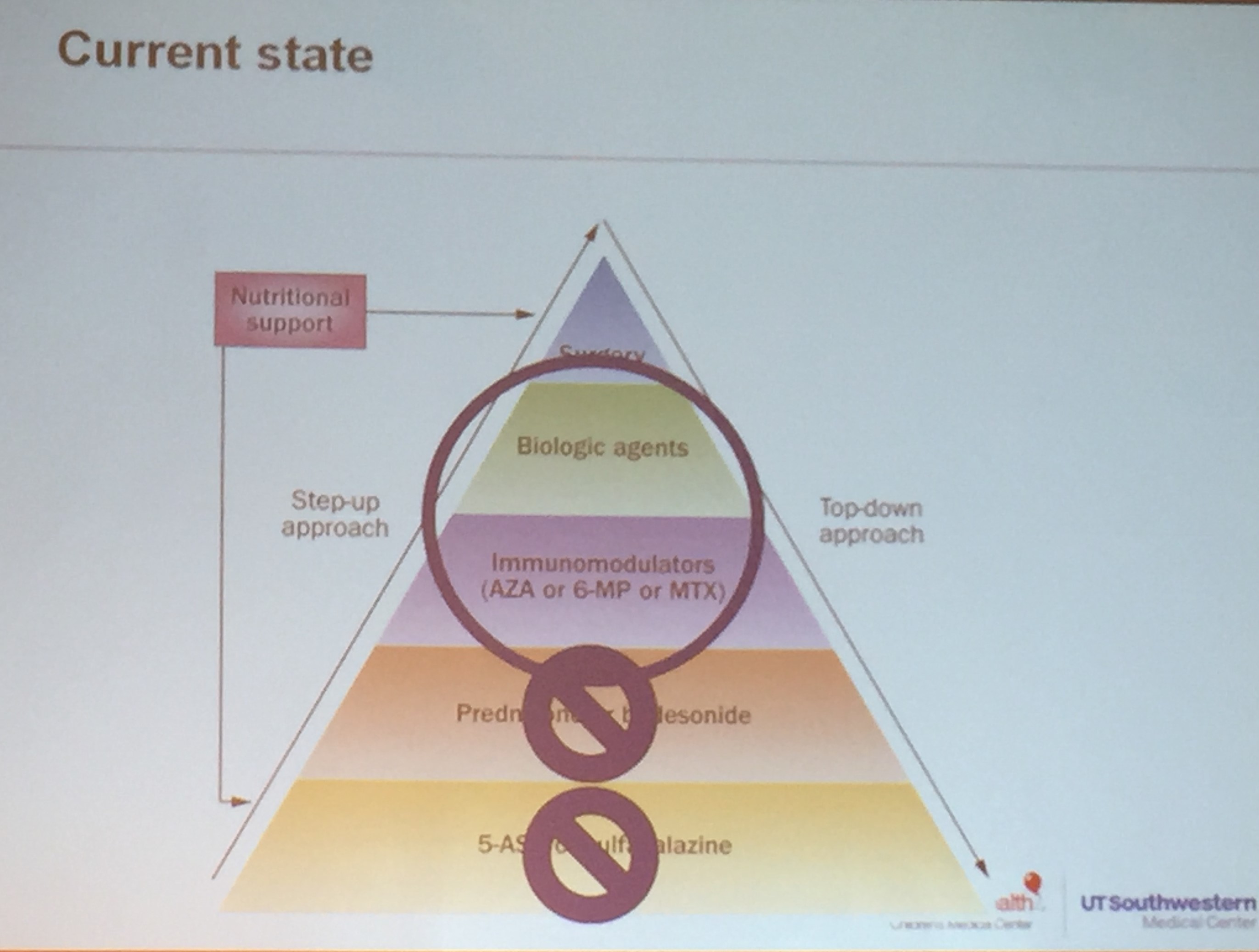
- Top-down or step-up models are outdated –use appropriate agent for each patient
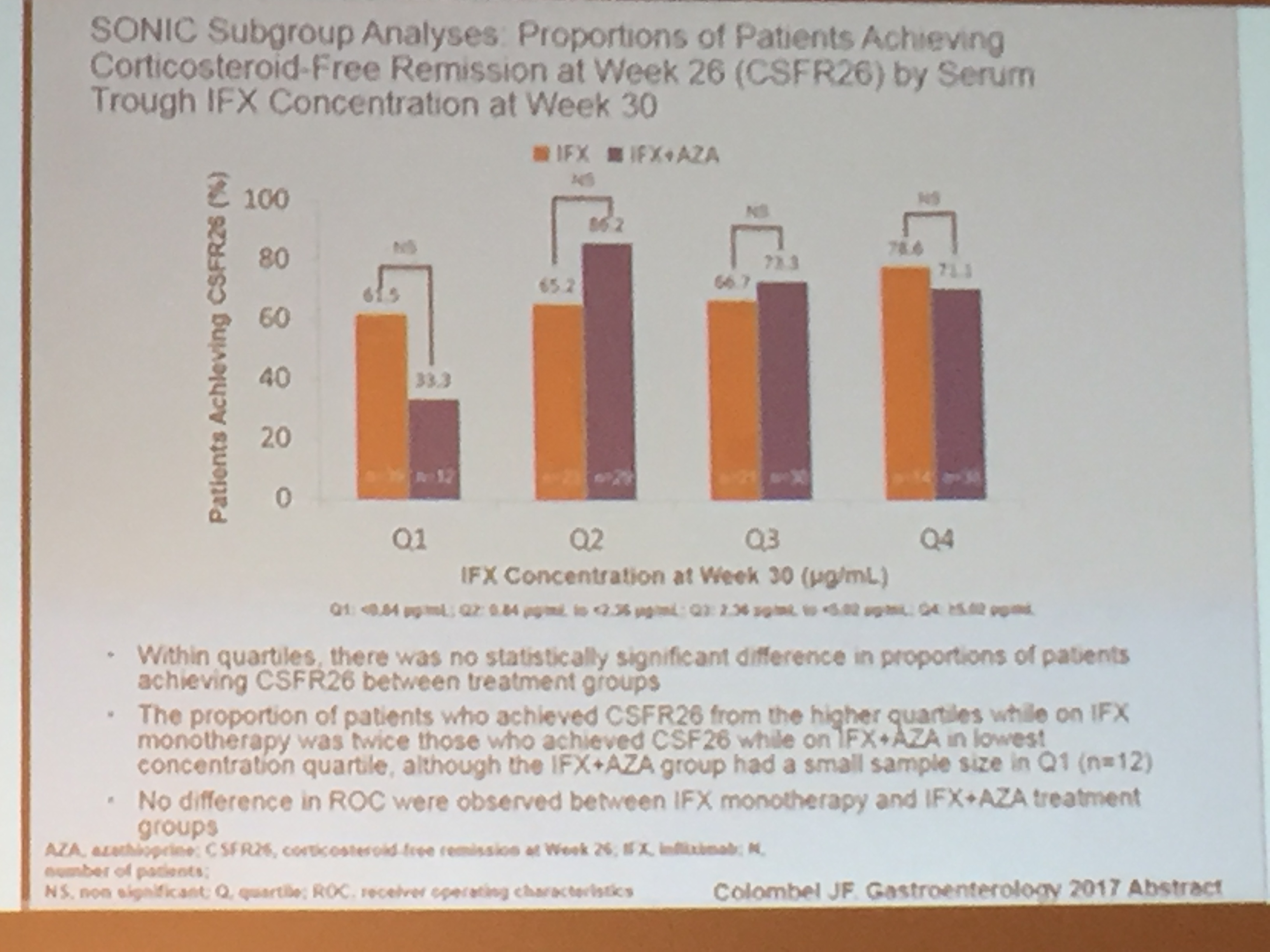
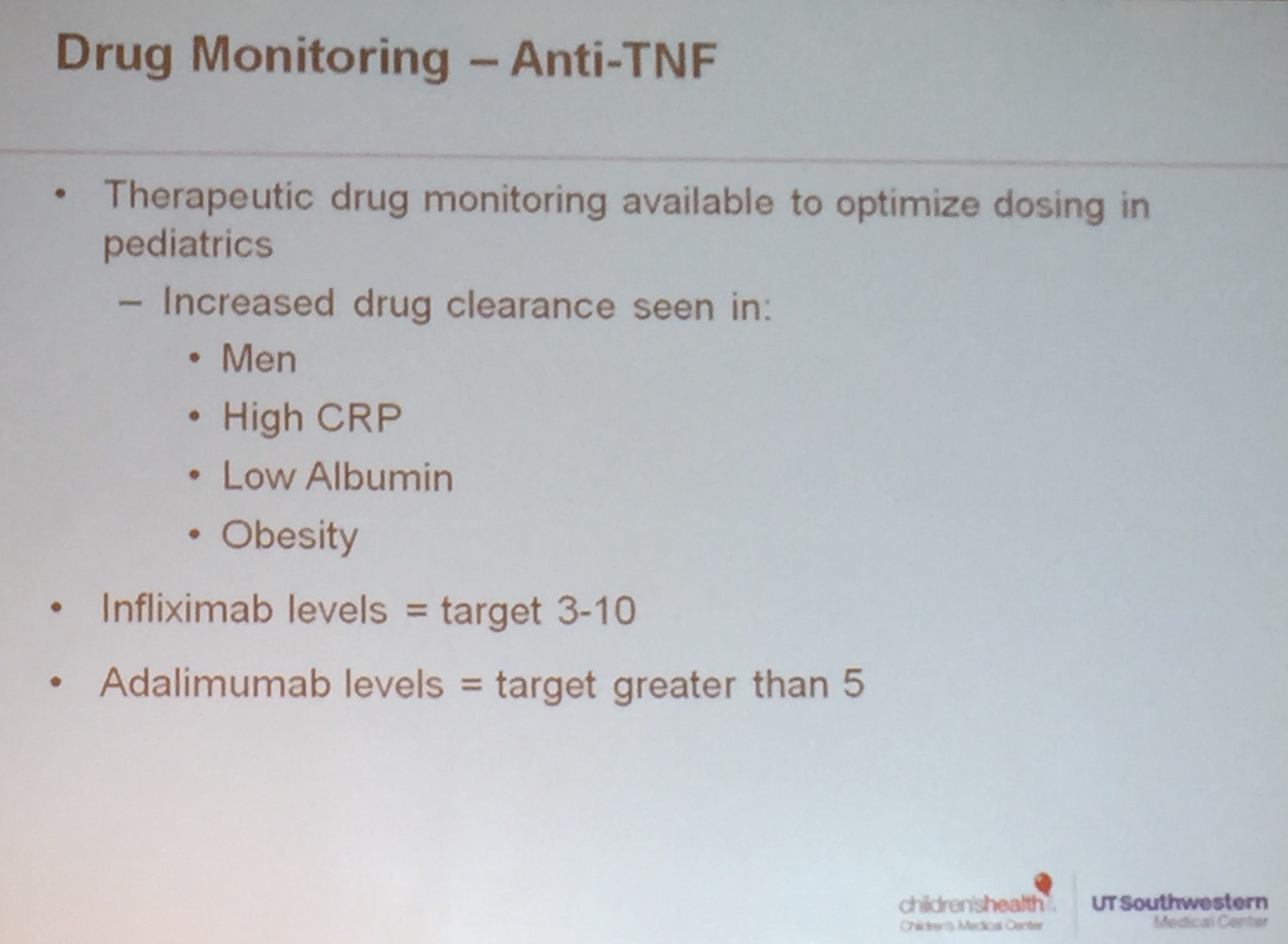
- Discussed therapeutic drug monitoring. In pediatrics, checking infliximab (IFX) level after 14 weeks is recommended by ICN per Dr. Patel.
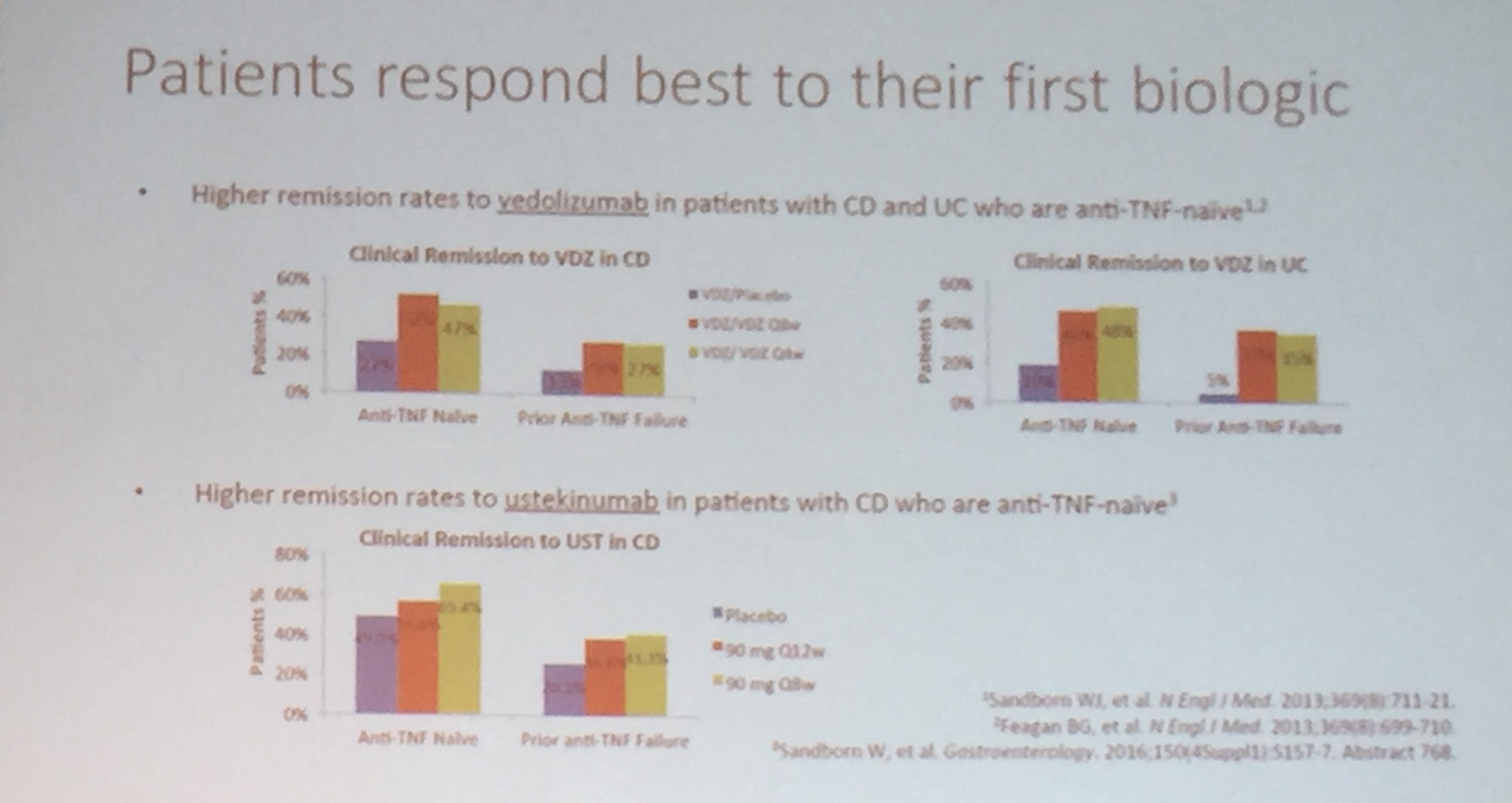
- Veolizumab -no pediatric FDA indication yet.. Alpha4Beta7 integrin blocker –blocks recruitment of WBC
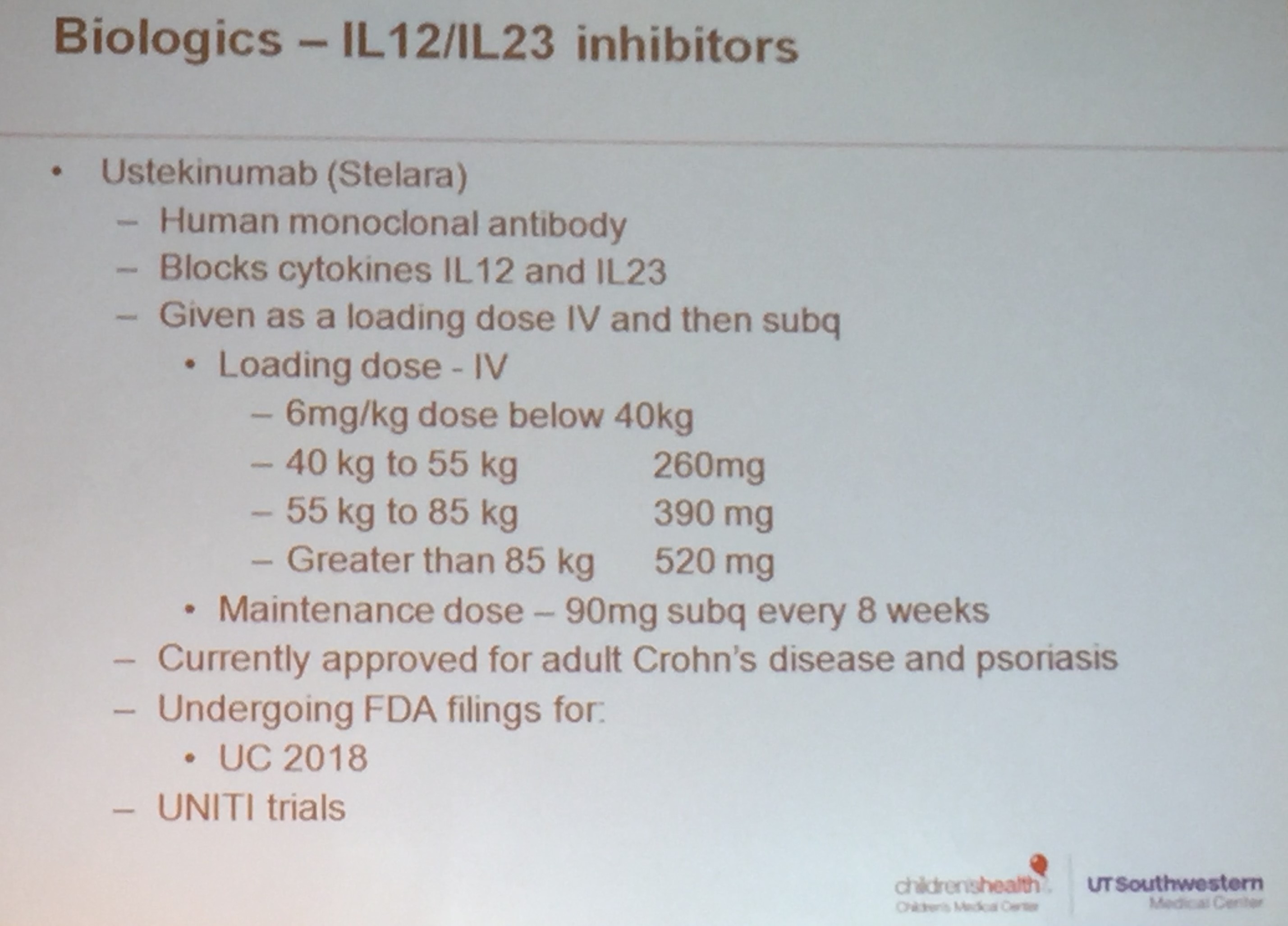
- Stelara -off label in pediatrics. Seems to be helpful for patients who have psoriasis on TNF agents.
- Exclusive enteral nutrition (EEN) like medical therapies are therapies and not cures. It has to be maintained to be effective.








Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) and changes in diet should be confirmed by prescribing physician. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.