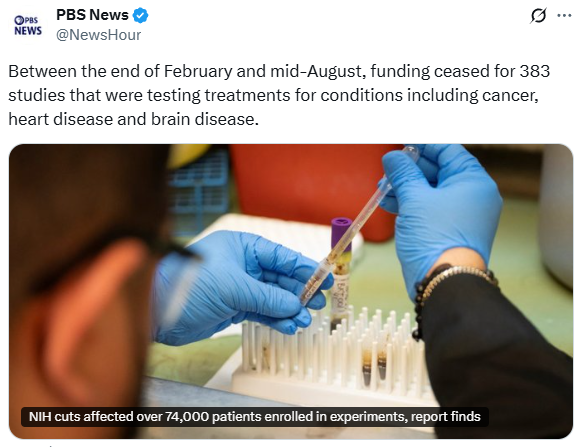
Between the end of February and mid-August, funding ceased for 383 studies that were testing treatments for conditions including cancer, heart disease and brain disease. The cuts disproportionately impacted efforts to tackle infectious diseases like the flu, pneumonia and COVID-19, researchers found…
More broadly, the lost research harms patients who could have benefited from a possible new treatment, researchers said in the report published Monday in the journal JAMA Internal Medicine…
“The whole purpose of these clinical trials is to generate evidence on what works and doesn’t work in medicine,” said study co-author Anupam B. Jena with Harvard Medical School. Researchers counted 11,008 NIH-funded studies during the study period. Of those, 1 in 30 lost funding.
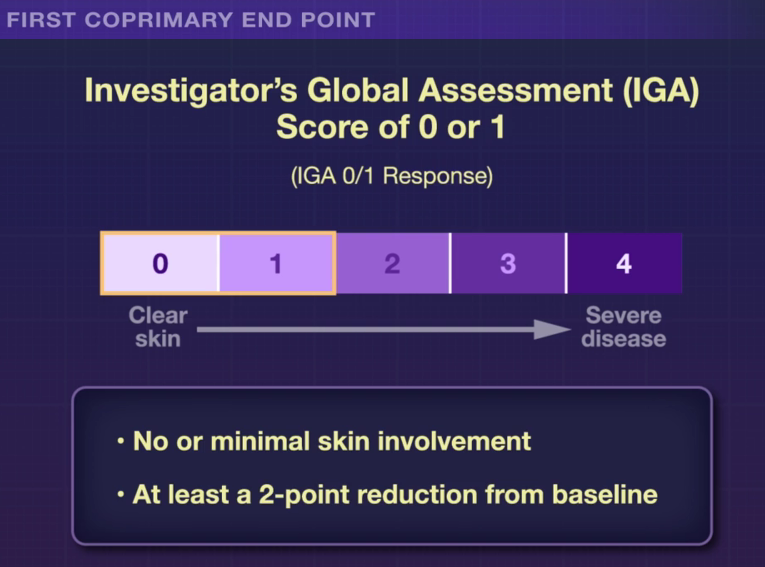
R Bissonnette et al. NEJM 2025; 393: 1784-1795. Oral Icotrokinra for Plaque Psoriasis
RS Stern. NEJM 2025; 303: 1854-1855. Oral Psoriasis Therapy — For Whom and at What Cost and Risk?
S Wharton et al. NEJM 2025; 303: 1796-1806. Orforglipron, an Oral Small-Molecule GLP-1 Receptor Agonist for Obesity Treatment
In the ICONIC-LEAD study (Bissonnette et al), 684 adolescents and adults participated in a DBPC trial with an oral peptide, icotrokinra, which binds the IL-23 receptor. This medication is of interest as there are ongoing trials with it for inflammatory bowel disease. Other injectable medications targeting IL-23 are already approved for IBD.
Key Findings:
The associated editorial notes that this new therapy is likely to cost ~$70,000 per year. The cost of psoriasis care has increased more than 2000% since 1997. “Because of these high prices, rebates and discounts to pharmacy benefit managers that often guide formulary preferences are likely to govern clinician’s selection of immune-based oral and parenteral therapies for psoriasis.”
In the ATTAIN-1 Trial (Wharton et al), the authors share the results of an oral GLP-1 Receptor Agonist, Orforglipron, monotherapy for obesity.
My take: There are similar injectable alternatives to each of these medications for psoriasis, obesity and diabetes. The availability of oral medications could reduce one barrier to treatment. Cost barriers may preclude their use in many patients when they become available. In addition, long-term outcome data are still needed.
This article reviews the growing health concerns regarding microplastics and nanoplastics (MNPs) specifically regarding the GI tract.
Key points:
“As these [plastic] products degrade, they break down into smaller particles, forming microplastics (< 5 microm) and nanoplastics (<1 microm), collectively referred to as MNPs”
“Although many plastic products are deemed recyclable, in the United States, less than 10% are actually recycled…annual global production projected to reach 1.1 billion tons by 2025. Simultaneously, over 12 billion tons of plastic wastes are expected to accumulate in landfills”
“The average American ingests approximately 5g of plastic per week, equivalent to 1 credit card, and 39,000–50,000 particles annually”
Potential association of MNPs with metabolic-associated steatotic liver disease, liver and pancreatic cancer and inflammatory bowel disease. “Studies have reported significantly higher levels of MNPs in patients with IBD compared with healthy controls.”
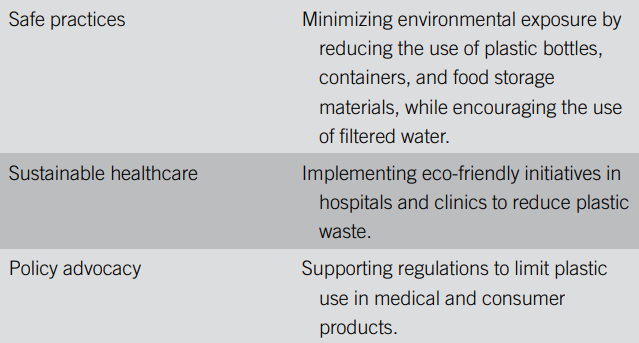
In a related article in Gastroenterology and Endoscopy News (October 2025), Dr. Johnson noted that “reduction of plastic intake from bottled water to tap water in one study reduced microplastic intake, the number of particles within human tissues, from 90,000 to 4,000…Avoid heating food in plastics…the effect of microwave increased the evidence of microplastics by over 4.2 million and the nanoplastics, 2 billion, just in three minutes in the microwave.”
My take: Something that almost everyone could agree on – they would like less plastic in their food and environment. How to achieve this is much more difficult.
EJ Shapiro. NEJM 2025; 393: 1360-1361. “You Still Going to be Doing This?”
This commentary mirrored a lot of my recent experience. The author is startled at how patients are asking if he will still be taking care of patients in a few years and how he has enjoyed being a clinician.
Here is an excerpt:
At first, I was startled — I’d never seriously considered the timeline of my own career…Whether it was thanks to luck, sound reasoning, some resolution of my cognitive dissonance, or (least likely) an easy disposition, I mostly enjoyed the ride. Medical school flew by…every rotation opening a new world…As a resident, then a fellow, I learned the delicate balance between personal responsibility and teamwork required in caring for patients facing the range of problems…
Then…I …realized that my opinion — no discussion with the team, no attending cosignature, just mine alone — would guide this patient’s care… So many lives shared, some with laughter, less often with tears. Many of them I helped, and some I probably didn’t…
I realize the time has come to try to figure out the answer to, “Are you still going to be doing this?” But the decision doesn’t come easily. On a day-to-day basis, I love what I do, mostly because of the connections with those patients, and the nurses, techs, secretaries, medical assistants, and my partners (some of whom are now in my children’s age group). Also because medicine always changes and always fascinates.
Of course, prior authorizations, electronic medical record snafus, obtuse hospital administrators, and sometimes the clinical demands can feel oppressive… But… when I go into the exam room, close the door, greet the patient, and begin our visit, none of those structural irritants matter. We explore their situation and try to figure out how to move forward. The challenge and respect of that task never really pale…
Still, all the other passions, affections and hobbies, grandchildren, books, and mountains call out…And… I’d rather go when the reaction from the people left behind will be regret rather than relief…
I still have some things to consider before I put that full stop on my medical career, but maybe at some point the choice will become clear — like the one that long ago began it. Everything has its season.
My take: Though I am not ready to retire, I am getting the question from families about when I might and have started to think about the next season.
The AAP and more than 40 other medical, health and patient advocacy groups also issued a joint statement condemning the change and called on the CDC to “return to its long history of promoting evidence-based information.”
Potential links between vaccines and autism have been studied for decades. More than 40 high-quality studies in seven countries involving over 5.6 million people have found no connection.
“The conclusion is clear and unambiguous: There’s no link between vaccines and autism,” Dr. Kressly said. “Anyone repeating this harmful myth is misinformed or intentionally trying to mislead parents.”
Scientists believe there is no single root cause of autism. Interactions between genetic changes and environmental influences likely play a role, according to an AAP Fact Checked article. Improved awareness and screening and updated diagnostic criteria have contributed to increases in autism prevalence.
“At this point, it’s not about doing more studies. It’s about being willing to accept what the existing studies clearly show,” said Alison Singer, M.B.A., co-founder and president of the Autism Science Foundation.
She said spending more money on settled science takes funding away from research on genetics and services for autistic people. False claims further stigmatize autistic people and their families…
Sean T. O’Leary, M.D., M.P.H., FAAP, chair of the AAP Committee on Infectious Diseases, called the latest move to put misinformation on the trusted CDC website “madness” and “a tragic moment for this country” and said he does not blame the career CDC scientists.
“For many decades, we (could) rely on CDC to provide the American public with the best available science,” Dr. O’Leary said. “Now our government is using it as an apparatus to spread falsehoods and lies.”
Here is a screenshot on media coverage of this story:
Recently, Dr. Jennifer Lee gave our group an excellent update on artificial intelligence (AI) for pediatric gastroenterology. My notes below may contain errors in transcription and in omission.
AI is ubiquitous -it helps you login into your phone, helps with traffic apps, filters spam from email, and even edits Bowel Sounds (gets rid of the ‘umms’)
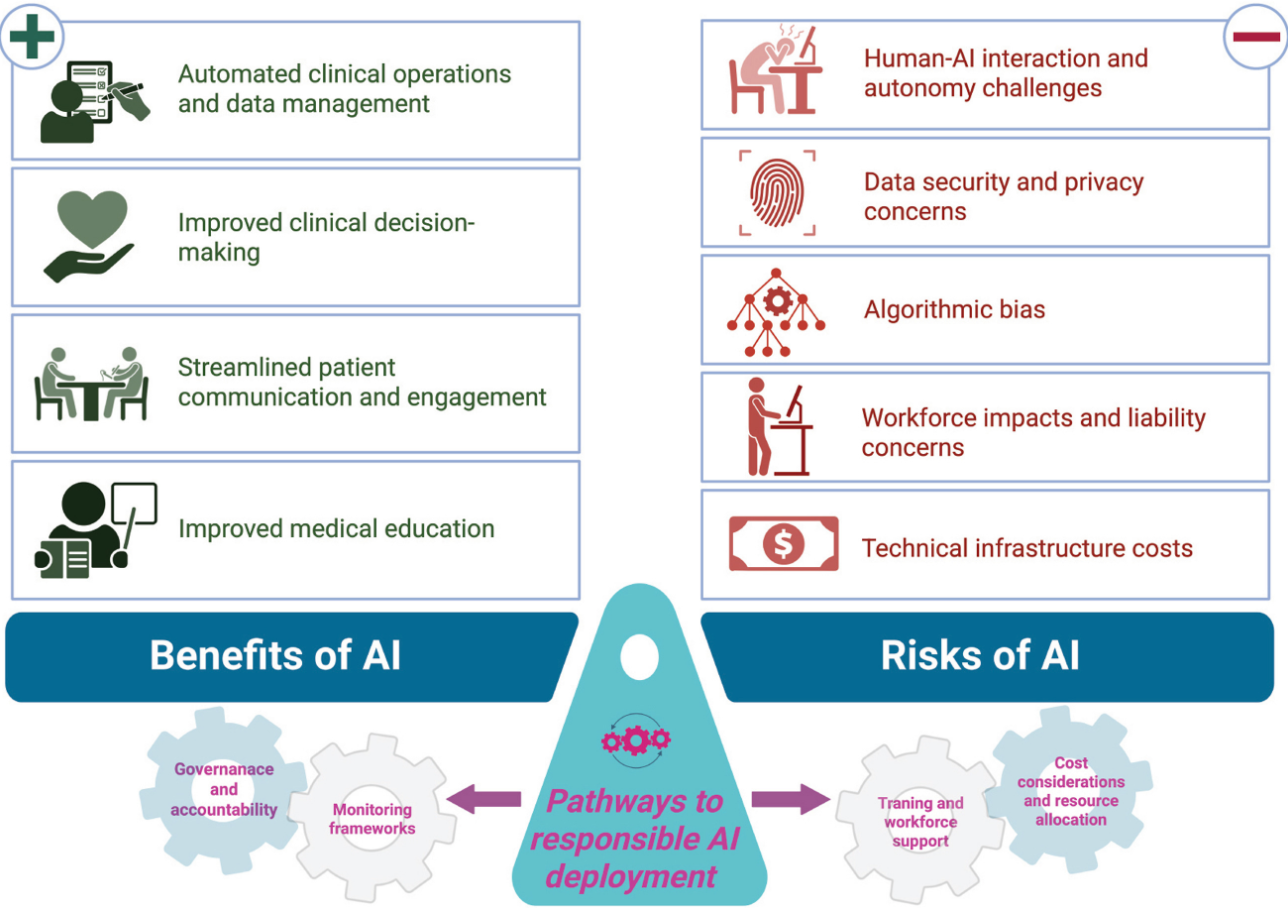
AI can help and AI can harm
Dr. Lee thinks that AI is not going to replace doctors and may help doctors in their clinical work
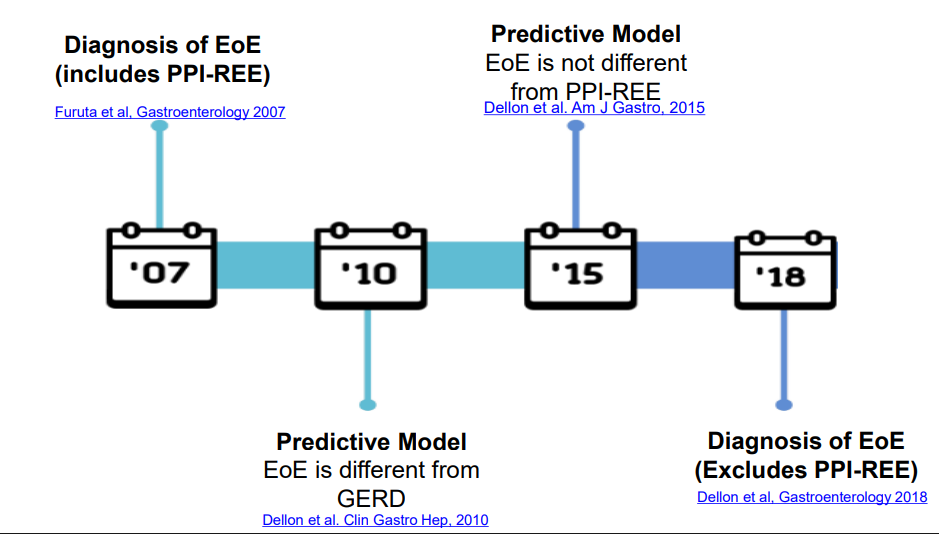
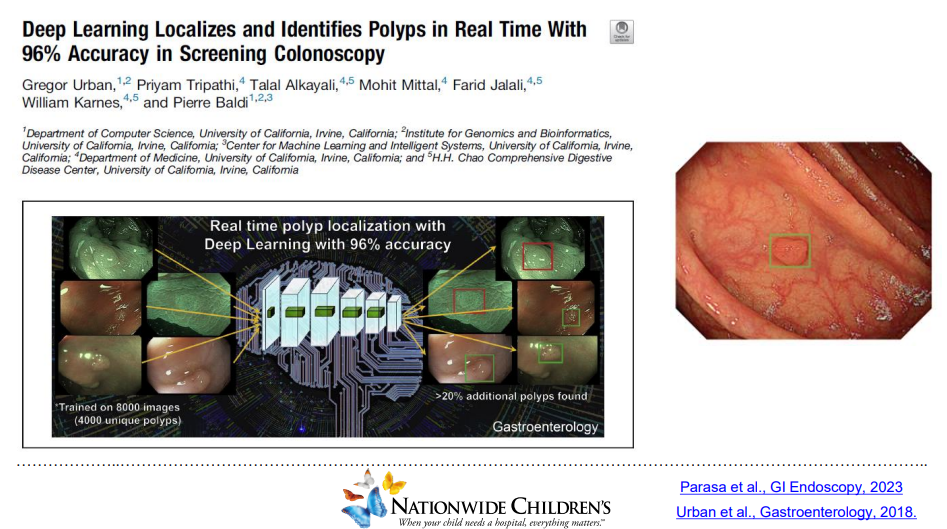
AI is teaching computers to think and predict problems. This can include analyzing radiology images, endoscopic findings (eg. polyps), interpreting EKGs, help with voice recognition, and scribe office visits (still in early stages)
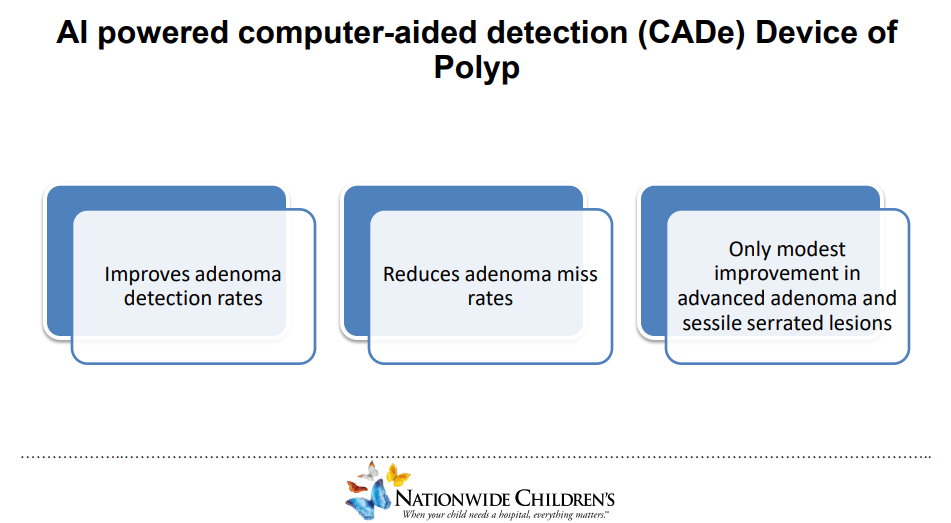
For colonoscopy, AI may aid polyp detection but whether this is clinically meaningful is unclear
With more complex analysis, AI is less transparent
AI algorithms can increase bias
Reliance on AI could lead to skill deterioration. MIT did a study showing less brain activity when using ChatGPT
Generative AI can create a summary of a patient chart. EHRs are partnering with AI
Agentic AI is when AI is set up to act autonomously like reminding patients to get vaccines, reminding to make appointments, or helping schedule appointments
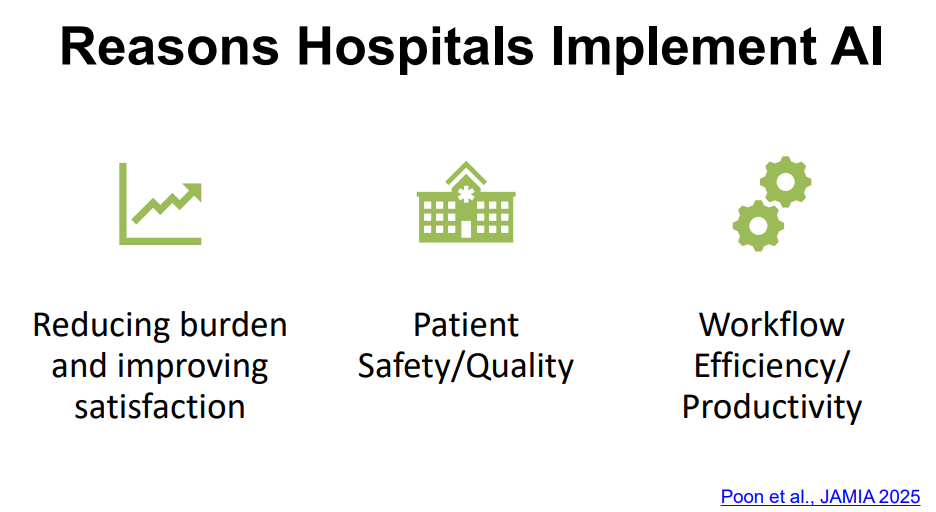
AI in the clinic and hospital may help reduce documentation burden, improve satisfaction and improve safety for patients
AI does have a problem of hallucination (‘making stuff up’) (my comment: so can people). Case report of man admitted to the hospital after following ChatGPT advice in substituting sodium bromide to reduce salt intake (Eichenberger et al. Annal Internal Medicine, 2025. A Case of Bromism Influenced by Use of Artificial Intelligence)
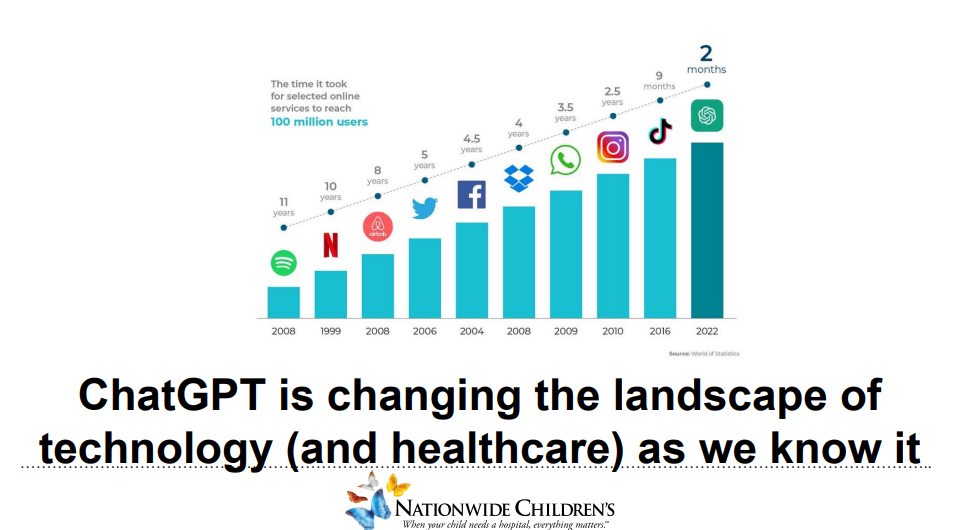
AI tools are still in early stages; however, ChatGPT uptake has been much quicker than previous internet tools
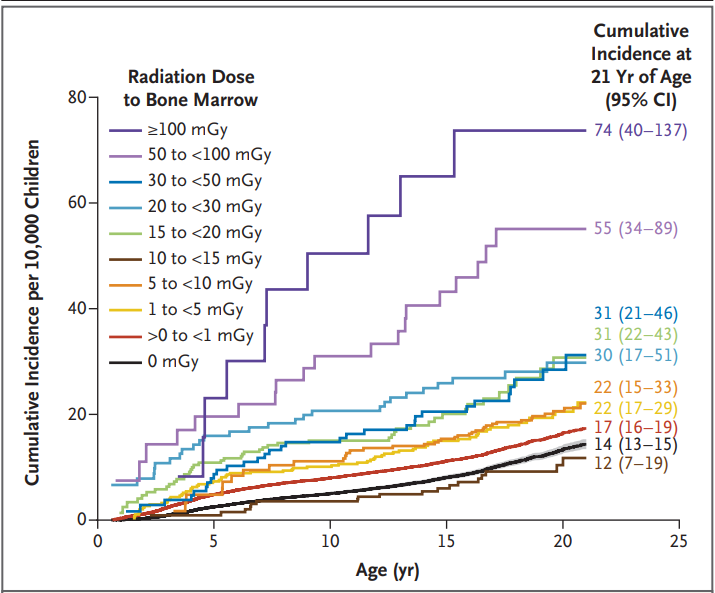
R Smith-Bindman et al. NEJM 2025; 393: 1269-1278. Medical Imaging and Pediatric and Adolescent Hematologic Cancer Risk
Methods: This was a retrospective cohort of 3,724,623 children born between 1996 and 2016 in six U.S. health care systems and Ontario, Canada, until the earliest of cancer or benign-tumor diagnosis, death, end of health care coverage, an age of 21 years, or December 31, 2017.
Key findings:
During 35,715,325 person-years of follow-up (mean, 10.1 years per person), 2961 hematologic cancers were diagnosed, primarily lymphoid cancers (2349 [79.3%]), myeloid cancers or acute leukemia (460 [15.5%]), and histiocytic- or dendritic-cell cancers (129 [4.4%]).
The excess cumulative incidence of hematologic cancers by 21 years of age among children exposed to at least 30 mGy (mean, 57 mGy) was 25.6 per 10,000
The authors estimated that 10.1% of hematologic cancers may have been attributable to radiation exposure from medical imaging, with higher risks from the higher-dose medical-imaging tests such as CT
Cumulative Incidence of Hematologic Cancer According to Attained Age and Radiation Dose to Bone Marrow among Children without Down’s Syndrome
Discussion Points:
“A 15-to-30-mGy exposure equivalent to one to two CT scans of the head was associated with an increased risk by a factor of 1.8”
“Although CT and other radiation-based imaging techniques may be lifesaving, our findings underscore the importance of carefully considering and minimizing radiation exposure during pediatric imaging to protect children’s long-term health”
“Research on Japanese atomic-bombing survivors showed that leukemia rates peaked 6 to 8 years after exposure, with excess risk lasting for more than five decades, particularly for acute myeloid leukemia”
This study tried to avoid concerns about reverse causation — in which imaging is performed because of existing cancer symptoms –by lagged exposures by 6 and 24 months
“The increasing use of low-value imaging in children and excessive radiation doses in CT are well documented…In many cases, reducing the imaging dose or substituting magnetic resonance imaging or ultrasonography may be more feasible than avoiding imaging altogether”
While the risks in aggregate appear quite substantial, the editorial (L Morton. NEJM 2025; 393; 1337-1339.Studying Cancer Risks Associated with Diagnostic Procedures –Interpret Wisely) makes the point that the risks for the individual are very small. “Fewer than 1% of youths in this study accumulated doses of 30 mGy or more from medical imaging and even at this exposure level, the excess cumulative incidence of hematologic cancers was low (25.6 per 10,000)…we need to ensure that all involved in medical imaging…wisely interpret the results…to understand the balance of the very small risks and the notable benefits of necessary imaging examinations to provide optimal patient care.”
My take: This study is a reminder to carefully evaluate the benefits, risks and alternatives when using ionizing radiation studies.
10/20/25 NY Times: Peanut Allergies Have Plummeted in Children, Study Shows “The new study, published Monday in the journal Pediatrics, found that food allergy rates in children under 3 fell after those guidelines were put into place — dropping to 0.93 percent between 2017 and 2020, from 1.46 percent between 2012 and 2015. That’s a 36 percent reduction in all food allergies, driven largely by a 43 percent drop in peanut allergies.”
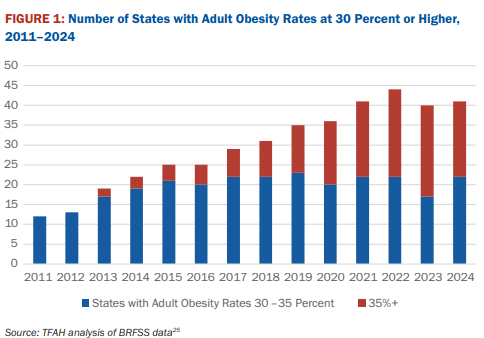
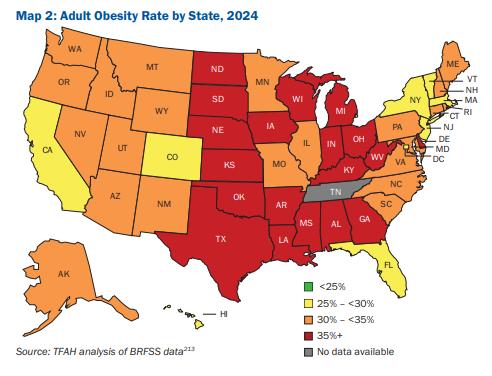
10/16/25 ABC News: Obesity remains high in the US., but more states showing progress, a new report finds “For the first time in more than a decade, the number of states with rates of obesity of 35% or more dropped, an encouraging sign that America’s epidemic of excess weight might be improving. But cuts to federal staff and programs that address chronic disease could endanger that progress, according to a new report released Thursday. Nineteen states had obesity rates of 35% or higher in 2024, down from 23 states the year before, according to an analysis of the latest data collected by the U.S. Centers for Disease Control and Prevention”
I was unaware previously of the Mitchell B Cohen award. This early to mid-career leadership award was established in 2023. It is terrific that this award is available and named after Dr. Cohen (my mentor) who has done so much for our field.
Congratulations to Dr. Feldman and Dr. Di Lorenzo -this year’s AAP award winners.
Reporting from Uganda, Mr. Kristof reports on the devastating and worsening impact related to the cuts of foreign aid –without apparent cost savings. He details three particular avoidable deaths and outlines the larger problem. Here’s an excerpt:
The Trump administration has claimed that no one has died because of its cuts to humanitarian aid…Yet what I find here in desperate villages in southwestern Uganda is that not only are aid cuts killing children every day, but that the death toll is accelerating.
Stockpiles of food and medicine are running out here. Village health workers who used to provide inexpensive preventive care have been laid off. Public health initiatives like deworming and vitamin A distribution have collapsed. Immunizations are being missed. Contraception is harder to get. Ordinary people are growing weaker, hungrier and more fragile. So as months pass, the crisis is not easing but growing increasingly lethal — and because children are particularly vulnerable, they are often the first to starve and the first to die… credibleestimates by experts suggest that the child death toll may be in the hundreds of thousands this year alone — and likely an even higher number next year.
A June 3 State Department memo, headed “sensitive but unclassified,” saying that the shutdown of the U.S. Agency for International Development will cost taxpayers $6.4 billion over two years… the money is necessary to manage “litigation, claims, residual payments and closeout activities.”..
A recent study published in The Lancet estimated that the cuts will cost the lives of about 690,000 children under the age of 5 in 2025, and 829,000 next year. The study estimated that some 3.1 million children under age 5 would die during Trump’s second term because of his cuts in humanitarian assistance...
PEPFAR, founded by President George W. Bush with the strong backing of America’s evangelical Christians. It turned the tide of AIDS and has saved 26 million lives — but the Trump administration has withheld some of its funding…About 65 percent of PEPFAR awards have been canceled…
Yet it’s also true that there are hints that the Trump administration is beginning to find some footing on aid. It has begun to place new orders for R.U.T.F. and has plans to move these stockpiles. It is preparing to hand over its food aid stockpiles to U.N. agencies to distribute to those in need. And it announced this month that PEPFAR will distribute lenacapavir, an important new drug that prevents AIDS transmission, in at least eight countries next year. These are real and positive steps; they just don’t make up for the larger pattern of chaos and cutbacks…