In the article, they note “the exception is for any live-attenuated virus vaccines or replication-competent viral vector vaccines that come to market.” Currently, all of the vaccines are inactivated (not live-attenuated).
These recommendations apply to approved populations which currently do not include pediatric patients or patients who are pregnant.
A recent commentary (JM Perrin et al. NEJM 2020; 383: 2595-2598. Medicaid and Child Health Equity) describes what is happening with Medicaid and the Children’s Health Insurance Program (CHIP).
Key points:
Over the past 20 years, the proportion of pediatric health care coverage provided by Medicaid and CHIP has been increasing. In 1997, these programs represented about 15% of health care coverage compared to ~35% in 2018. This corresponds to reductions in employer-provided coverage
Unlike private insurance, Medicaid is always available as it doesn’t have fixed enrollment periods
State funding of Medicaid creates challenges. “States have routinely used strategies for limiting enrollment”
“Medicaid’s low physician payment rates, which average about two-thirds of rates paid by Medicare for the same services, depress physician participation…Lack of access to specialists poses additional problems in many communities”
The authors recommend the following:
Medicaid should be expanded to cover all children from birth through 21 years of age
The federal government should assume full financial responsibility
Medicaid payments should parallel national Medicare standards
Key point: At 6 months after acute infection, COVID-19 survivors (n=1733 enrolled in study) were mainly troubled with fatigue or muscle weakness, sleep difficulties, and anxiety or depression. Patients who were more severely ill during their hospital stay had more severe impaired pulmonary diffusion capacities and abnormal chest imaging manifestations
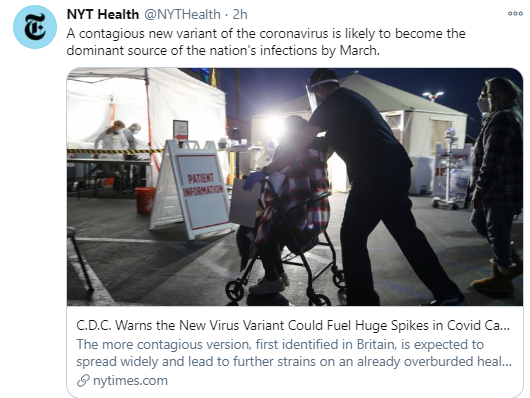
NY Times (1/15/21): C.D.C. Warns the New Virus Variant Could Fuel Huge Spikes in Covid Cases “The new variant, called B.1.1.7, was first identified in Britain, where it rapidly became the primary source of infections, accounting for more than 80 percent of new cases diagnosed in London and at least a quarter of cases elsewhere in the country.”
“A doctor researched the safety of the COVID-19 vaccinations not only to counsel his patients and staff but also to make his own decision about whether to get the vaccine.
Carey Goldberg of WBUR has the story about how most of the staff at the Cambridge Health Alliance COVID-19 clinic in Somerville, Massachusetts, “got to yes.”
22 minute presentation: COVID Vaccine Primer available at NPR website is a really good presentation (for more widespread adoption)
Methods: Data were obtained from the second National Firearms Survey, conducted online 30 July 2019 to 11 August 2019. Respondents (n=4030) were asked, “Has a physician or other health care practitioner ever spoken to you about firearm safety?”
Key finding:
Of all respondents, 7.5% (95% CI, 6.6% to 8.6%) had ever discussed firearm safety with a provider (12.0% [CI, 9.9% to 14.6%] of those living with children vs. 5.3% [CI, 4.4% to 6.3%] in homes without children)
In the comments to this brief study, several useful points were made.
#1: Train physicians on this topic: “1. This is not taking a position regarding gun ownership; 2. Access to firearms is associated with suicide, accidents, and firearm-related violence; 3. State laws regarding safe firearm storage; 4. Principles of safe storage; 5. Principle of separate ammunition storage; 5. Concept of removing firearms to another location (e.g., a relative) when children are small.”
#2 We can do better. “It’s not that hard to ask the question or put into your intake questionnaire; Is there a gun in the house? and if yes is the answer, follow-up”
Related blog posts:
No Exaggeration: Too Many Children Are Dying in the U.S. “The sad fact is that a child or adolescent in the United States is 57% more likely to die by the age of 19 years than those in other wealthy nations.” This is due mainly to more deaths from MVAs and from gun violence.
Two recent commentaries help advance the understanding of sexuality and transgender people with regard to discrimination and potential implications for health care.
Stroumsa et al note that about 1.9 million adults in U.S. identify as transgender. Key points:
This summer’s Supreme Court ruling in the employment-discrimination case Bostock v. Clayton County is likely to influence future court rulings regarding discrimination in health care coverage. “In the majority opinion, Justice Neil Gorsuch wrote, ‘It is impossible to discriminate against a person for being homosexual or transgender without discriminating against that individual based on sex.'”
Despite this favorable ruling for transgender persons, the current administration has tried to perpetuate discrimination on the basis of religious freedom. “The Trump rules stripping transgender rights from ACA protection are most likely invalid under Bostock.”
“The medical profession has an ongoing obligation to act..[to create] health care environments that are as welcoming for transgender and nonbinary patients as they are for cisgender patients.”
Shteyler et al discuss how birth certificate gender assignments can be detrimental. They note that birth certificates have changed many times to collect useful public information. One prominent feature has been a ‘line of demarcation’ in which there is legally identifying fields above the line and deidentified fields (eg. race, marital status) below the line which are reported in aggregate. They argue that sex assignment should be deidentified. Key points:
“Designating sex as male or female on birth certificates suggests that sex is simple and binary when, biologically, it is not.”
~1 in 5000 people have intersex variations
~1 in 100 exhibit chimerism, mosaicism, or micromosaicism, “conditions in which a person’s cells may contain varying sex chromosomes”
~6 in 1000 people identify as transgender. “Others are binary, meaning they don’t exclusively identify as a man or a woman, or gender nonconforming, meaning their behavior or appearance doesn’t align with social expectations for their assigned sex.”
“Only 9% of transgender people who want to update their gender on the documents succeed in doing so.”
“Leaving any sex designation visible on birth certificates sacrifices privacy and exposes people to discrimination.”
Medical providers have a duty to help policymakers understand the science and to make sure that “medical evaluations aren’t being misused in legal contexts.”
My take: When I was a child/adolescent, I barely had any concept regarding the spectrum of sexuality. Though, it was easy to see many individuals who were ostracized due to their differences. As a medical provider, I see children/teens whose sexual identity is homosexual, transgender, or nonbinary. I think it is a sign of progress that there is more acceptance to the variation in sexual identity but much more is needed.
On another hot button topic, David Brooks explains why programs aimed at reducing racial discrimination don’t work: 2020 Taught Us How To Fix This “The superficial way to change minds and behavior doesn’t seem to work, to bridge either racial, partisan or class lines. Real change seems to involve putting bodies from different groups in the same room, on the same team and in the same neighborhood.”
Full Text: All About COVID-19 Vaccines (Thanks to Seth Marcus for the reference). This article explains how the vaccines work, who essential workers are, and the effectiveness of the vaccines.
Rising case counts and rising test positivity rates mean there is more virus out there — and you need to double down on precautions, especially if you have a high-risk person in your orbit.
Whether your bubble is just your immediate household — or you’ve formed a bubble with others — take some time to check in with everyone and seal the leaks.
Mask up. You’re going to need it for a while.
Watch the clock, and take the fun outside… If you’re spending time indoors with people who don’t live with you, wear a mask and keep the visit as short as possible. (Better yet, don’t do it at all.)
The only way to drive down infection rates for now will be to avoid large indoor gatherings, wear masks, cancel travel and limit your holiday celebrations to just those who live in your home.
The vast majority of patients with Covid-19 will manage the illness at home. Check in with your doctor early in the course of your illness, and make a plan for monitoring your health and checking in again if you start to feel worse.
If you feel sick, you should be tested for Covid-19. A dry cough, fatigue, headache, fever or loss of sense of smell are some of the common symptoms of Covid-19. After you take your test, stay isolated from others and alert the people you’ve spent time with over the last few days, so they can take precautions while you’re waiting for your result.
While every patient is different, doctors say that days five through 10 of the illness are often the most worrisome time for respiratory complications of Covid-19.
The vaccines will be much less effective at preventing death and illness in 2021 if they are introduced into a population where the coronavirus is raging — as is now the case in the United States.
An analogy may be helpful here, says David Leonhardt, who writes The Morning newsletter for The Times. He explains that a vaccine that’s 95 percent effective, as Moderna’s and Pfizer’s versions appear to be, is a powerful fire hose. But the size of a fire is still a bigger determinant of how much destruction occurs.
The print version has some additional advice. From Dr. Fauci: “We have crushed similar outbreaks historically. We did it with smallpox. We did it with polio, We did it with measles. We can do it with coronavirus…The future doesn’t need to be bleak. It’s within our hands to really shape the future, both by public health measures and by taking up the vaccine.”
Between November 1, 2020, and December 13, 2020, the 7-day moving average for daily COVID-19 deaths tripled, from 826 to 2430 deaths per day
As occurred in the spring, COVID-19 has become the leading cause of death in the United States (daily mortality rates for heart disease and cancer, which for decades have been the 2 leading causes of death, are approximately 1700 and 1600 deaths per day, respectively)
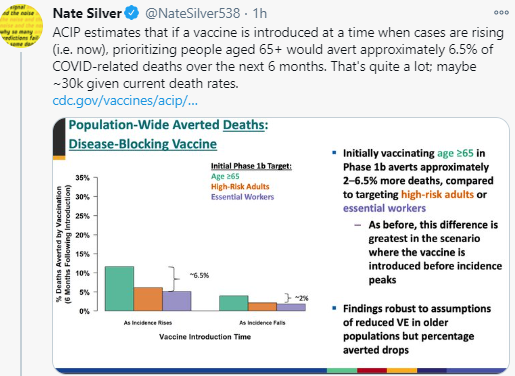
Vaccine Strategy: Nate Silver’s twitter feed suggests that after vaccination of medical personnel, focus of vaccine efforts should rely on age rather than at-risk conditions (which could affect 100 million in U.S). Using an age-based system would also be easier; it would minimize influence and wealth in the distribution of the vaccine.
“Excess mortality in younger adults: Among U.S. adults aged 25 to 44, there were 19% more deaths than expected — or 12,000 people — from March through July 2020. In JAMA, the researchers — including Dr. Rochelle Walensky, who has been nominated to lead the CDC — report that 38% of this excess mortality was directly from COVID-19, but that proportion varied by region. Deaths from COVID-19 were similar to or exceeded unintentional deaths from opioids in this age group in 2018 in several areas of the country. The authors write that this may be an underestimate of the COVID-19 mortality burden in younger adults, as they may have been undertested.”