Category Archives: General Health
Image Only: Eliminating Cervical Cancer with HPV Vaccine
Image

Mental Health of Medical Students
It is well-recognized that there is a high rate of burnout and even suicides among physicians. The concern regarding mental health extends to medical students. According to a recent commentary (JF Karp, AS Levine. NEJM 2018; 1196-8), “despite entering medical school with relatively good mental health, medical students become depressed, burned out, and suicidal at alarming rates.” This is thought to be due to “demanding schedules, cost, and stigma” to obtain mental health services.
The editorial advocates for medical students: “Working closely with the physician-services divisions of large hospital systems may help schools and hospitals leverage resources and provide shared opportunities to improve the care of students, trainees, and faculty and staff physicians.”
Related blog posts on burnout:
- Physician Burnout ‘Hidden Crisis’
- Physician Burnout Spreading (Part 1)
- Physician Burnout Spreading (Part 2)
- Addressing Physician Burnout
- Increasing Rates of Professional Burnout
- The burden of being a physician | gutsandgrowth
- MD Job Dissatisfaction –Million $ Mistake? | gutsandgrowth
- Off-Duty Doctors and Family Obligations | gutsandgrowth
- “It is never boring to be a physician” | gutsandgrowth
- Working While Sick: Red Badge of Courage or Scarlet Letter?

Frpm NEJM twitter feed
Images Only: In the news –Healing Property of Cow Dung Soap, Salmonella Outbreak, Better Evaluations for Doctors Who Frequently Prescribe Antibiotics


Expansive View of Endoscopy from Porto IBD Group
The pediatric IBD Porto Group of ESPGHAN has updated endoscopy guidelines: S Oliva et al. JPGN 2018; 67: 414-430. In total, the authors make 17 recommendations –here are a few of them:
A) In non-emergency situations, the diagnostic evaluation for suspected IBD in children should include a combination of EGD and colonoscopy. Multiple biopsies from each segment are recommended even in the absence of macroscopic disease.
B) Endoscopic evaluation is recommended for the following:
- before major treatment changes
- in symptomatic patients when it is not clear whether the symptoms are inflammation-related
- in Crohn’s disease(CD) to ensure mucosal healing during clinical remission
- in Ulcerative colitis (UC) to ensure mucosal healing during clinical remission only if fecal calprotectin is elevated
C) 6-12 months after bowel resection to identify postoperative recurrence
D) Endoscopic surveillance in pediatric UC after 10 years from the onset of disease (as early as 8 years in older children (>16 years) with risk factors like extensive disease and strong family history
E) In patients with concurrent primary sclerosing cholangitis (PSC), surveillance colonoscopy may be considered every 1-2 years, starting from time of PSC diagnosis. However, in children <12 years of age, surveillance could be postponed based on individual risk factors.
In addition to discussions of conventional endoscopy, the authors favor evaluation of small bowel inflammation: “the choice to perform CE [capsule endoscopy], MRE or both, depends on local availability and expertise.” The authors caution to consider strictures and the potential need for patency capsule prior to CE.
Conclusion of authors: “Endoscopy in pediatric IBD provides a more definitive diagnosis and disease extent evaluation, assesses therapeutic efficacy and leads to targeted therapy, which lessens complications and progression.”
My take: While I agree that endoscopy increases our understanding of disease extent and response to treatment, I do have some concerns about the recommendations (under section B above) regarding assessment of mucosal healing. Part of the concern is that there is not a single accepted definition of mucosal healing. Also, as a practical matter, there needs to be a discussion of the costs and more proof that frequent endoscopy will improve outcomes; it is possible that increased use of endoscopy will lead to some detrimental outcomes in some patients based on the interpretation of the results (eg. dropping a therapy that may be helping and replacing with a less effective treatment)..
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications/diets (along with potential adverse effects) should be confirmed by prescribing physician/nutritionist. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
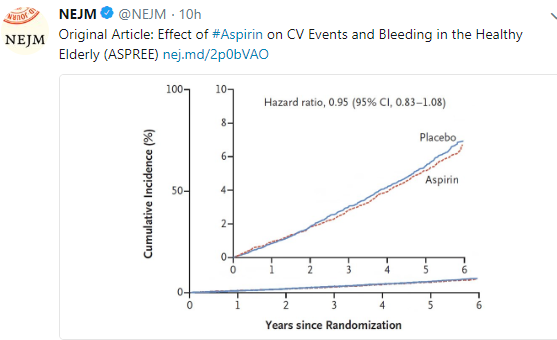
More on Aspirin
Over the last few years, I have posted a couple blogs on aspirin. While this topic is not a frequent concern in the pediatric population, it is often a concern for those caring for this population.



Images Only: EoE, Measles Outbreak, and Obesity Rate Disparities




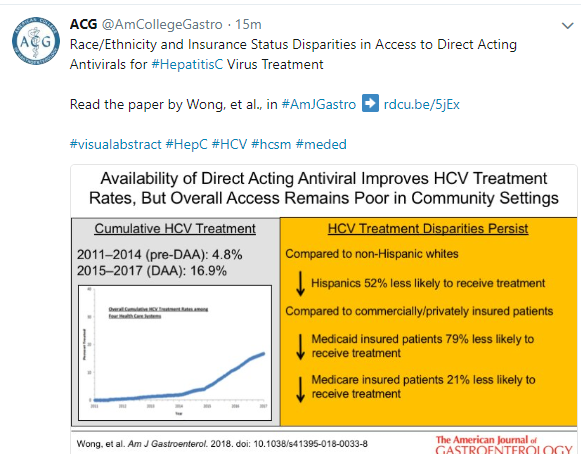
Images Only: Health Disparity for Maternal Deaths and HCV Treatment

This Makes Me Mad…Immigration Policy
When our government takes actions on behalf of our country, this reflects on all of our values. So, earlier this year I was disgusted and angry when I learned that as part of a ‘zero tolerance’ rule, young children were separated from their parents and placed in something akin to cages. For me, this is a stain on our country’s history that could be compared to other atrocities like the Tuskegee experiments and Japanese internment during WWII. While this policy was more short-lived, there are still children separated from their parents and for the children involved the consequences could be life-long. Sadly, our entire country is responsible because we elected this administration which adopted these policies.
Now, this administration which seems incapable of any shame, is planning more steps that should make decent persons upset. Additional threats to lawful immigrants are being devised (KM Perreira et al. NEJM 2018; 379: 901-3).
“Under current guidelines, persons labeled as potential public charges can be denied legal entry to the United States” and in some cases deported. Public-charge guidelines aim to keep immigrants from relying on public charges (eg. cash-assistance programs like welfare) for the first 5 years after admission to the U.S.
“The Trump administration is proposing sweeping changes to these [public-charge] guidelines.” One of these proposed expansions of public-charge determination is including enrollment for Obamacare, which is legally mandated and which can include subsidies. Another target is the Children’s Health Insurance Program. As a consequence of these guideline changes, instead of ~3% of lawful immigrants being considered as receiving a public charge, if adopted, this would increase to a range from 32% to 47%.
If these policies are adopted, this is likely to have a lot of adverse health consequences. Immigrants, including U.S.-born children, will be less likely to receive health care and more likely to be food insecure; 25% of U.S.-born children of immigrants currently receive SNAP (supplemental nutrition assistance program) benefits. Health consequences will affect millions and include an increase in low birth infants, increased infant mortality, and increased maternal morbidity.
For health care providers and institutions, implementation of these policies is likely to result in higher costs from uncompensated care.
In related commentaries (BL Grace et al. NEJM 2018; 379: 904-5, M Martin. NEJM 2018; 379: 906-7), the authors note the following points:
- “Current immigration policies are undermining trust in U.S institutions…and changing the way immigrants and refugees seek health care.” Many are worried that seeking health care could lead directly or indirectly (after providing information) to deportation
- “Even naturalized citizens fear that their status is no longer secure.”
- “I feel sad that my colleague’s 6-year-old patient has nightmares and urinary incontinence because she is terrified her parents will be deported. Sad that my patients fear coming to the hospital despite grave illness out of panic that someone will ask about their immigration status.”
My take: We are all accomplices (many unwitting) in the roll out of these detrimental policies that are now affecting lawful immigrants..
Related blog posts:
- America Needs Immigrants (Doctors)
- Rural Health: “And How Long Will You Be Staying?”
- Immigrant Doctors Blocked by New Rules Too

Life & Death before Roe v Wade
A recent commentary describes the tragic outcome of one young nurse in 1968: A Remembrance of Life before Roe v. Wade
An excerpt: Why am I telling Jane’s story now? The lack of legal and safe abortion before the Roe v. Wade decision of 1973 killed and maimed thousands of young women.