Methods: Here we characterize the trajectory by which the gut microbiome recovers its taxonomic and functional profile after antibiotic treatment in mice on regular chow (RC) or Western Diet (WD).
Key findings: “Only mice on RC undergo a rapid successional process of recovery. Metabolic modelling indicates that a RC diet promotes the development of syntrophic cross-feeding interactions, whereas in mice on WD, a dominant taxon monopolizes readily available resources without releasing syntrophic byproducts. Intervention experiments reveal that an appropriate dietary resource environment is both necessary and sufficient for rapid and robust microbiome recovery, whereas microbial transplant is neither.”
Conclusion (from authors): “Our data challenge widespread enthusiasm for faecal microbiota transplant (FMT) as a strategy to address dysbiosis, and demonstrate that specific dietary interventions are, at a minimum, an essential prerequisite for effective FMT, and may afford a safer, more natural and less invasive alternative.”
My take: This study suggests that the best way to get a “healthy” microbiome is to eat a healthy diet rather than to try to alter with FMT. This finding likely would be the same for probiotics as well.
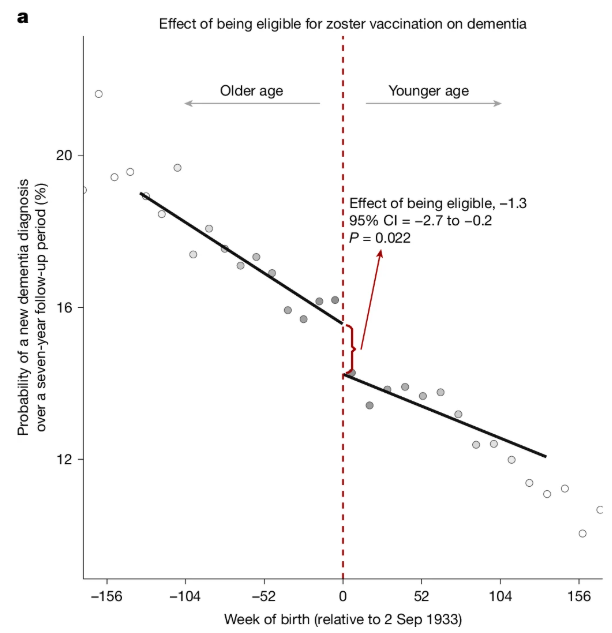
It’s been shown that reactivation of the chickenpox virus can lead to the accumulation of aberrant proteins associated with Alzheimer’s…
The new research, published Wednesday in Nature, analyzed data from more than 280,000 older adults in Wales and found that people who received the original shingles live virus vaccine were 20% less likely to develop dementia of any type than those who were not vaccinated...
The new study was possible because of an unusual public health policy in Wales that provided a “natural experiment” to explore the potential impact of the vaccine on dementia risk. With the rollout of the vaccine on Sept. 1, 2013, in Wales, shots were offered to people who were 79 on that date but not given to people who had turned 80.That allowed the German and Stanford University researchers to compare two groups of people with similar health characteristics who differed only by one week in age...
Bolstering the case for the shingles vaccine protecting against dementia were the findings from a study published in Nature Medicine in 2024 that analyzed medical records from more than 100,000 patients. That analysis suggested the newer shingles vaccine was associated with even better protection against dementia.
Two recent commentaries discuss some of the problems for aspiring physicians:
RP Walensky, LD Walensky. NEJM 2025; 392: 1251-1254. Application Overload — A Call to Reduce the Burden of Applying to Medical School
DB Holt, EA Elster. NEJM 2025; 392: 1249-1251. Rethinking Shadowing for Aspiring Physicians
In the first article, the authors detail the burden associated with the common-place high-volume applications to medical schools.
“The cost is approximately $150 per school for application fees, plus $345 for taking the MCAT and having the score distributed through AMCAS. These fees are waived for qualifying low-income applicants (as primarily defined by household income below 400% of the national poverty level) who apply to the AAMC Fee Assistance Program and provide the required financial documentation.2 After submitting the primary application, applicants face a flood of secondary applications, some requiring up to eight additional essays. Even when the essay prompts are similar to those from other schools, the instructions often specify different lengths. One premedical student posted on social media the findings of his review of 54 medical schools’ secondary applications: he identified 222 different prompts, which he provided to help applicants get a jumpstart on their frenzied essay writing.3..
Between 2013 and 2023, … the total number of applications and the average number of applications per student increased dramatically — by 40% (from 690,281 to 966,947) and 28% (from 14.4 to 18.4), respectively. Despite the disproportionate escalation in applications submitted, the success rate (matriculants divided by applicants) remained flat (range, 36 to 44%).”
The authors recommend limiting applications to 10 to 12 medical school applications per applicant. This would benefit students as well as faculty burdens.
“The secondary-application process also needs to be reined in. Medical schools could adopt standardized secondary essays… Under this model, a student applying to 10 schools would complete a maximum of 13 secondary essays — 3 standardized and 1 customized essay per school — rather than the current norm of 60 to 80 essays (e.g., 20 secondary applications with 3 to 4 distinct essays each).”
My take: In Charlie and the Chocolate Factory, there are only five golden tickets. If everyone buys twice as many Wonka bars, it is a lot more expensive and perhaps more time-consuming. For medical school applicants, applying to 20 or more programs does not help if almost everyone is doing this. It does disadvantage the minority who do not have the financial means or available time to complete this arduous task.
In the second commentary, the article details the problems with shadowing experiences.
“Medical school admission in the United States remains intensely competitive. In 2024, according to the Association of American Medical Colleges (AAMC), prospective students submitted an average of 18 applications apiece…Many medical school admissions committees consider shadowing a physician to be an essential clinical experience for professional identity formation, so nearly all applicants now do some shadowing: 95% of respondents to the 2024 AAMC Matriculating Student Questionnaire (MSQ) said they’d spent time observing a physician at work.1…
Premedical students are spending more time shadowing — sometimes hundreds to thousands of hours, which often necessitate taking a “gap year” between college and medical school at a financial cost…Three quarters of medical school applicants report taking time off before medical school, 50% taking 1 to 2 years and 25% taking 3 or more years...
These additional years delay entry into the workforce and result in higher levels of debt than moving more quickly toward potential earnings as a physician; one lost year of a physician’s salary (an average of $265,000) would result in an estimated net loss of $2 million by retirement if the money were invested at a 7% return…
Although medical schools consider clinical experiences other than shadowing, a review of our own data suggests that applicants who have shadowed physicians for more than 50 hours are more likely than their peers to be admitted — and more likely to come from higher-income families.“
The authors point out that unstructured observation is of unclear benefit. A course from Stanford, that far fewer hours (11-20 hrs) was sufficient for more than 90% of students “to decide whether medicine was the right career for them….The current emphasis on shadowing not only contributes to a longer and more expensive medical education pathway but also discourages nontraditional applicants and pursuit of genuine interests in other areas that make for well-rounded physicians.”
My take: The pathway to medical school has become more time-consuming and expensive. At the same time, it is doubtful that lengthy shadowing experiences or extensive numbers of applications are benefiting aspiring students.
S Machado et al. NEJM 2025;392:1310-1319. Association between Wealth and Mortality in the United States and Europe
Methods: This was a longitudinal, retrospective cohort study with 73,838 adults (mean [±SD] age, 65±9.8 years), a total of 13,802 (18.7%) died during a median follow-up of 10 years.
Key findings:
The gap in survival between the top and bottom wealth quartiles was wider in the United States than in Europe
The poorest Americans appeared to have the lowest survival among all wealth groups in the study sample
Survival among the participants in the top wealth quartiles in northern and western Europe and southern Europe appeared to be higher than that among the wealthiest Americans
Survival in the wealthiest U.S. quartile appeared to be similar to that in the poorest quartile in northern and western Europe
The countries in the Survey of Health, Ageing, and Retirement in Europe (SHARE) were split into the following three groups: northern and western Europe (Austria, Belgium, Denmark, France, Germany, the Netherlands, Sweden, and Switzerland), southern Europe (Italy, Portugal, and Spain), and eastern Europe (Czech Republic, Estonia, Hungary, Poland, and Slovenia). The shaded area in Panel A indicates the difference between quartile 4 (the wealthiest) and quartile 1 (the poorest) in the Health and Retirement Study (HRS); the same shaded area was added in Panels B, C, and D for the purposes of comparison. The median duration of follow-up was 10 years in both surveys, and the mean (±SD) age at baseline was 65±9.8 years.
In their discussion, the authors note that health care access should not be a factor for wealthy Americans. However, “systematic factors may influence longevity across social strata, such as diet; environment; behavioral, cultural, and social attitudes; and opportunities for social mobility.2,28,32,33 The poorest are most vulnerable to these systemic factors, but these factors are broad and probably affect the entirety of society.”
My take: This study indicates that mortality in the United States is higher than in Europe, even at higher wealth levels.
“Fifty years ago, life expectancy in the U.S. and wealthy European countries was relatively similar. That began to change around 1980. As European life expectancy steadily increased, the U.S. struggled to keep pace — and its life expectancy even began declining in 2014…The wealthiest group in northern and western Europe had mortality rates about 35% lower than the wealthiest group in the U.S.”
These charts show measles data through April 7th. Some additional data through Apirl 11th is listed below.
For those interested in a deeper dive into the measles numbers, you can follow Caitlin Rivers substack. From her notes on April 11:
“Since my last update on Tuesday, Arkansas and Hawaii reported cases for the first time this year. At least five states have reported ten or more cases, which is very unusual. Texas continues to register the most cases, with 541 to date.”
“According to the CDC, 712 cases have been reported so far this year. 1 in 3 (32%) are under the age of 5, and 1 in 10 (11%) have been hospitalized.”
Congratulations to Dr. Benjamin Gold who is one of the honored heros at this year’s CCFA Take Steps. Also, congratulations to Clara Cann and Lauren Leonard who are being recognized as well.
A Canadian study, published Wednesday in the journal PLOS Mental Health, finds that young people who consume multiple muscle-building products are more likely to show symptoms of a condition called muscle dysphoria…
About 2,730 Canadian teens and adults ages 16–30, mostly white males and females, were recruited via Instagram and Snapchat advertisements…
26% of the boys and men scored above the level for muscle dysmorphia — that is, being extremely preoccupied with a perceived lack of muscle mass or tone. Use of the workout supplements and products was associated with more symptoms of muscle dysmorphia…
Experts said the findings spotlight how unrealistic body ideals — often fueled by fitness influencers who promote or sell workout supplements online — may be driving more children and young adults to overuse powders or pills.
My take: The patients in this study may not be representative of the entire population; thus, the percentages of those affected should be interpreted carefully. Nevertheless, it is likely that a very significant proportion of young men have “muscle dysphoria” (also termed “‘bigorexia”). Supplements are poorly regulated and can result in adverse effects at any dosage (see posts below).
There is very little that Americans can agree on these days…
But one thing nearly everyone agrees on? Vaccines are good.
This simple fact has been overshadowed by fears about what will happen to vaccine policy under Robert F. Kennedy Jr., the new secretary of health and human services. He has a long history of vaccine skepticism, and critics fear his leadership could lead to interference with vaccine programs or even withdrawal of vaccines from the market. Such moves are already roiling some state health programs. In Louisiana, the Health Department will “no longer promote mass vaccination,” instead leaving vaccine education to medical providers…
Recent reports in the news media and medical journals highlight a decline in the proportion of kindergartners who have received the measles, mumps and rubella shot. In the past five years, national coverage has fallen to 93 percent, from 95 percent, and in some states like Idaho, it is as low as 80 percent. But while these numbers fall short of the national goal of 95 percent required to maintain herd immunity for measles, they remain a resounding show of confidence…
Some 92 percent of American children received the polio vaccine by age 2, and more than 90 percent were vaccinated against hepatitis B. And it’s not just because of school requirements. Nearly nine in 10 Americans — including 86 percent of Republicans — say the benefits of childhood vaccines outweigh the risks...
Emphasizing the popularity of vaccines is not merely a matter of correcting the record. Studies have shown that presenting vaccines as a subject of debate or controversy can unintentionally reinforce vaccine hesitancy by making the issue appear less settled. For instance in one study, researchers found that college students who were asked to read a news report on vaccine safety that presented both sides in a falsely balanced fashion came away with the mistaken impression that the science on vaccine safety was in flux…
Routine vaccinations are just that: routine. Nearly all children receive them, and millions have benefited by being spared painful diseases and death. Leaders who undermine this basic tool may find themselves on the wrong side of both science and voters.
My take: Caitlin Rivers provides a lot of useful advice regarding infectious diseases. She has frequent (~weekly) substack articles with up-to-date information regarding infection prevalence (eg. Flu, COVID, norovirus, etc). Link to substack: Force of Infection
“The medical community largely anticipated that combining the abilities of doctors and A.I. would be the best of both worlds, leading to more accurate diagnoses and more efficient care…That assumption might prove to be incorrect. A growing body of research suggests that A.I. is outperforming doctors, even when they use it as a tool…
Simply giving physicians A.I. tools and expecting automatic improvements doesn’t work. Physicians aren’t completely comfortable with A.I. and still doubt its utility, even if it could demonstrably improve patient care…
Medical training will need to adapt to help doctors understand not just how to use A.I., but when to rely on it and when to trust their own judgment…But the promise for patients is obvious: fewer bottlenecks, shorter waits and potentially better outcomes. For doctors, there’s potential for A.I. to alleviate the routine burdens so that health care might become more accurate, efficient and — paradoxically — more human.”
In a related Substack article (open access: Opinion | When A.I. Alone Outperforms the Human-A.I. Partnership), Dr. Topol and Dr. Rajpurkar list several studies showing that AI alone may be better than physicians with AI under some circumstances:
My take (borrowed from the authors): “The future of medicine won’t be shaped by a simple choice between human or artificial intelligence, but by our ability to understand their respective strengths and limitations, and to orchestrate their collaboration in ways that truly benefit patient care.”