More information from this year’s annual NASPGHAN meeting.
This blog entry has abbreviated/summarized these presentations. Though not intentional, some important material is likely to have been omitted; in addition, transcription errors are possible as well.
IBD Treat to Target: Treat the Patient or Treat the Disease
Robert Baldassano Children’s Hospital of Philadelphia
I missed the first few minutes of this presentation, even though I had highlighted this as one of my top priorities. So, if anyone reading this post has some additional comments, they are certainly welcome.
Key points:
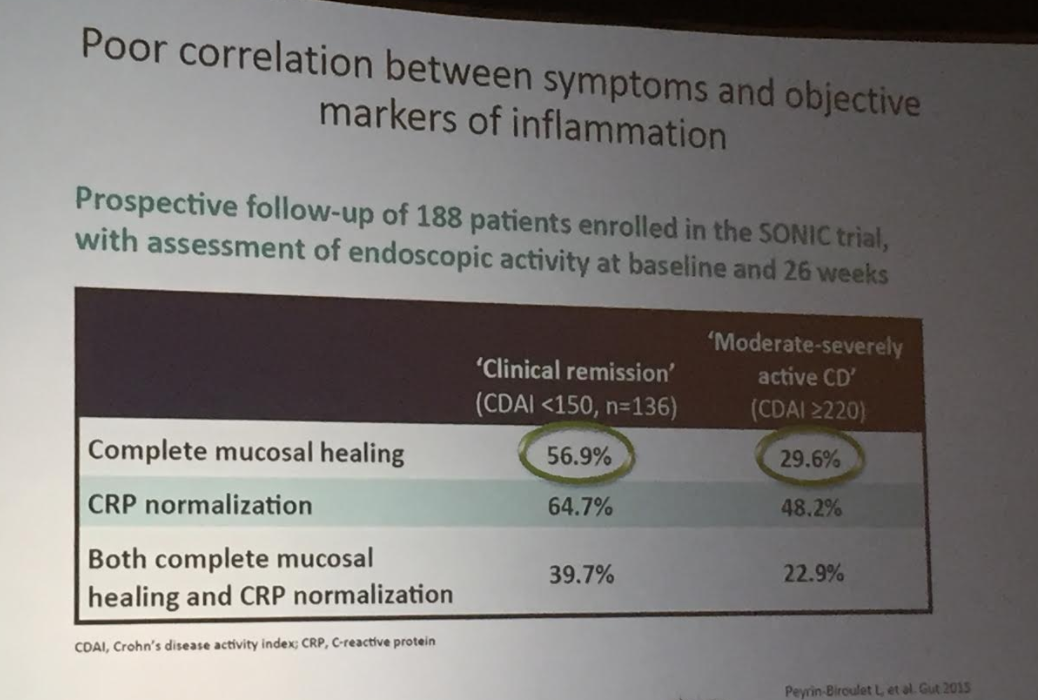
- Do not rely on symptoms alone to assess patient improvement.
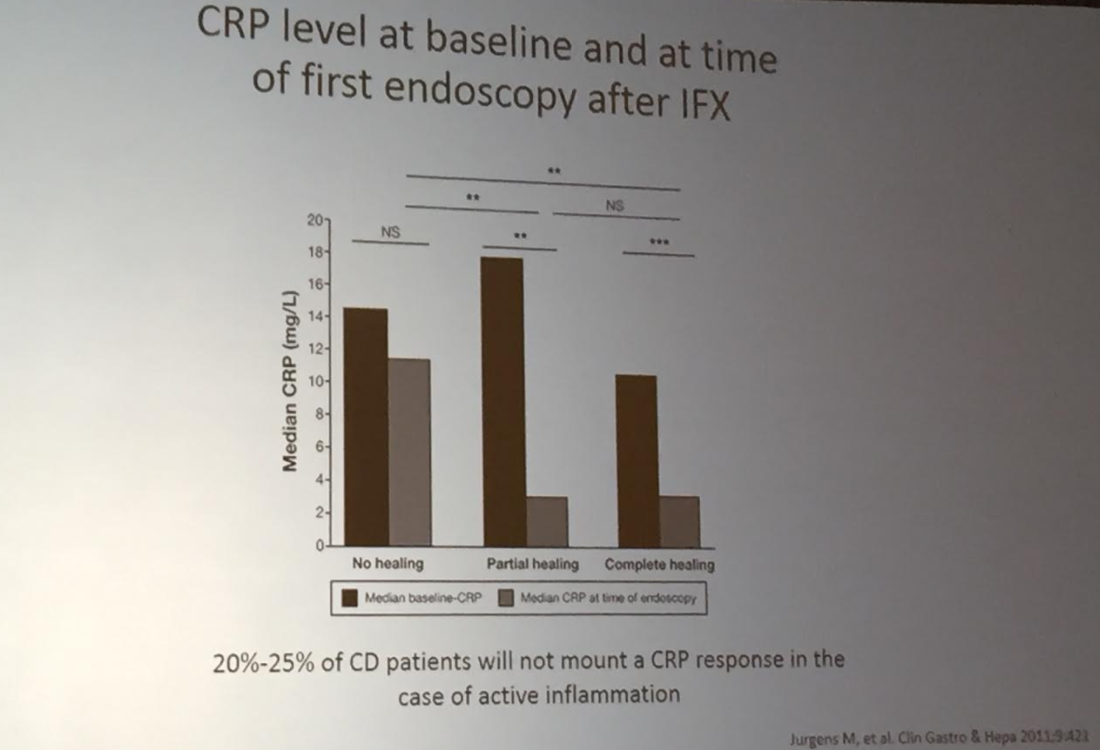
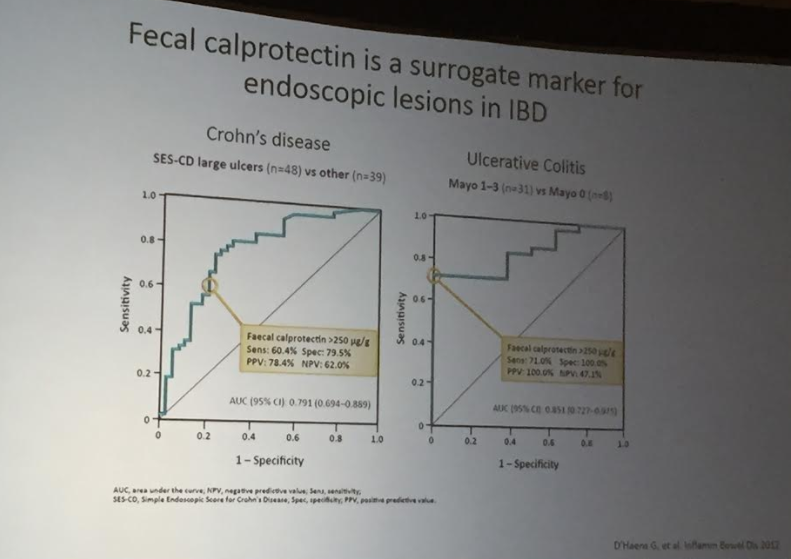
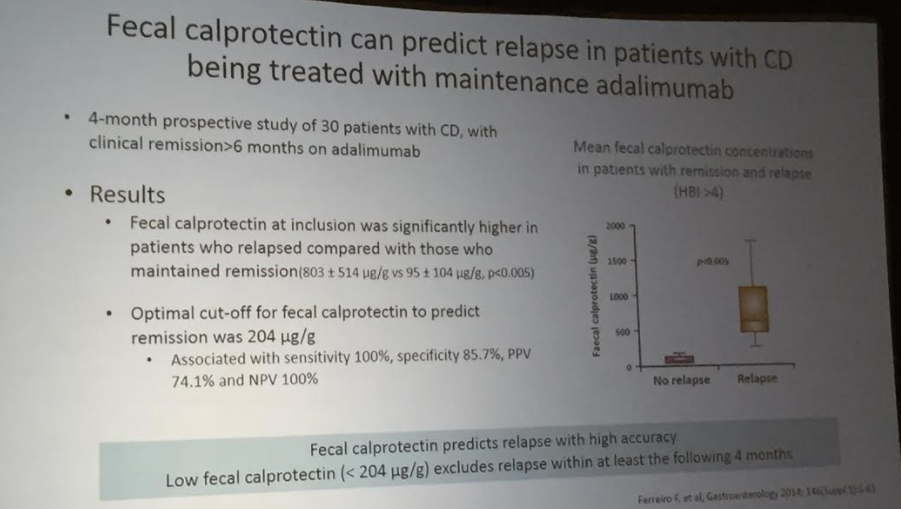
- Best surrogate marker: calprotectin. Frequent calprotectin levels can help determine objective improvement; it is much more helpful than CRP as ~25% of patients do not elevate their CRP levels
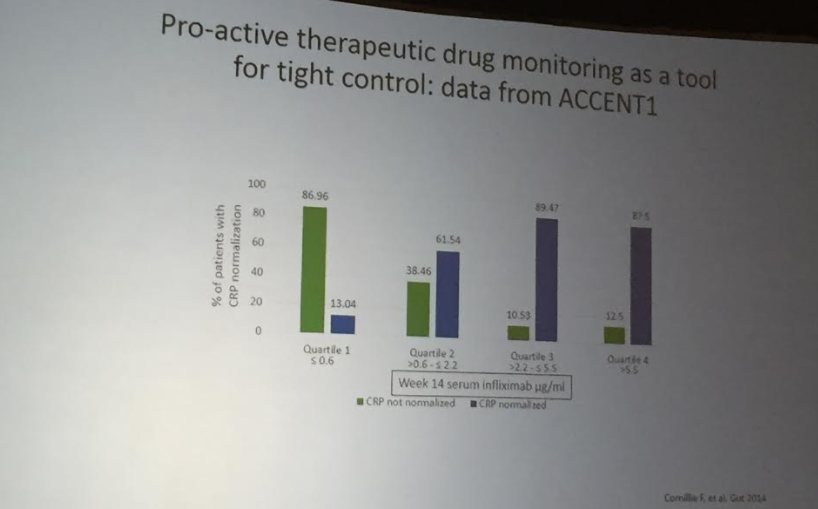
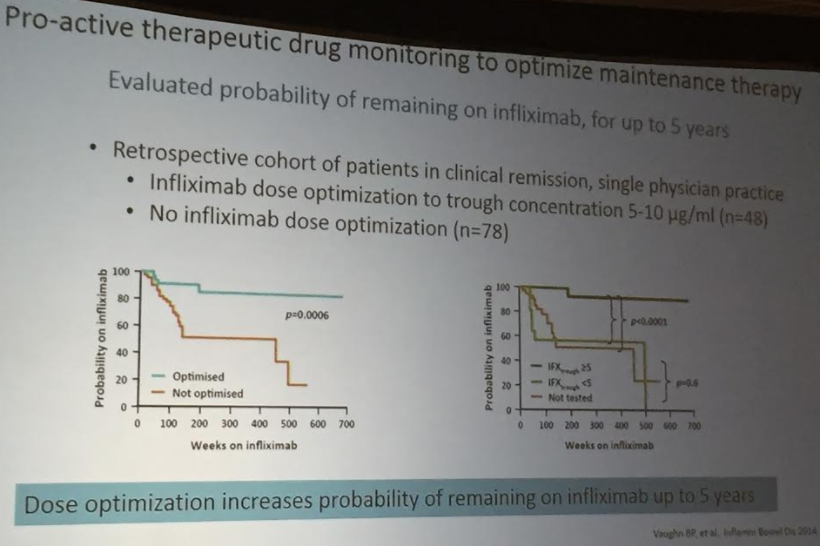
- Therapeutic drug monitoring is important in improving outcomes. Dose optimization improves response rate and durability of infliximab response.
- Evolving targets in ulcerative colitis. Even histologic activity, in the absence of endoscopic activity, is associated with relapsing disease
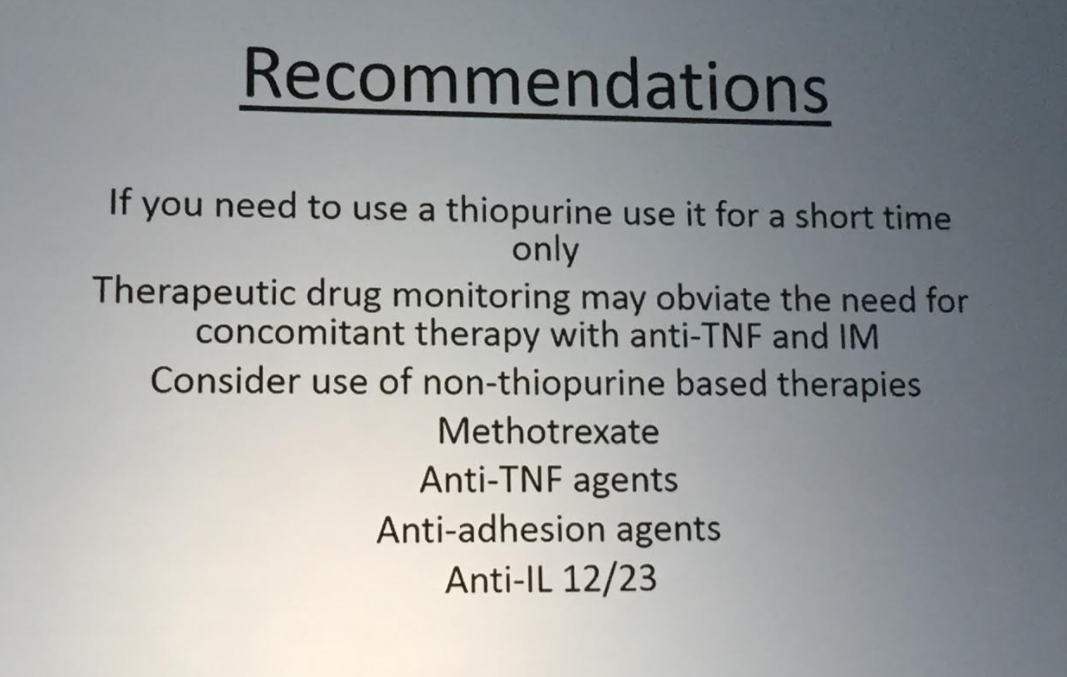
- Dr. Baldassano indicated that he no longer is starting patients on thiopurine therapy. There are “36 phase 3 trials underway.” Thus, many promising options for those who may burn through current treatments
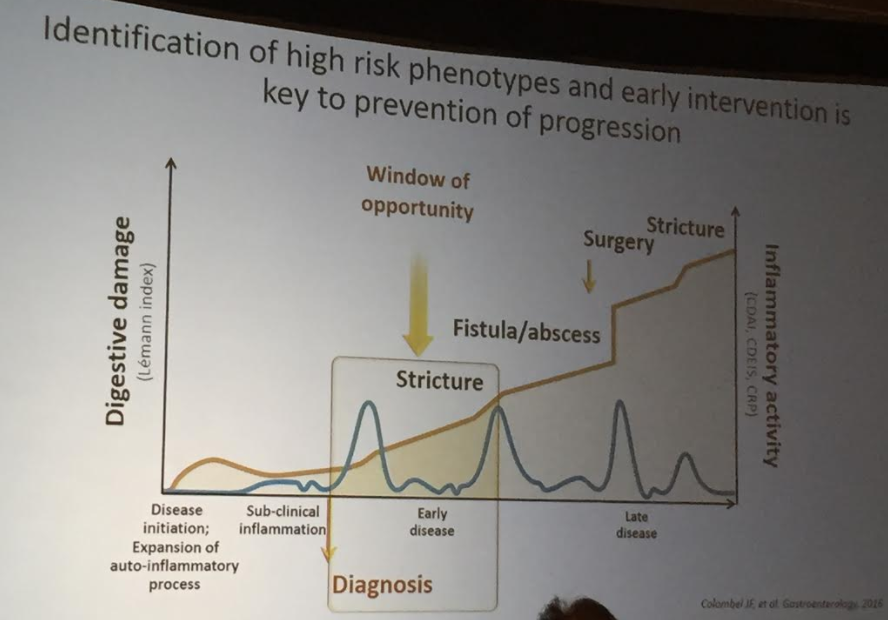
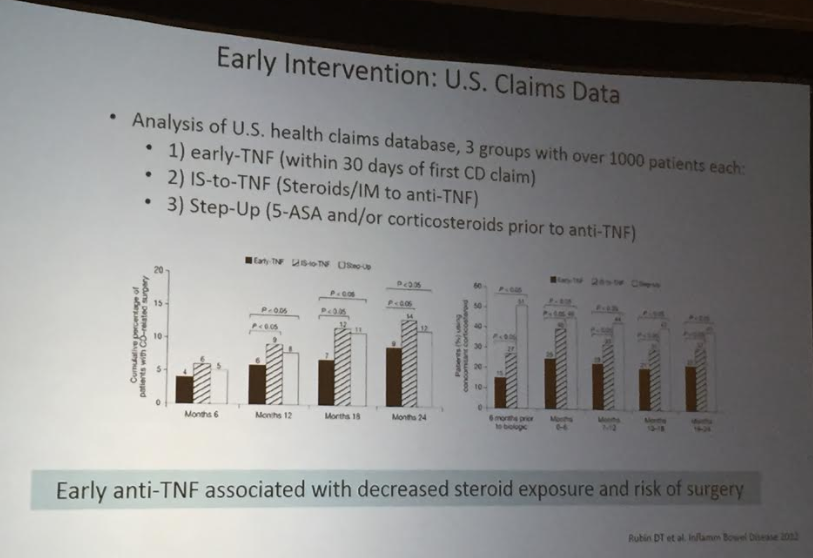
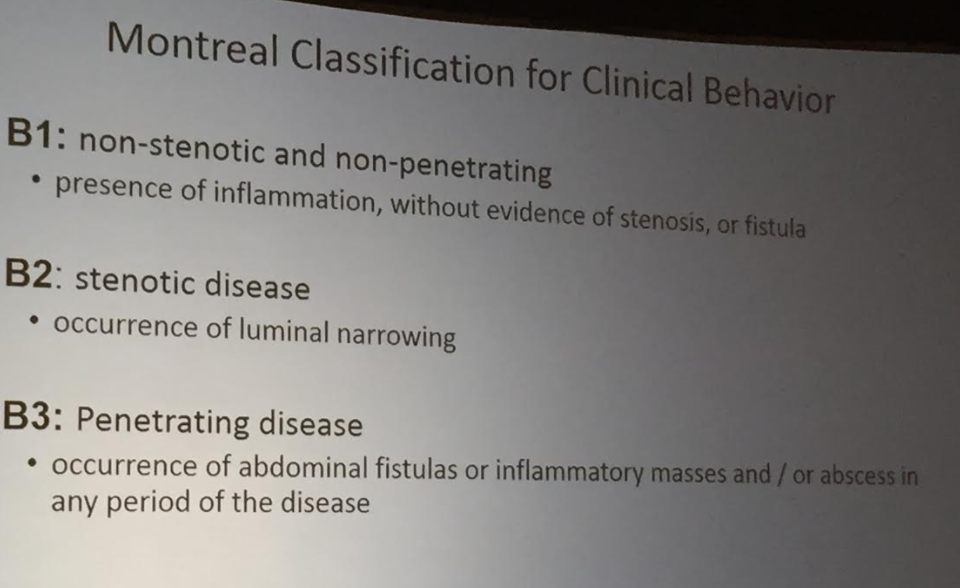
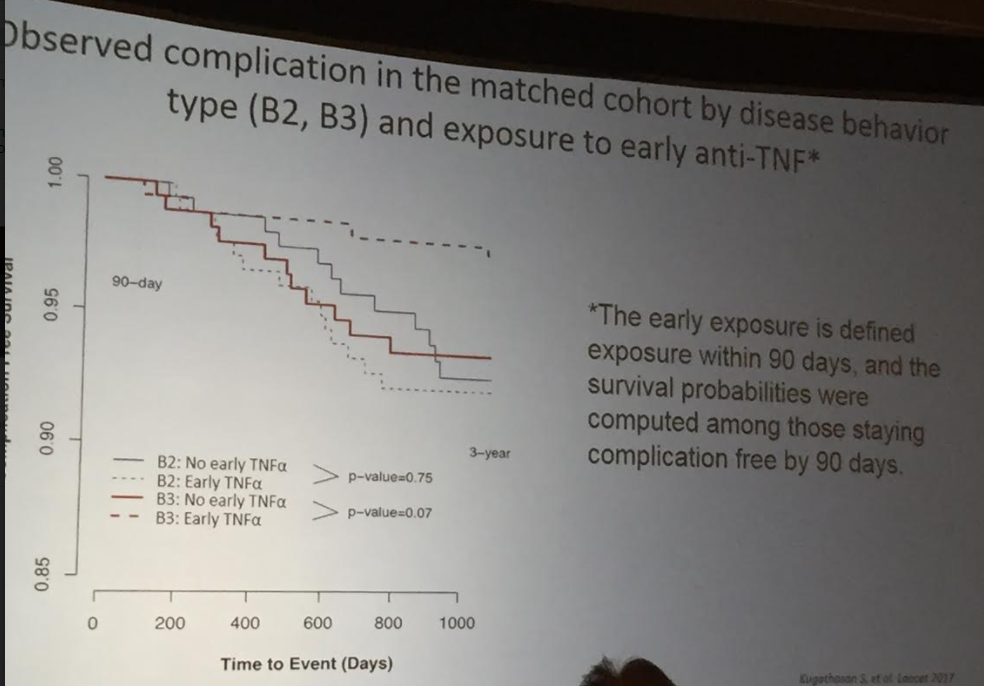
- This lecture reviewed data from the RISK study showing that early (1st 90 days w/in diagnosis) TNF therapy helps prevent penetrating disease (related post: CCFA Update 2017/RISK study)
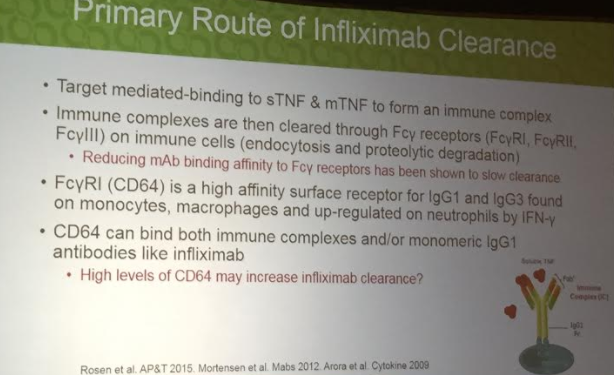
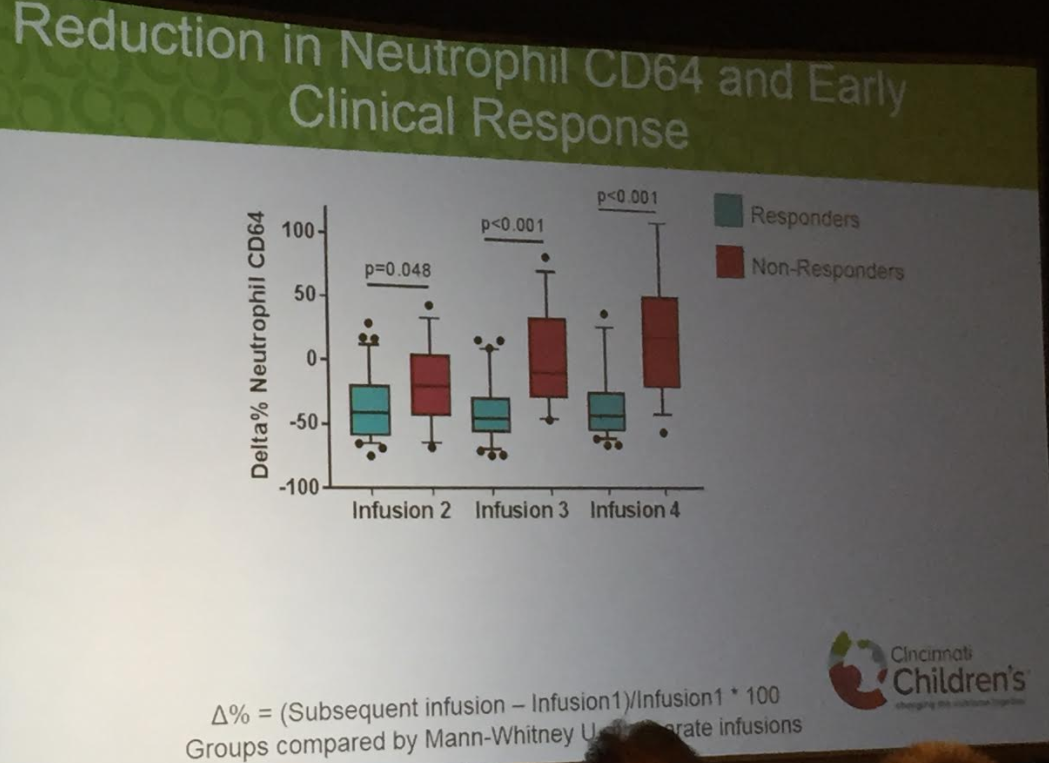
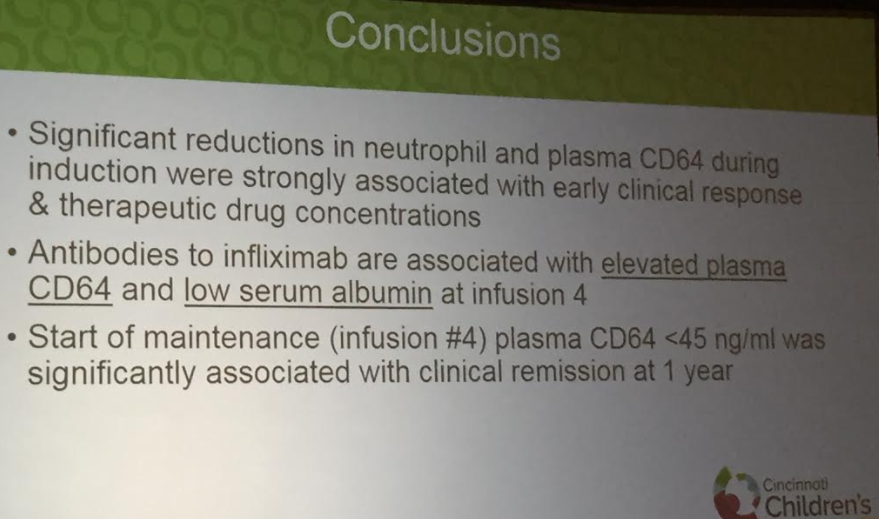
Another presentation by Philip Minar et al (Cincinnati Children’s Hospital Medical Center) shows that CD64 suppression is an early biomarker of response to infliximab therapy.