- Finding Value in Unexpected Places — Fixing the Medicare Physician Fee Schedule. RA Berenson, JD Goodson. NEJM 2016; 374: 1306-10.
- When Is It Ethical to Withhold Prevention? TA Farley. NEJM 2016; 374: 1303-5.
As noted in yesterday’s blog post, after reading these two commentaries I thought a little more about value in pediatric gastroenterology. These articles though focus on other aspects. In the first reference, the authors explain the flaws with moving from volume to value-based care. They note that the medicare physician fee schedule (MPFS) has a powerful influence on physician activities and “their tendency to perform unneeded tests and procedures.” In fact, the fee schedule heavily contributes to growing shortages of primary care physicians. Key points:
- “Two key flaws in the RBVS [resource-based relative value scale] are its substantial misevaluations of physician work and the failure of current service codes to capture the range and intensity of nonprocedural physician activities, known as evaluation and management (E/M) services.”
- “The MPFS still assumes that it takes nearly 30 minutes to interpret a magnetic resonance image of the brain…typically takes about 10.” Echocardiogram per MPFS assumes 31 minutes, but takes 5-10 minutes. For colonoscopy with polyp removal, MPFS assumes 78 minutes, but this is overestimated as well.
- Valuations depend on AMA-sponsored expert panels…not surprisingly, updates that reduce RVUs are rarely proposed.
- While the commentary implies that procedural codes are overvalued, it notes that due to complexity of chronic conditions that E/M codes are undervalued.
- Their conclusion: “implementing new incentives and quality measures in new payment models while maintaining a broken fee schedule is a prescription for failure.”
The second reference bemoans the fact that the medical system will spend enormous amounts of money to prolong the life of an individual with terminal cancer for a few weeks but will not see the imperative of providing adequate prevention measures. Key points:
- “Many people reject any attempt to put a dollar value on human life…but…limits of funding make it impossible to pay for every conceivable intervention.”
- Cost-effectiveness is not considered by Medicare in determining treatment. “For example, treatment of metastatic lung cancer may cost $800,000 per QALY [quality-adjusted life-year], but it is typically provided. In sharp contrast, primary preventative services are often withheld even if they are highly cost-effective.”
- Diabetes prevention program focused on exercise and nutrition has QALY costs of $14,000. Smoking cessation with nicotine-replacement therapy has QALY <$5000.
- Author’s conclusion: “because withholding primary prevention leads to unnecessary suffering and death, we should be just as creative in finding ways to pay for it” as we do with treatment of all illnesses.
My take: At an individual physician level, we need to keep working to utilize our resources more carefully. However, at a policy making level, efforts at improving incentives for primary prevention and primary care are needed.
Related blog posts (see yesterday’s post Why are so many Low Value Endoscopies Performed? for related links as well):

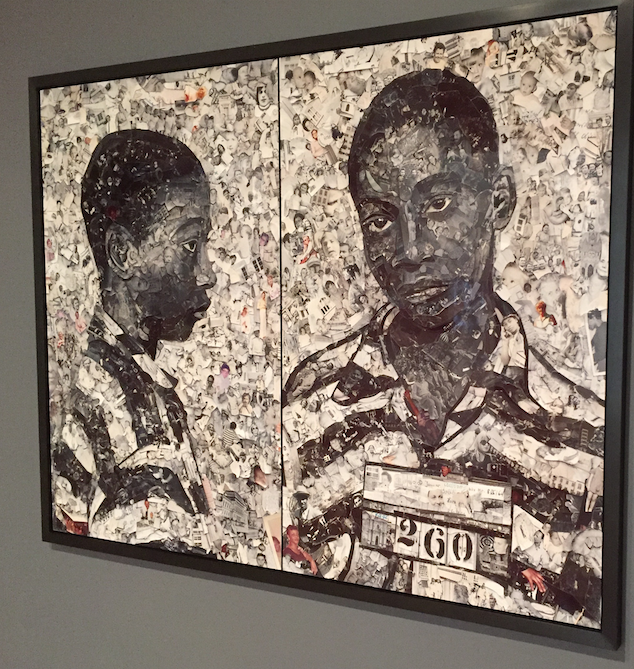
Poster on Front of High Museum is reproduction of Vik Muniz piece created from Jelly and Peanut Butter