This blog entry has abbreviated/summarized this terrific presentation; most of the material has been covered in this blog in prior entries but still this was a useful review. Though not intentional, some important material is likely to have been omitted; in addition, transcription errors are possible as well.
Optimizing Therapeutic Drug Monitoring –Dr. Hans Herfarth
- Trough levels have been recognized to correlate with remission rates. Good data from SONIC (2010) for infliximab. Ultra2 trial (2013) showed similar data for adalimumab.

- Low albumin predicts higher rates of failure, possibly due to loss of infliximab in stool.
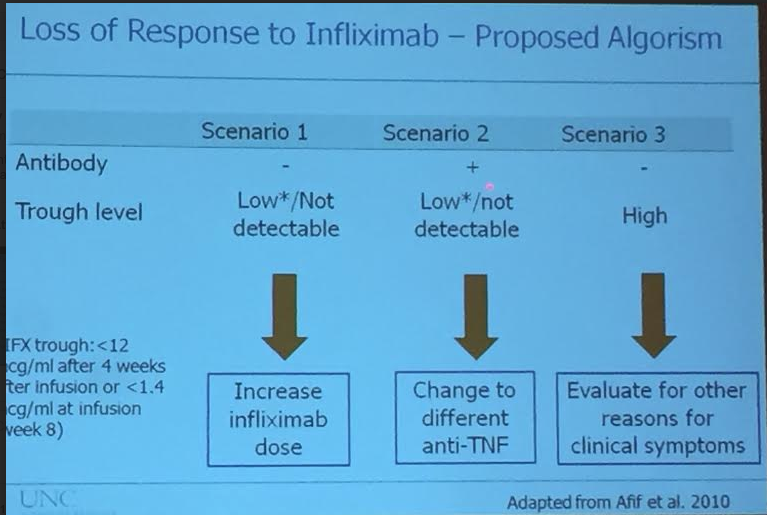
- Reviewed algorithm for loss of response to infliximab based on trough levels. If low infliximab and no antibodies, increase dosing of infliximab has high likelihood of clinical response.
- If high infliximab and not responding, evaluate for other reasons including irritable bowel, and strictures.
Scenarios that create confusion with therapeutic drug monitoring:
- If clinically-well patient has antibodies and adequate drug level, could observe or possibly add immunosuppressive agent. ~3% of patients have simultaneous ATI and IFX detection.
- If clinically-well with low infliximab level, could increase dose or observe.
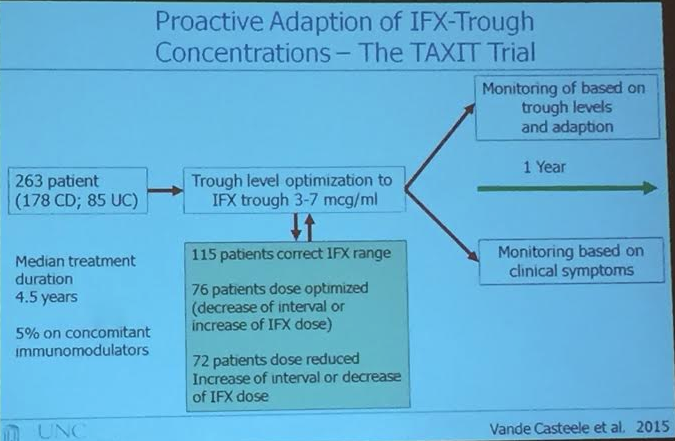

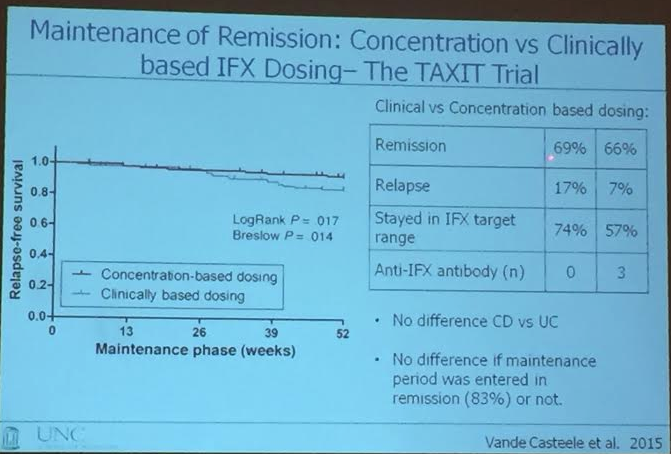
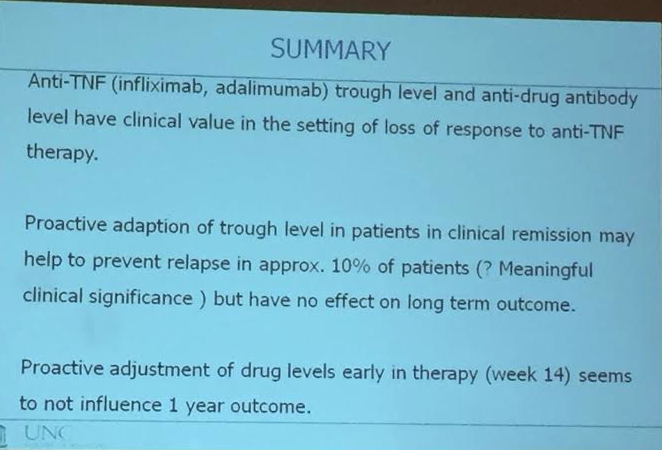
- In TAXIT study, however, lowering dose (panel B above) to get in target range was associated with a lower rate of response. No clear difference between clinically-based changes compared with proactive monitoring. Proactive adaption of trough levels may help prevent relapse in ~10% but not shown to alter long-term outcomes
- TAILORIX study looked at tailoring dose at week 14. ‘Week 14 adaption did not make a significant difference at 1 year.’ Limitation: 122 patients.
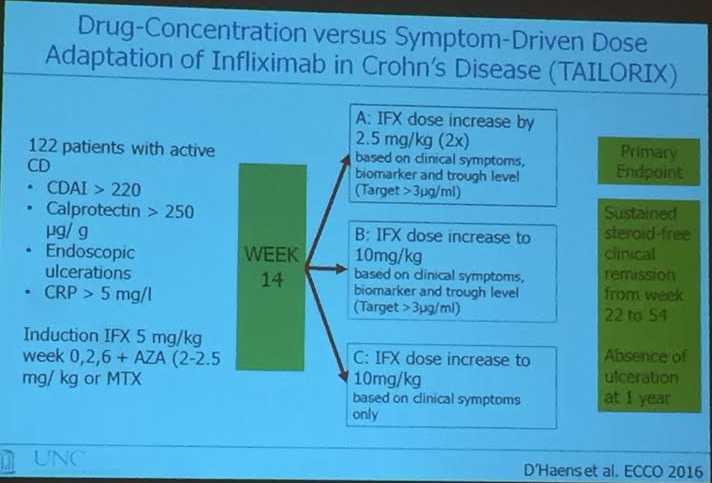

Hard to see Group C (clinically-based group) in this slide
Drug monitoring has become popular but its importance as a preemptive measure is unclear. Dr. Herfarth’s practice is to monitor when loss of response but not to monitor if doing well. His view: if someone is doing well, therapeutic drug monitoring can be confusing. It is not proven that optimizing drug levels will improve long-term outcomes. (In children, especially due to growth, drug monitoring may be more important.)
One other recommendation from Dr. Herfarth: he recommends combination therapy in his patients are started on a 2nd anti-TNFs.