After reading a few commentaries regarding value in medicine (which I will summarize tomorrow), it made me think a little more about value in pediatric gastroenterology.
I recently observed that a pediatric gastroenterologist in another group had a pattern of scheduling a lot of procedures. In pediatric gastroenterology, we are not doing endoscopies to screen for malignancy. The majority of children evaluated in our offices do not have organic disease. In addition, there are a number of variables that can be used to select patients who are most likely to benefit from evaluation. In fact, much of our value comes from this selection process, because non-physicians can be taught to be endoscopic technicians.
My reaction to this volume of cases was that I thought either this practitioner was seeing a ton of patients, had been away and had accumulated a number of cases, or that this was low value care. Though, another possibility is that the physician may be influenced by the “illusion of control” or “therapeutic illusion.” (NEJM full text: The Science of Choosing Wisely –Overcoming the Therapeutic Illusion). According to a recent editorial, “When physicians believe that their actions or tools are more effective than they actually are, the results can be unnecessary and costly care.”
“The therapeutic illusion is reinforced by a tendency to look selectively for evidence of impact — one manifestation of the “confirmation bias” that leads us to seek only evidence that supports what we already believe to be true.”
Whatever the circumstances with regard to endoscopy volume, my intent is not to single out an individual or specific group. My impression is that there are a lot more pediatric endoscopies being done these days and many are not needed. While I recognize that clinicians recommend endoscopy with a great deal of variation, my suspicion is that those who use endoscopy less frequently are likely to see similar outcomes. So, why are there so many low value endoscopies performed?
- The entire system is incentivized to do more procedures. Physicians and hospitals are compensated more for doing these procedures.
- Families and sometimes referring physicians think these procedures are necessary. In fact, there are studies that generally indicate higher levels of patient satisfaction when more diagnostic tests are done even if they are unnecessary.
- Physicians have a great deal of knowledge asymmetry in healthcare compared with families and it is expected that they will use their knowledge to help families pursue appropriate care. While all physicians may have some lapses, some physicians skirt this part of their job. One physician described this type of pediatric GI practice to me: “Scope first, think second.”
This blog has highlighted numerous aspects of health care economics. Pharmaceutical companies and hospitals have been criticized for gaming the system. The blog has discussed efforts to improve value like the “Choosing Wisely” campaign. Though, it is interesting to note that even with this campaign, most physician groups rarely identified areas that would affect their financial bottom-line. Among pediatric gastroenterologists, a frequent concern that I hear regards the overuse of CT scans by emergency room physicians.
When I take my car for repairs, I don’t want them doing an expensive overhaul unless it is really needed. If a car needs a muffler change, but the repairman recommended a few thousand dollars of repairs, that would be outrageous. Yet, in many cases with children, who are more precious than cars, the main difference with excessive endoscopic procedures, is that health insurance covers the majority of the costs.
I wonder too whether the frequency of endoscopy procedures actually discourages some families from having endoscopic procedures when they are clearly needed (eg. suspected celiac disease, suspected inflammatory bowel disease).
My take: Financial resources are limited. When physicians do not help utilize resources well, this results in poor care, whether families realize this or not. Ultimately, this will result in increased regulatory burdens for all physicians to more carefully justify what they are doing and/or result in efforts to eliminate financial incentives for unnecessary care. However, as noted previously (Do deductibles work to improve smart spending on health care?), financial incentives often affect both low value and high value care.
Any readers care to comment?
Related blog posts:
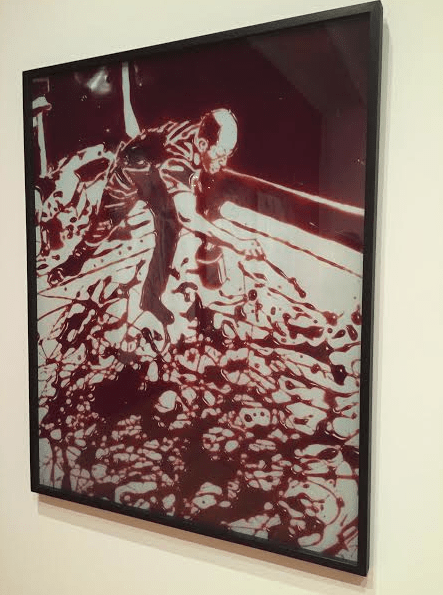
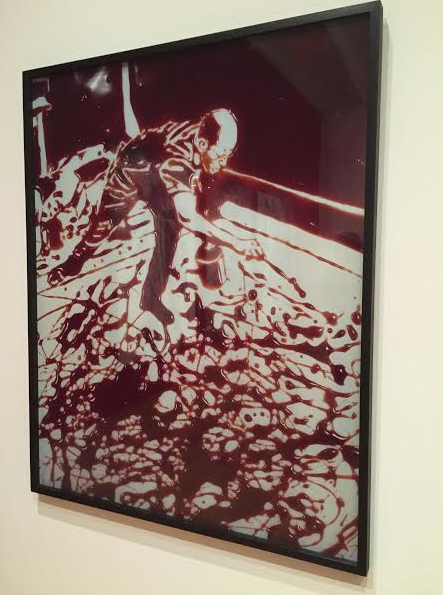
ViK Muniz Art -done completely from chocolate syrup -see the picture below for comparison.
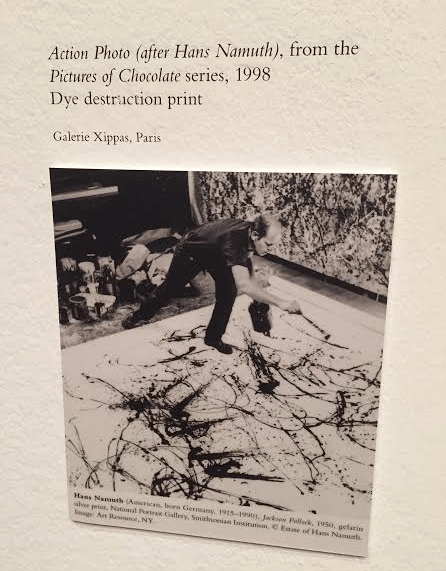
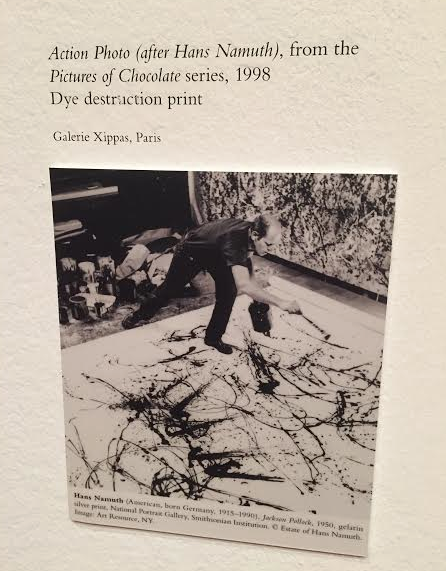
The Vik Muniz piece above is modeled after this photograph of Jackson Pollack