F Monge-Urrea, E Montijo-Barrios. JPGN 2022; 75: 391-395. Drug-induced Liver Injury in Pediatrics
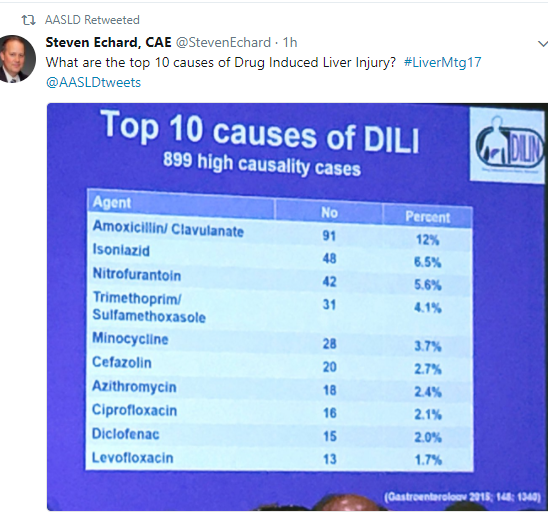
Background: Antibiotics and antiepileptics remain the most frequent causes of DILI. DILI may result in severe outcomes (eg liver transplant) in up to 5% of cases and could result in chronic liver disease in ~20%.
This is a terrific review -Figure 1 is particularly helpful. Figure 1 is an algorithm. Prior to using algorithm, review potential hepatoxcity by searching in NIH Livertox website. Next steps:
- Calculate pattern of injury (R score). R= ALT/ULN divided by ALP/ULN (ALP =alkaline phosphatase)
- Identify suspect drug. Hepatocellular (R >/=5), Mixed (R=2-5), Cholestatic (R</= 2). Examples of hepatocellular include acetaminophen, NSAIDs, Minocycline. Examples of mixed include azathioprine, and sulfasalazine. Examples of cholestatic include amoxicillin/clavulanate, and TMP/SMX
- Exclude alternative causes
- Calculate RUCAM Score (detailed in Table 1). This score can also be found at this link (open access): Overview of causality assessment in drug-induced liver injury
- Discontinue implicated drug and review specific therapies. For example, N-acetylcysteine for acetaminophen, and carnitine for valproate
- Consider liver biopsy only if suspected DILI progresses or fails to resolve on withdrawal of suspect drug (resolution can take 3-4 months)
Drug stop rules are reviewed:
- ALT or AST values that exceed 8 times the ULN
- ALT or AST values that exceed 5 times the ULN -hold medication for 2 weeks
- ALT or AST values >3 times the ULN and Bilirubin >2 times the ULN
- ALT or AST values that exceed 3 times the ULN with progressive nonspecific symptoms
Related blog posts:
- Data on Drug-Induced Liver Injury
- Augmentin Hepatotoxicity | gutsandgrowth
- Advice on drug-induced liver injury (DILI)
- Bookmark This Article on Pediatric Acute Liver Failure
- Liver Shorts -August 2020
- Predicting a Bad End in Drug-Induced Liver Injury | gutsandgrowthEd
- Liver Problems with Inflammatory Bowel Disease | gutsandgrowth

Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.