Background: “Placebo-controlled trials are especially important during the early phases of drug development, as use of placebo aids early detection of efficacy or futility.”
Methods: The authors performed a systematic review which identified 47 trials including 20,987 patients (14 267 [68·0%] receiving active drug and 6720 [32·0%] receiving placebo) were eligible. The studies involved multiple RCTs of biologics and small molecules in IBD.
Key findings:
The risks of worsening of IBD activity (Active treatment vs placebo: 563/13,473 [4·2%] vs 530/6252 [8·5%];RR 0·48)
Withdrawal due to adverse event (Active treatment vs placebo: 401/13 363 [3·0%] vs 299/6267 [4·8%]; RR 0·62)
Serious adverse event (Active treatment vs placebo: 682/14,267 [4·8%] vs 483/6720 [7·2%]; RR 0·69)
Serious infection (Active treatment vs placebo: 140/14 ,194 [1·0%] vs 91/6647 [1·4%]; RR 0·67)
Serious worsening of IBD activity (Active treatment vs placebo: 187/11,271 [1·7%] vs 189/5056 [3·7%]; RR 0·4)
VTEs (Active treatment vs placebo: 13/7542 [0·2%] vs 12/2981 [0·4%]; RR 0·45)
All of these adverse outcomes were significantly lower with active drug than placebo.
My take: Now that there are proven medications that are effective for moderate-to-severe Crohn’s disease, head-to-head trials of novel drugs against existing drugs with proven efficacy, rather than placebo-controlled trials, should be prioritized.
Doctors and pharmacists say the scorching temperatures enveloping the country could be endangering people’s health in an unexpected way: by overheating their medications.
Millions of Americans now receive their prescription medications through mail-order shipments, either for convenience or because their health plans require it. But the temperatures inside the cargo areas of delivery trucks can reach 150 degrees Fahrenheit in the summer, according to drivers — far exceeding the range of 68 to 77 degrees recommended by the national organization that sets standards for drug handling.
Mail-order pharmacies say that their packaging is weather resistant and that they take special precautions when medication “requires specific temperature control.” But in a study published last year, independent pharmaceutical researchers who embedded data-logging thermometers inside simulated shipments found that the packages had spent more than two-thirds of their transit time outside the appropriate temperature range, “regardless of the shipping method, carrier, or season…
Liquid medications like insulin or AUVI-Q, the epinephrine injection for allergic reactions, are often at heightened risk of degradation because excessive heat exposure can cause the evaporation of liquid components that were compounded at precise ratios. Aerosolized medications, too, are uniquely vulnerable because of the risk of pressure changes in the canister.
P.B.M.s [pharmacy benefit managers] often force mail order as the only option, constantly exposing our meds to destructive temperatures way outside the manufacturer’s specifications for days on end
My take: Worsening climate can even affect medication distribution. This article describes the consequences of medications affected by weather conditions including disease progression and liver transplant rejection. Lobbyists for P.B.M.s have effectively stifled regulations. For our patients with serious underlying diseases, mail-order medication efficacy is yet another concern. This NY Times article was published in August -hot weather is likely less of an issue at this time of year.
“Baxter International said it would temporarily close production at its North Cove, North Carolina-based facility, raising concerns about a potential nationwide shortage.”
“There are four primary manufacturers of IV fluids in the U.S. Baxter is the leader, accounting for about 60% of the market…In a statement published online Thursday, Baxter said it doesn’t yet have a timeline for when operations will be back up and running…A part of the problem, the company said, is that bridges to its site were damaged in the storm, limiting transport in and out.”
“The company is the main supplier for Mass General Brigham in Boston, which uses more than 100,000 liters of IV fluid from Baxter every month. On a call Thursday with reporters, Dr. Paul Biddinger, Mass General’s chief preparedness and continuity officer, said the health system received a letter from Baxter that said that due to the temporary closure, the system would receive only 40% of its usual supply from the manufacturer. “
My take: This is a nationwide problem and we need to conserve our supplies. This has happened before with Hurricane Maria hitting Puerto Rico in 2018.
Use oral fluids/rehydration fluids when possible in place of IV fluids
For many patients, IVFs can be used at lower rates or held overnight
Would try to complete IVF bags that were started in ED or OR when patient transitions to a hospital floor bed before changing to a new IV fluid bag
Nasogastric (NG) tube fluids can be administered more frequently
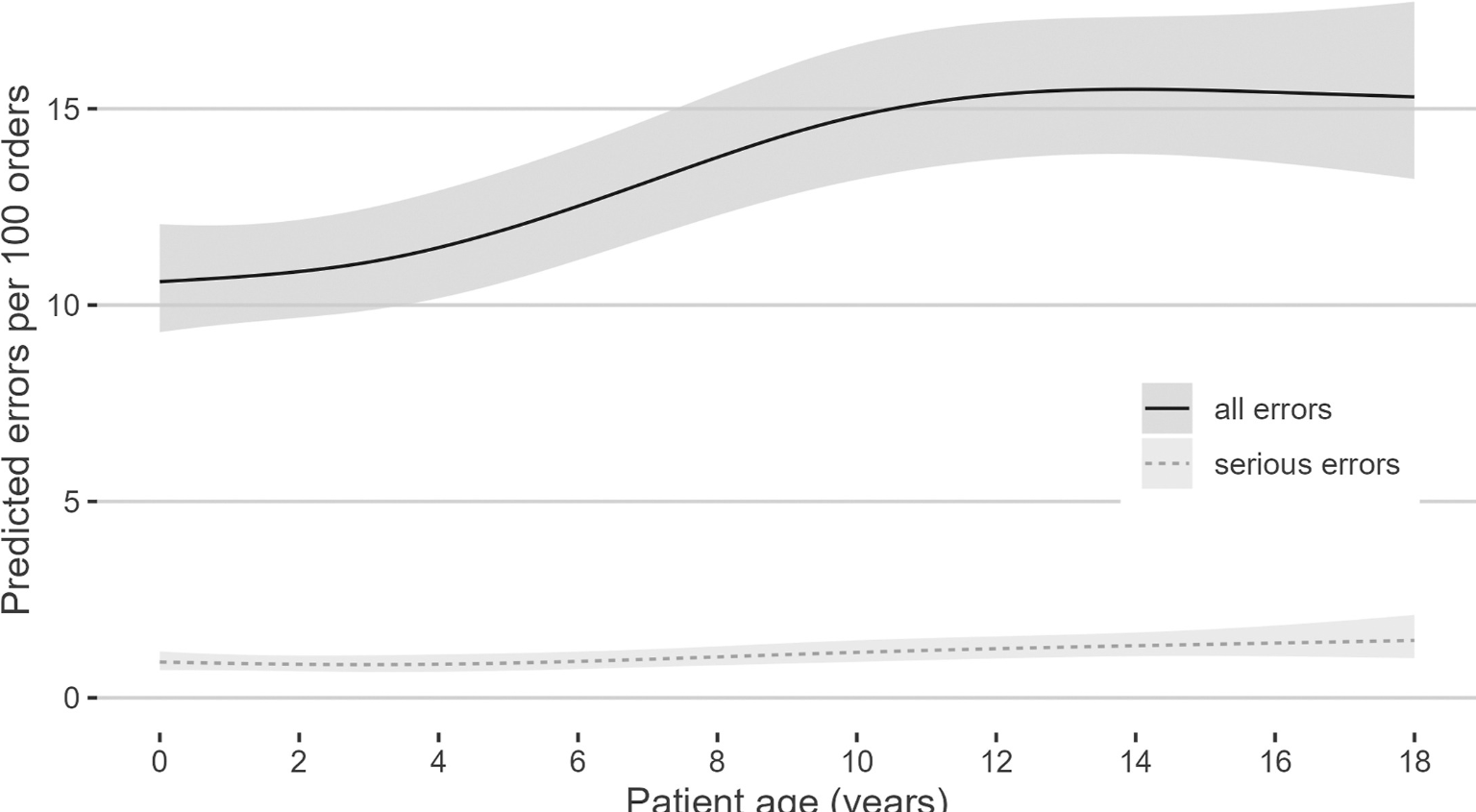
Methods: This study from Australia included (1) prescribing errors identified from chart reviews from two hospitals as well as (2) medication administration errors assessed by direct prospective observation of 5137 administrations at a single hospital. In total, this study examined almost 70 000 medication orders and more than 5000 medication administrations.
Key findings:
There was a modest increase in prescribing errors with age
There was a high rate of errors across all age groups. The crude error rate for prescribing was 18.6/100 orders
Hospital A had 14.5 prescribing errors per 100 orders using paper prescribing, and this increased to 17.6 per 100 orders during implementation of electronic prescribing then fell to 11.7 per 100 orders a year later.11 Prescribing error rates at hospital B were higher (28 per 100 orders in 2016, falling to 20 per 100 orders in 2020).
From the associated commentary (DM Goodman): “The Institute for Healthcare Improvement describe the 5 rights of medication administration –right patient, right drug, right dose, right route, and right time. But to achieve these goals, the right systems must also be in place.”
My take: This study makes me wonder what the error rate in our hospital is –I would think it would be much lower than the rates described in this study. This study makes me more appreciative of the occasional call I get from the pharmacist to adjust the dosing and the built-in alerts in our EMR.
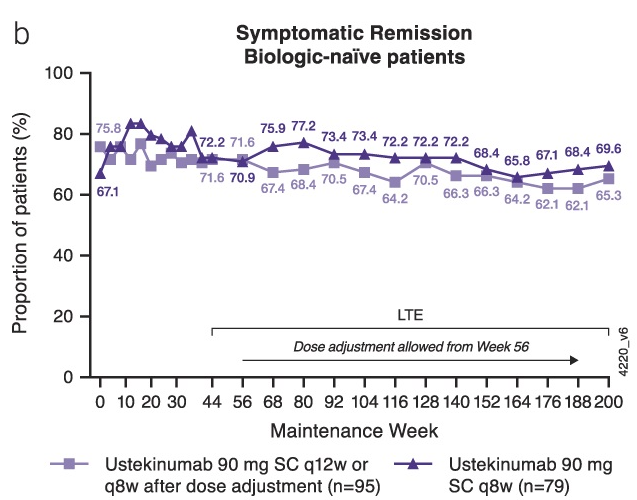
Background: In the initial UNIFI study, 44% and 38% remission rates were seen after 44 week treatment among patients with and without prior biologic exposure (See post: Ustekinumab for Ulcerative Colitis (UNIFI Trial)).
Methods: Ustekinumab induction responders who completed 44 weeks of maintenance treatment and agreed to enter the long-term extension continued their subcutaneous maintenance therapy (90 mg ustekinumab every 8 or 12 weeks [q8w or q12w] or placebo). Starting at week 56, randomized patients could receive dose adjustment to 90 mg q8w.
Key findings:
Of the 348 patients randomized to subcutaneous ustekinumab at maintenance baseline (q8w and q12w combined), 55.2% were in symptomatic remission at week 200.
A greater proportion of biologic-naive patients (67.2% [117/174]) were in symptomatic remission than those with a history of biologic failure (41.6% [67/161]).
Of the 171 patients with endoscopic evaluation at week 200, 81.6% (71/87) in the q12w group and 79.8% (67/84) in the q8w group had endoscopic improvement.
Safety: From weeks 156 to the final safety visit (up to week 220), no deaths, major adverse cardiovascular events, or tuberculosis occurred in patients receiving ustekinumab. Nasopharyngitis, UC worsening, and upper respiratory tract infections were the most frequently reported adverse events. “Exposure-adjusted analysis showed that ustekinumab AE rates were not greater than placebo.”
Immunogenicity: Overall, 5.5% (22/400) of randomized and nonrandomized patients who continued ustekinumab in the LTE were positive for ADA through the final safety visit. Overall, 5 of these 22 patients (22.7%) were positive for neutralizing antibodies. ADA were often transient and seemed to have no effect on efficacy.
My take: About ~25% of patients starting ustekinumab can expect to be in remission after 4 years based on this study. This estimate is based on a remission rate of ~55% at 200 weeks after achieving clinical remission in ~44% of the initial cohort patients at 44 weeks of treatment. The study provides additional data regarding a favorable safety profile.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
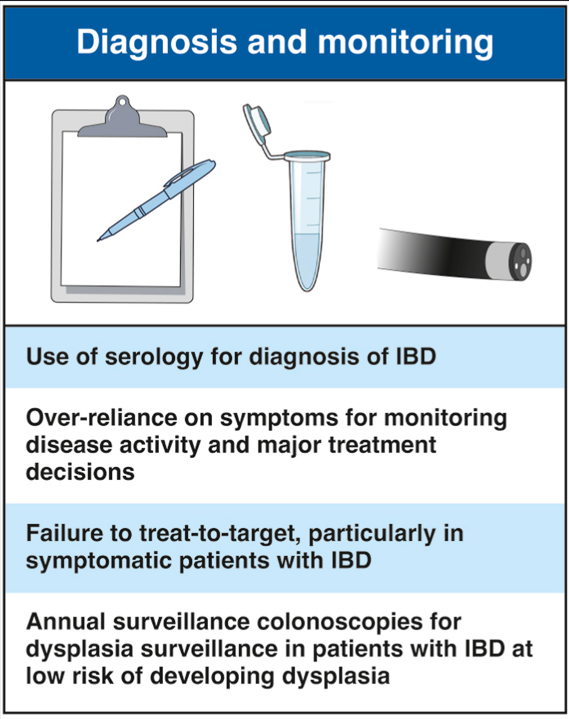
“Serological tests such as pANCA, ASCA, and other serological anti-microbial antibody tests for the diagnosis of IBD in patients with non-specific symptoms or in those with negative endoscopic and radiologic evaluation represents low-value care.“
“Making major therapeutic decisions based only on the presence of symptoms in patients with IBD, particularly CD, without objective confirmation of inflammation, represents low-value care. “
“Use of 5-ASA for the management of CD, particularly for patients at high risk of disease-related complications, represents low-value care. The safety of these medications must not be confused for their lack of efficacy in this setting. The utility of 5-ASA in a subset of patients with mild colonic CD who are at low risk of disease-related complications remains to be adequately studied.”
“Routine continuation of oral 5-ASA in patients with IBD who have been escalated to advanced therapies represents low-value care. Selective use of 5-ASA, particularly topical therapy in patients with persistent symptoms of proctitis despite optimized biologics may be appropriate.”
“Premature discontinuation of TNF antagonists in patients with IBD with partial but inadequate response or loss of response (after initial improvement) to index agent, without an attempt with accelerated dosing or therapeutic drug monitoring to potentially optimize therapy, represents low-value care.”
“Failure to consider dose de-escalation of TNF antagonists in patients who have achieved stable and persistent remission with intensive dosing regimens may represent low-value care.“
“Prolonged use of high-dose intravenous corticosteroidsbeyond5 to 7 days without significant clinical improvement, in patients hospitalized with ASUC, represents low-value care. In these patients, escalation to rescue medical therapy or surgery should be strongly considered.”
My take: If the comedian Jeff Foxworthy wrote this article, each of the opinions would have started off with ‘You might be wastin money if…’
In June, risankizumab (Skyrizi) received FDA approval as a treatment for moderate to severe ulcerative colitis in adults. FDA approval relied on the data from these two randomized trials.
Methods: For the induction trial, patients were randomized 2:1 to receive 1200 mg of risankizumab or placebo administered intravenously at weeks 0, 4, and 8. For the maintenance trial, patients with a clinical response (determined using the adapted Mayo score) after intravenous treatment with risankizumab were randomized 1:1:1 to receive subcutaneous treatment with 180 mg or 360 mg of risankizumab or placebo (no longer receiving risankizumab) every 8 weeks for 52 weeks.
Key findings:
In the 12-week induction INSPIRE study with 975 patients, the clinical remission rates at week 12 were 132/650 (20.3%) for 1200 mg of risankizumab and 20/325 (6.2%) for placebo (P < .001)
In the induction trial, a greater proportion of treated patients achieved endoscopic improvement (36.5% vs. 12.1%; P < 0.00001) and endoscopic histologic mucosal improvement (24.5% vs. 7.7%; P < 0.00001) after 12 weeks
In the induction trial, a clinical response at 12 weeks was noted in 418/650 (64.3%) of risankizumab-treated patients and 116/325 (35.7%) of the placebo-treated patients
In the COMMAND maintenance trial with 548 patients, the clinical remission rates at week 52 were 72/179 (40.2%) for 180 mg of risankizumab, 70/186 (37.6%) for 360 mg of risankizumab, and 46/183 (25.1%) for placebo. Both doses were statistically-significant compared to placebo, P < .001 and P = .002, respectively
After 1 year of treatment with either maintenance dose of risankizumab, more than 40% of patients had histologic and endoscopic improvement
More than 75% of patients in the maintenance trial had a history of inadequate response to advanced therapies
My take: The published results of risankizumab for Crohn’s disease are much more impressive than the results in this study.
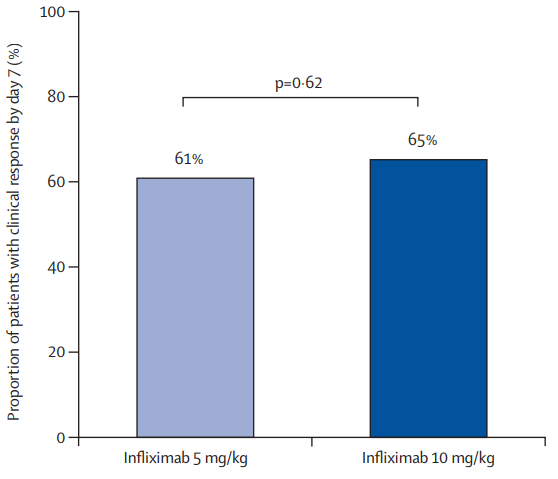
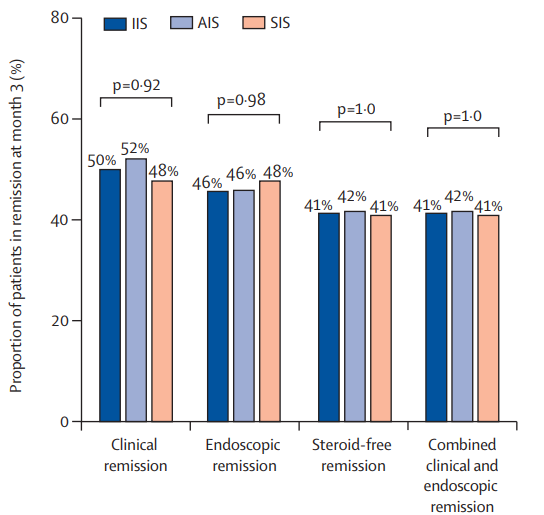
Methods: In this open-label, multicenter, randomized controlled trial, patients aged 18 years or older from 13 Australian tertiary hospitals with intravenous steroid-refractory ASUC were randomly assigned (1:2) to receive a first dose of 10 mg/kg infliximab or 5 mg/kg infliximab (randomization 1). Block randomization was used and stratified by history of thiopurine exposure and study site, with allocation concealment maintained via computer-generated randomization. Patients in the 10 mg/kg group (intensified induction strategy [IIS]) received a second dose at day 7 or earlier at the time of non-response; all patients in the 5 mg/kg group were re-randomized between day 3 and day 7 (1:1; randomization 2) to a standard induction strategy (SIS) or accelerated induction strategy (AIS), resulting in three induction groups. Patients in the SIS group received 5 mg/kg infliximab at weeks 0, 2, and 6, with an extra 5 mg/kg dose between day 3 and day 7 if no response. Patients in the AIS group received 5 mg/kg infliximab at weeks 0, 1, and 3, with the week 1 dose increased to 10 mg/kg and given between day 3 and day 7 if no response.
Thus, this was the first RCT comparing an intensified induction strategy (IIS; 10 mg/kg infliximab at weeks 0 and 1, with the second dose given earlier if no clinical response), an accelerated induction strategy (AIS; 5 mg/kg infliximab at weeks 0, 1, and 3, with the second dose increased to 10 mg/kg and given earlier if no response), and a standard induction strategy (SIS; 5 mg/kg at weeks 0, 2 and 6; with an extra 5 mg/kg dose before day 7 if no response) in steroid-refractory patients with ASUC.
Key findings:
There was no significant difference in the proportion of patients who had a clinical response by day 7 between the 10 mg/kg and 5 mg/kg groups: 65% vs 61%
In patients with a baseline albumin of less than 25 g/L, a day 7 response occurred in nine (64%) of 14 patients in the 10 mg/kg group versus 14 (45%) of 31 in the 5 mg/kg group (RR 1·43, p=0·17)
In patients with a baseline CRP of 50 mg/L or higher, a day 7 response occurred in six (60%) of ten patients in the 10 mg/kg group versus eight (42%) of 19 in the 5 mg/kg group (RR 1·39, p=0·34)
The proportions of patients with clinical response at day 14: 74% in the IIS group, 73% in the AIS group, and 68% of 44 in the SIS group.
The clinical remission at month 3: 50% in the IIS group, 52% in the AIS group, and 48% in the SIS group
The steroid-free remission at month 3: 41% in the IIS group, 42% in the AIS group, and 41% in the SIS group
The endoscopic remission at month 3: 46% in the IIS group, 46% in the AIS group, and 48% in the SIS group
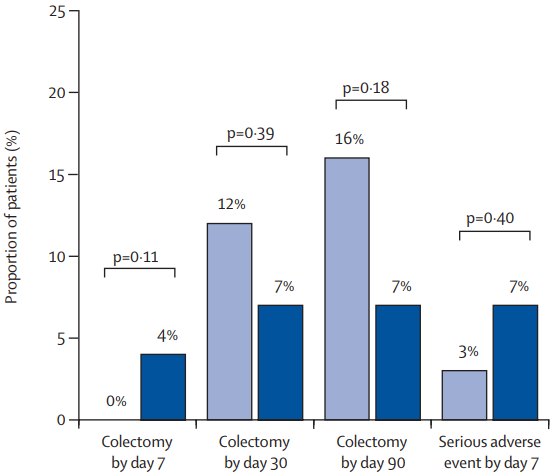
The colectomy rate at month 3: 7% in the IIS group, 19% in the AIS group, and 12% in the SIS group colectomy at month 3 were not significantly different between group (P=0.20)
The colectomy rate at month 12: 7% in the IIS group, 22% in the AIS group, and 15% in the SIS group colectomy at month 3 were not significantly different between group (p=0.13)
In post-hoc analysis of second-dose salvage strategies (among the group who had not responded at day7), a clinical response was observed in 19 (59%) of 32 patients who received a 10 mg/kg salvage dose versus nine (64%) of 14 who received a 5 mg/kg salvage dose (RR 0·92). Endoscopic remission at month 3 was observed in 11 (34%) who received 10 mg/kg salvage versus six (43%) who received 5 mg/kg salvage (RR 0·80). Colectomy by 3 months occurred in ten (31%) who received 10 mg/kg salvage compared with three (21%) who received 5 mg/kg salvage (HR 1·46)
Higher proportions of patients with clinical and biochemical remission between weeks 2 and 6 were apparent in the IIS and AIS groups versus the SIS group, but by 3 months, these differences were lost
My take: Intensified, accelerated, and standard induction regimens in the PREDICT-UC study did not result in a statistically-significant difference in clinical response by day 14 or in remission or colectomy rates by month 3. However, there are some important caveats:
There appeared to be a trend towards a lower colectomy rate in the IIS group.
There appeared to be a favorable trend towards an improved response to IIS group in those with low albumin (<25 g/L) and high CRP (>5 mg/L). The smaller numbers in these subgroups could have precluded statistical significance
Also, even the SIS group were able to receive a 4th induction 5 mg/kg dose between days 3-7 if they had not responded to treatment
In patients who had not responded to either 10 mg/kg or 5 mg/kg, a salvage dose at day 7 resulted in a >60% response rate
It is possible that a sustained strategy of more aggressive dosing (not done in this study) aided with therapeutic drug monitoring could result in better outcomes following IIS
This article describes trends and rationale for consolidation of gastroenterology practices.
Trends:
“From 2012 to 2022, the share of physicians who work in private practices dropped 13 percentage points, from 60.1% to 46.7%.” (In the 1980s, 76% of physicians owned their practice)
“Ownership among physicians younger than 45 dropped more than 12 percentage points from 2012 to 2022, from 44.3% to 31.7%.”
My Views (in bold) on the Authors’ Rationales for Consolidation:
“The potential advantages of consolidation include achieving economies of scale, increasing choices for patients beyond large hospital-based systems of care, enhancing the infrastructure to support high-quality value-based independent practices…whereas drawbacks …diminished authority.” The driving force for consolidation is money not improvement in “high-quality value-based” care. PE investors are tapping into health care to extract profits from the healthcare sector.
“The long-term implications for individual practices, physicians and patient care remain uncertain.” Some of the implications are already evident –increased costs for patients and without improvement in quality. PE consolidation does allow improved negotiation with insurers and hospitals.
“Large PE-backed groups provide resources to help independent practices stay independent.” This is quite a paradox. PE acquisition is a not a way to maintain independence.
My take: While consolidation, driven by financial incentives, is affecting all areas of healthcare, it is NOT resulting in improvement in patient care or physician satisfaction. This is true whether consolidation is acquisition by private equity or by hospitals. This article’s attempt to provide a different narrative is BS.
As an aside, in some ways, acquisition by hospitals is harder to justify than acquisition by PE; hospitals state that their main goal is patient care. Yet, when hospitals consolidate physician practices, this often runs counter to that goal by increasing costs for patients without improvement in quality.
In this prospective cohort study from Boston Children’s (2017-2022, n=157), the authors examined diagnostic evaluations in children presenting with Brief Resolved Unexplained Events (BRUEs).
Key findings:
Only 28% (20% during the hospitalization, 8% afterwards) underwent VFSS with 71% abnormal.
42% of infants had their BRUE attributed to GERD, and 33% were treated with acid suppression during follow-up
Provision of GERD diagnosis was associated with a delay in making an aspiration diagnosis. 10% (6/66) of patients with “GERD” diagnosis subsequently had swallow studies –all were abnormal. Mean diagnostic delay was 56 days.
Discussion points:
The approach of using symptoms to determine evaluation of BRUEs has been advised by AAP clinical practice guidelines (2016 & 2019); “however, our results suggest that reliance on these clinical characteristics may result in negative outcomes.”
Most aspiration in infants is silent aspiration and not detected by clinical feeding evaluation (CFE) in the absence of a VFSS. “It is concerning that 63% of patients had CFE alone without confirmatory VFSS in the present cohort, and it may be that this practice is even more common in other centers.” Silent aspiration can lead to repeat hospital visits and even long-lasting pulmonary damage including bronchiectasis.
Clinicians cannot diagnose aspiration based on history or bedside feeding evaluations. Objective testing (e.g. VFSS) is needed if there are concerns for dysphagia
Inappropriate diagnosis of GERD may cause harm. GERD medications have been associated with increased infections and may increase risk for allergies.
The role of aspiration in causing BRUEs has been well-recognized since 2017 (see below) by the same group in Boston. It is likely that evaluation of dysphagia is even less frequent in other medical centers.