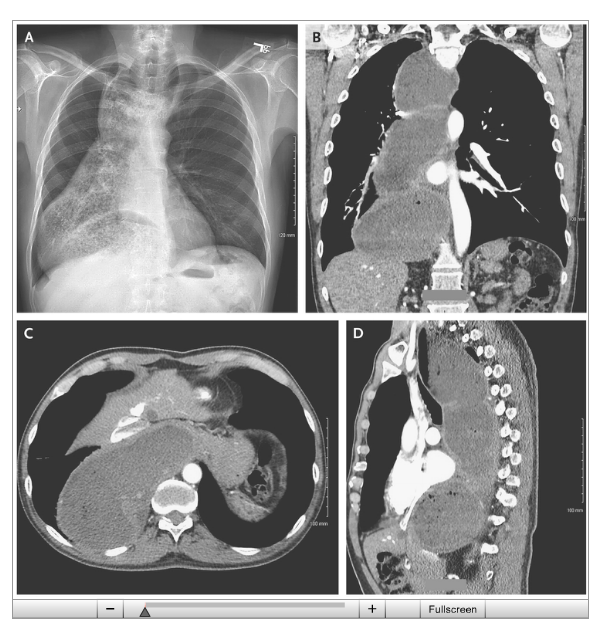
From NEJM twitter feed: Achalasia with Megaesophagus (in a 63 yo)
Related blog posts:

The ability to use whole exome sequencing and widely available genetic testing is yielding a plethora of new information regarding the genetic causes for many conditions. In gastroenterology, here are a few recent examples:
For me, I am not sure whether these findings should be considered mundane or amazing. On the one hand, each of the findings helps understand these diseases; yet, I came across all of these articles in the span of 24 hours and from the same journal.
From APFED twitter feed: What does the Food Allergen Labeling and Consumer Protection Act require?: http://youtu.be/nhBd9iTYkUQ?a (<2 minute video)
Plus one more reference on Achalasia:
A recent review on achalasia highlights the recent advances in our understanding of this disorder (Gastroenterol 2013; 145: 954-65). This post is mainly to note it as a useful reference.
Specific topics covered include the following:
Related posts:
As noted in a previous blog regarding NOTES (see link below), peroral endoscopic myotomy (POEM) has been investigated for treatment of achalasia. Now, a prospective study of 70 patients from 5 centers reports excellent results (Gastroeenterol 2013; 145: 309-11, editorial 272-73).
Results:
Potential benefits of POEM:
Early results suggest similar efficacy to surgery but with the recovery profile of an endoscopy Painless
For more widespread adoption, many questions need to addressed:
Related blog posts:
A concise review with good pictures, graphics and references:
Clin Gastroenterol Hepatol 2013; 11: 887-97.
Related post:
EPT for Achalasia | gutsandgrowth
EPT or esophageal pressure topography (using high-resolution manometry) can help predict outcomes for achalasia (Gastroenterol 2013; 144: 718-25, editorial 681-83).
Background: Patients with achalasia often present with dysphagia, chest pain, and regurgitation. These symptoms result from impaired lower esophageal sphincter relaxation and aperistalsis. While the main treatment has focused on disruption of the sphincter, esophageal body pressures may be important in long-term outcomes.
Three patterns of esophageal body pressures with achalasia:
According to the cited study which reviewed data from 176 patients in the European achalasia trial (time period: 2003-2008, 18-75 year old), success rates were better with type 2 achalasia (96%, n=114) compared with type 1 (81%, n=44) or type 3 (66%, n=18).
In addition, the EPT findings may influence treatment selection. Pneumatic dilation (PD) was more successful than Heller myotomy (HM) for type 2 patients (100% vs. 93%, p < 0.05). However, HM was considered successful more frequently for patients with type 3 achalasia (86% vs. 40% –though not statistically significant due to small numbers). For type 1, no significant difference was noted between HM and PD at 2 year followup, 81% vs. 85% respectively.
The commentary discusses some of the pertinent issues. For example, HM may be better than PD among type 1 patients; the exclusion of patients with severe dilatation of esophagus.
Take-home message (from editorial) “The task at hand is to determine whether these distinct categories truly matter in clinical practice…it seems that the subtypes of achalasia do have prognostic value…we …need to determine…whether subtypes can inform treatment options.”
