L Sims et al. JPGN 2024;79:1040–1046 Open Access! Eating concerns in youth with functional abdominal pain disorders
This retrospective cohort included 270 adolescents/young adults who attended an intensive, interdisciplinary pain treatment program, including 135 youth with functional abdominal pain (FAP) and an age- and gender-matched control group with a primary pain diagnosis of chronic headache.
Key findings:
- Limitation of this study: The population attending this intensive pain program is NOT representative of typical outpatient setting
- A history of an eating disorder was more common with FAP than in those with chronic headache (15.4% vs. 5.9%)
- In this cohort, patients with FAP compared to patients with chronic headache had higher rates of prior exclusion diets to manage their symptoms (46% vs. 22%, p = 0.007), and prior requirement enteral or parenteral feeds (18% vs. 1.5%, p = 0.001)
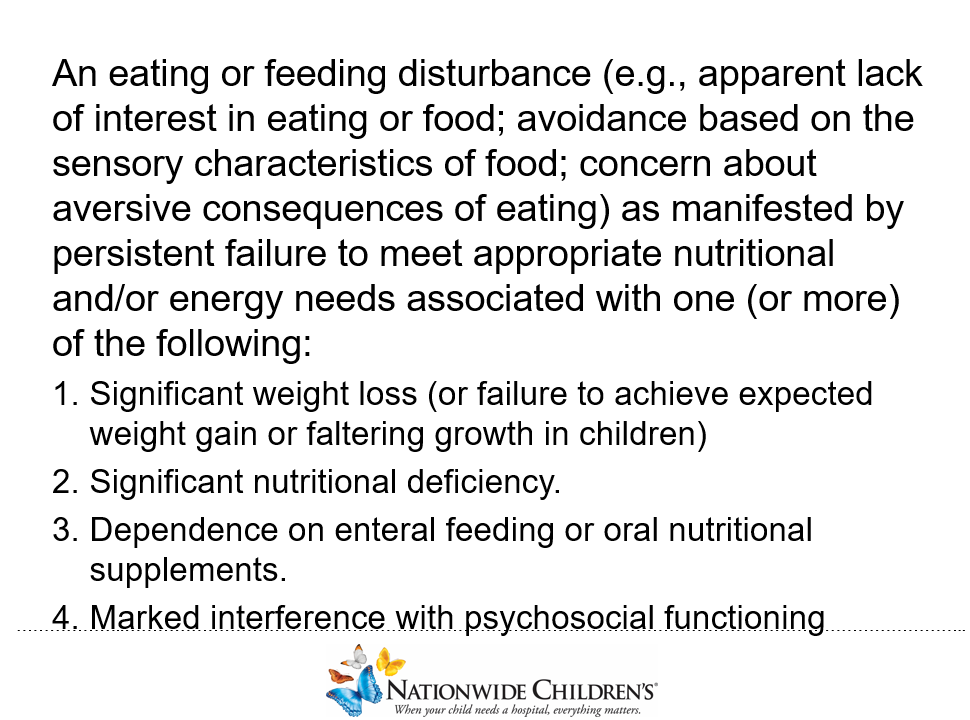
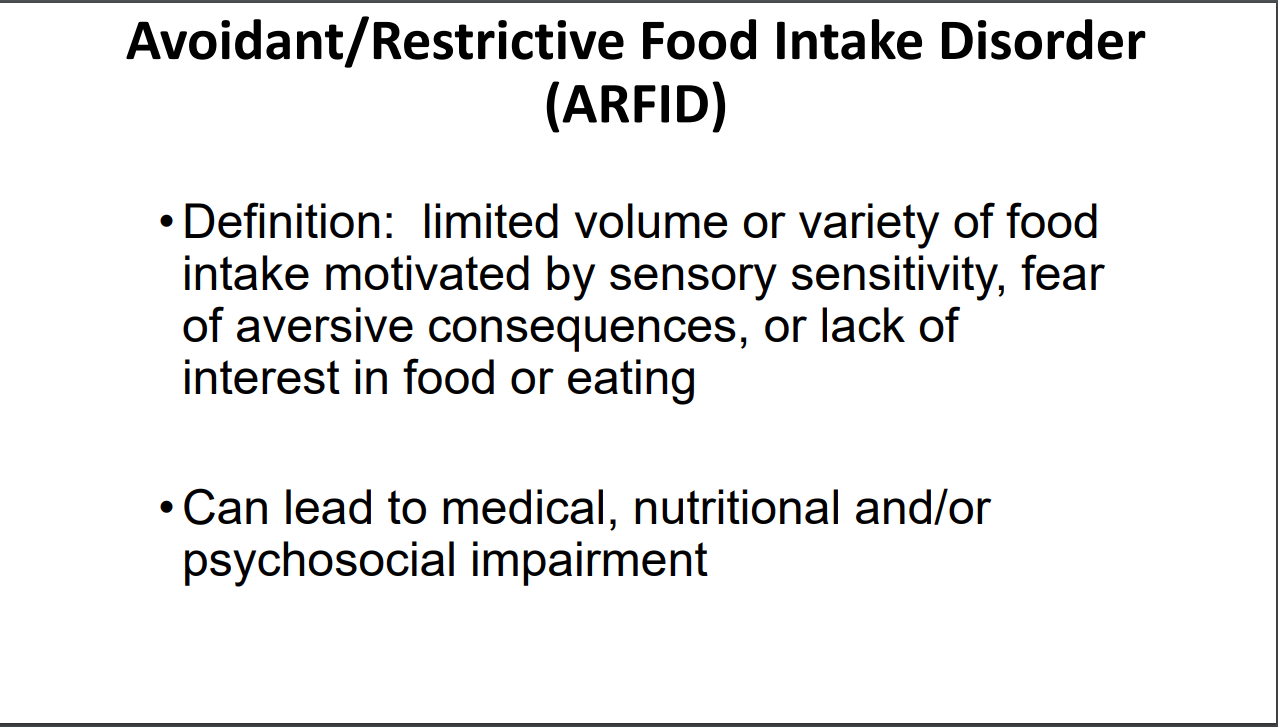
- The study found a significant association between a history of exclusion diets and meeting criteria for ARFID. “With regard to ARFID, the prevalence of patients in both groups who met diagnostic criteria (FAP: 50%; chronic headache: 36%) was also significantly higher than estimates from the general school-aged population (3%)”
- Patients with FAP were also more likely than patients with chronic headache to be diagnosed with postural orthostatic tachycardia syndrome ([POTS]; 46% vs. 30%) and have a history of food allergies or intolerances (43% vs. 25%)
- Significantly more adolescents with FAP (n = 68) than chronic headache (n = 45) had lost 4.5 kg or more, p = 0.004
My take: Most treatments for FAP, including dietary treatment, have some inherent risks. In patients placed on dietary therapies, screening and/or discussing the risk of dietary restriction need to be considered.
Related blog posts:
- Avoidant/Restrictive Food Intake Disorder (ARFID) with Irritable Bowel Syndrome and with Inflammatory Bowel Disease
- Mel Heyman: Past, Present and Future of ARFID
- Prevalence of Avoidant/Restrictive Food Intake Disorders in Pediatric Neurogastroenterology