- X Gu et al. AJG 2024; 119: 2288-2297. Effects of Retrograde Colonic Enema-Based Fecal Microbiota Transplantation in the Treatment of Childhood Constipation: A Randomized, Double-Blind, Controlled Trial
- M Stefano. AJG 2024; 119: 2187-2188 (Editorial). Fecal Microbiota Transplantation in the Treatment of Severe Constipation in Children: Is It the Future?
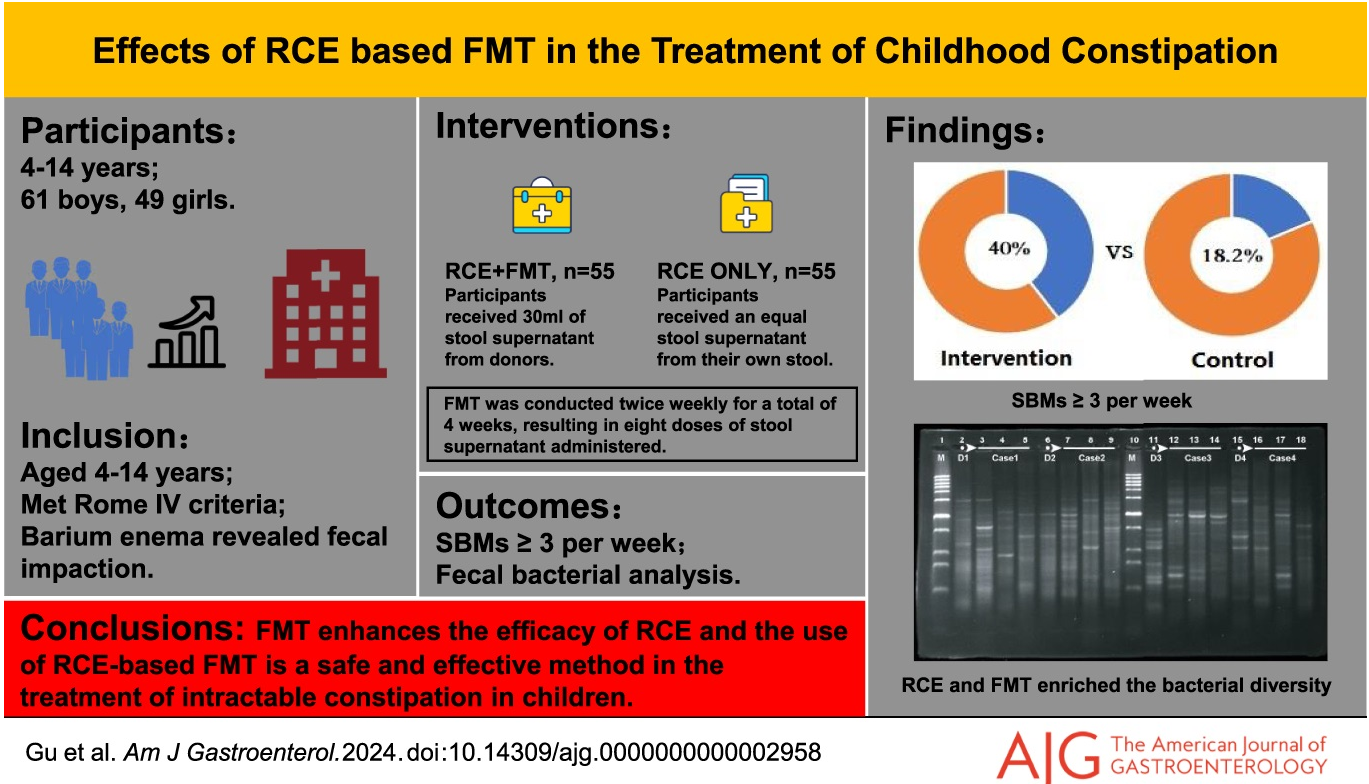
Methods: The efficacy of retrograde colonic enema (RCE) with fecal microbiota transplantation (FMT) was studied in a randomized, double-blind, controlled trial with 110 children. The initial cohort recruited was 576 patients; however, 466 were excluded for not meeting inclusion criteria. All participants received a daily RCE, followed by a 4-week FMT treatment (twice a week) and a 12-week follow-up period.
Key findings:
- At the end of the follow-up period, 22 patients (40.0%) in the FMT with RCE group and 10 patients (18.2%) in the placebo with RCE group had ≥ 3 spontaneous bowel movements per week
There was a low response to RCE alone which the authors attributed in part to the severity of constipation in the cohort. It is unclear the degree of compliance with the treatment protocol which was done in the home setting. There was a prior open-label study with NJ FMT which improved constipation in half of participants.
My take: Modulating the microbiome can have beneficial effects on stool frequency. This can be through diet and possibly FMT in severe cases of constipation. The availability of capsules could make this type of therapy easier but perhaps less palatable. Even if FMT proves to be a useful treatment, the optimal treatment regimen is not clear.
Related blog posts:
- OpenBiome Suspending FMT Shipments
- FMT Research & The Shawshank Redemption
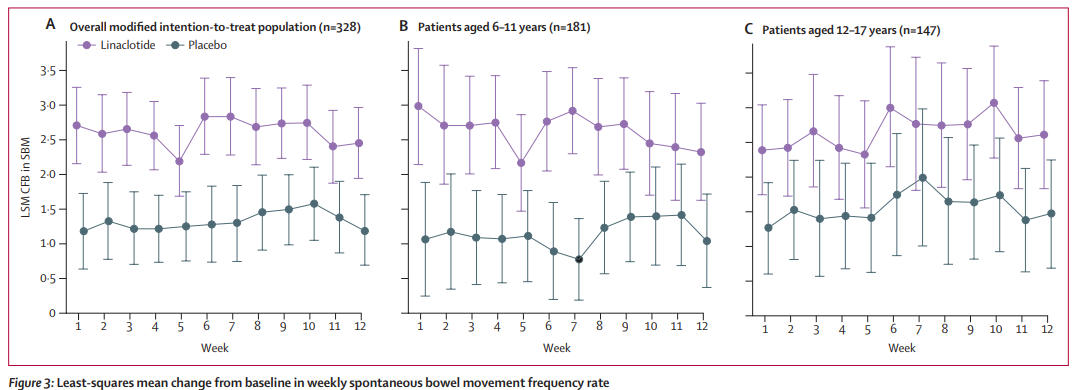
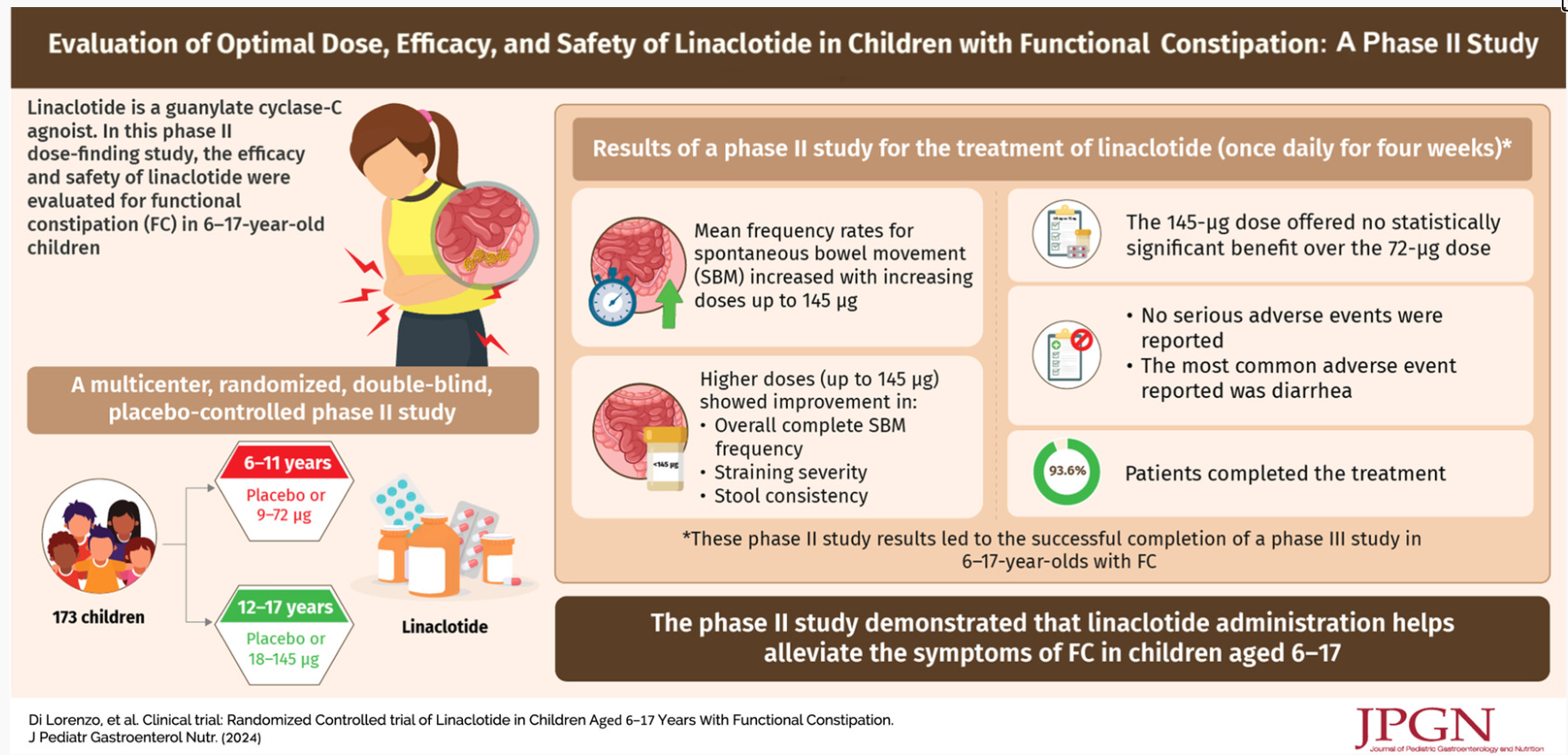
- Linaclotide -Here’s the Pediatric Data
- “Real-world” Efficacy for Fecal Microbiota Transplantation
- The Link Between Ultra-Processed Foods and Irritable Bowel
- How to Change Your Microbiome Quickly?
- What’s in Your Gut and How to Change It
- Can We Predict Which Patients With Irritable Bowel Will Respond to Dietary Manipulation Based on Their Microbiome?