KR Arellanos et al (Senior Author S Bonilla). JPGN Reports. 2026;7:19–27. Standardizing a protocol for Helicobacter pylori gastric biopsy culture: From implementation to sustained practice
Background: “The availability of antibiotic susceptibility data is essential for understanding local and regional resistance patterns and for informing future guidelines on optimal treatment regimens for children.” This quality improvement project report documents how “using a standardized checklist, in combination with educational initiatives for staff physicians and collaborative efforts with endoscopy and laboratory teams, were effective strategies to increase the use of gastric biopsy culture as a diagnostic tool for H. pylori infection and, to a lesser extent, to improve culture yield in patients with positive histology.”
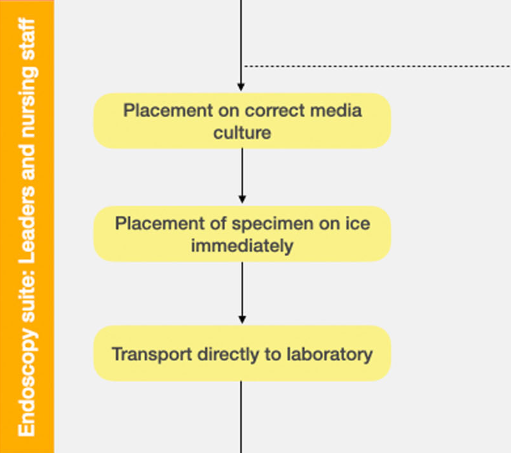
Key steps:
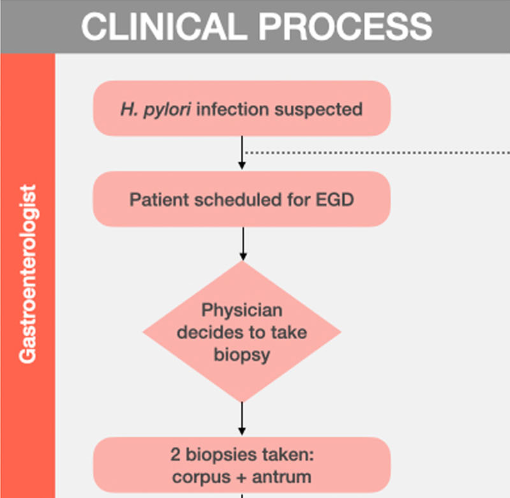
- Standardized checklist for biopsy collection used by nurses
- Standardized transport protocol
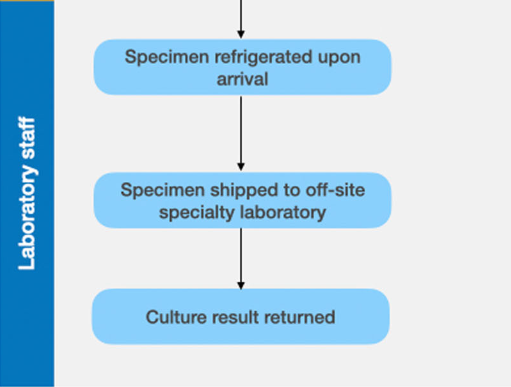
- Prompt refridgeration/transportation
- Using a single lab for testing (Mayo clinic)
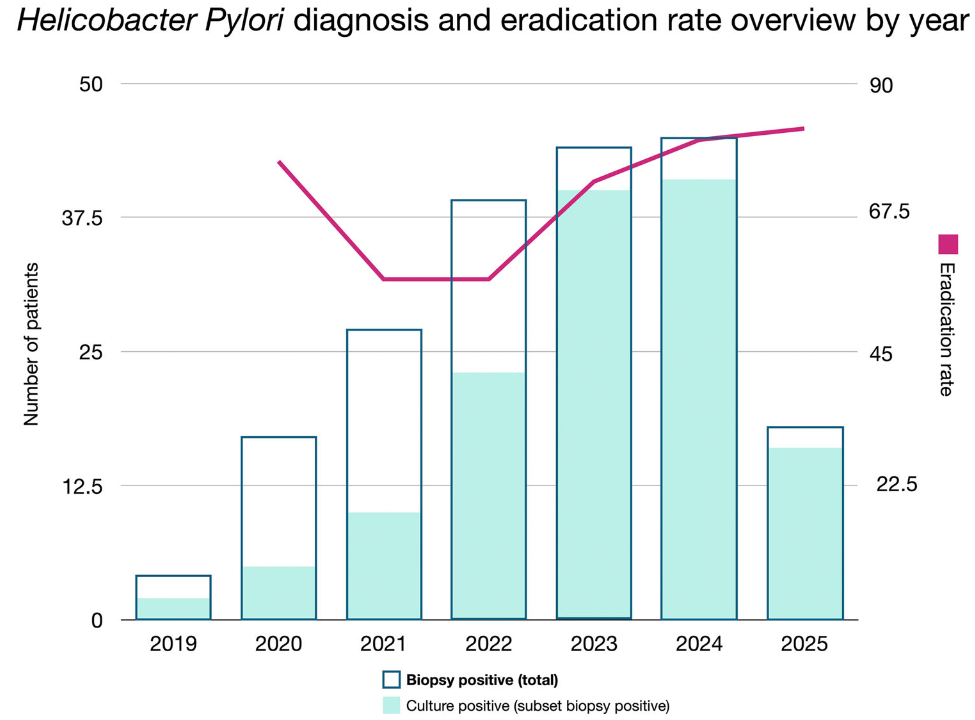
Key findings:
- There was a consistent increase in culture positivity for H pylori and this was associated with improved eradication rates
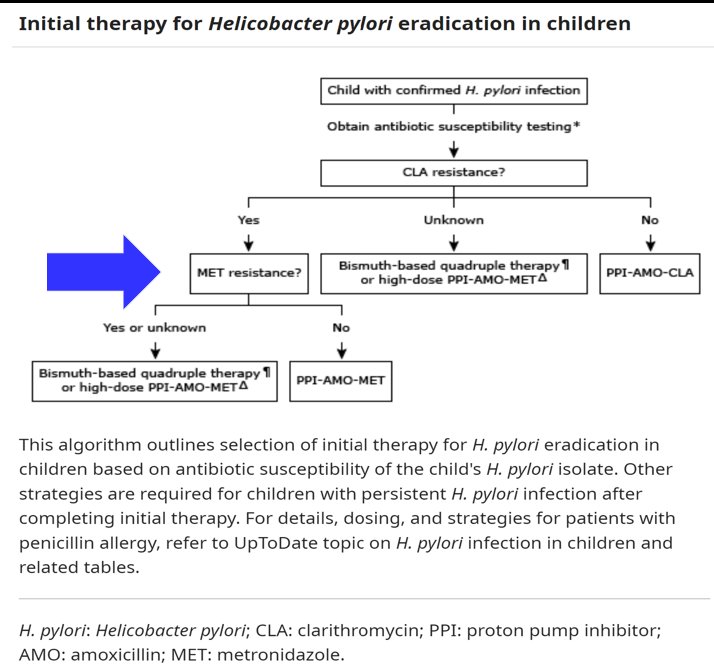
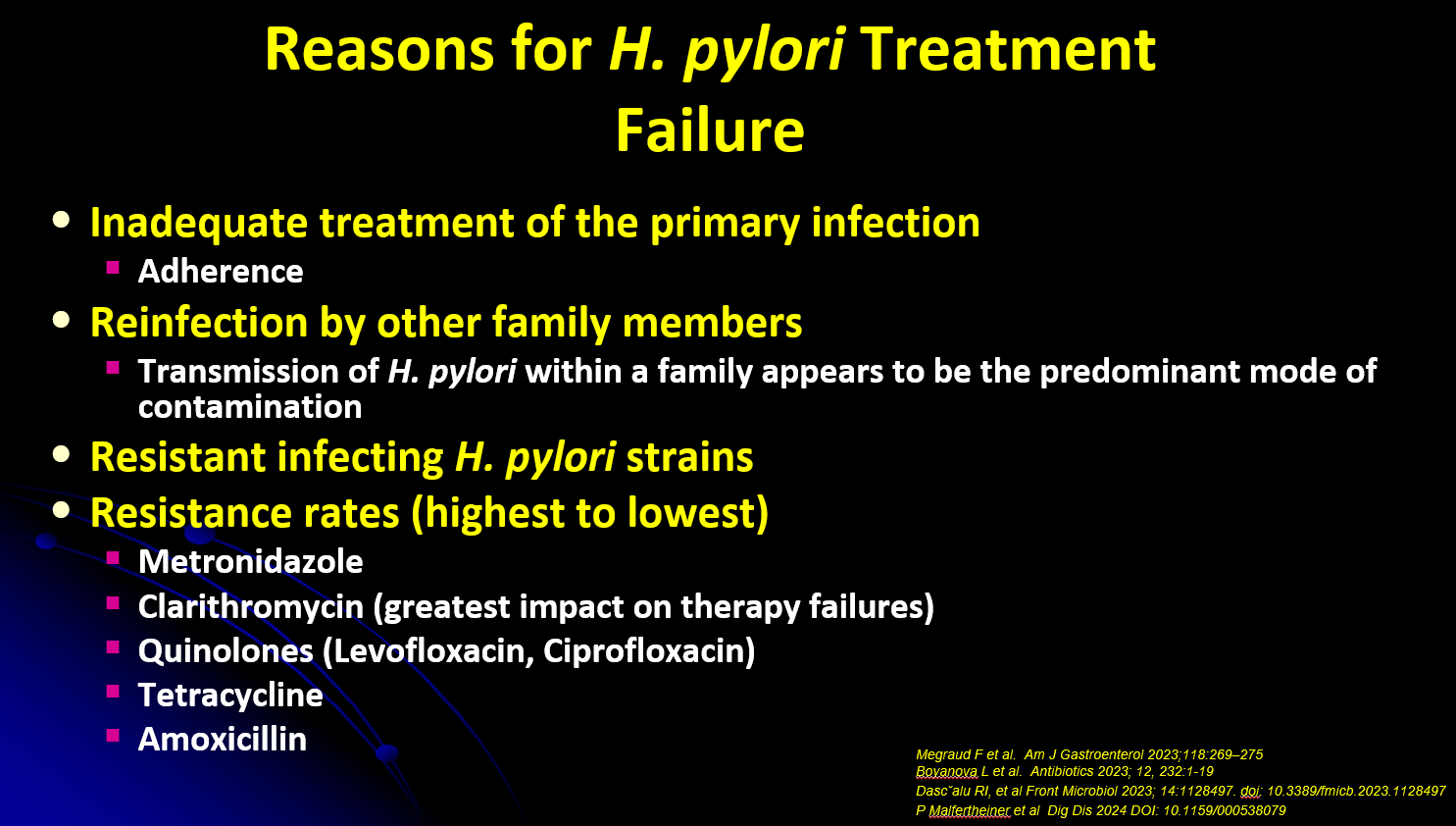
- Overall, antimicrobial resistance was highest for metronidazole (27.5%) and clarithromycin (18.7%), and lower for rifampin (12.2%), levofloxacin (10.1%), and amoxicillin (4.3%). Only one isolate showed resistance to tetracycline
Discussion: “Among the various interventions implemented during the QI project, the one that appears to have contributed most significantly to the dramatic improvement in culture yield among patients with H. pylori-positive histology was the consolidation of specimen processing to a single specialty laboratory [Mayo clinic].” Specific logistics included using a simple sterile container with saline-moistened tissue for collection and sending samples to specialty lab on the same day as collection.
My take: During this project, there was improved use of gastric culture and in culture yield. This resulted in meaningful improvement for patients. However, without clinical leadership to implement these changes, there will continue to be suboptimal eradication rates at other centers.
Related blog posts:
- H Pylori Study Methods
- 5 Rights and H pylori Treatment
- How To Achieve Helicobacter Pylori Cure Rates of >95%
- Give the Right Dose (for H pylori) -It Works Better!
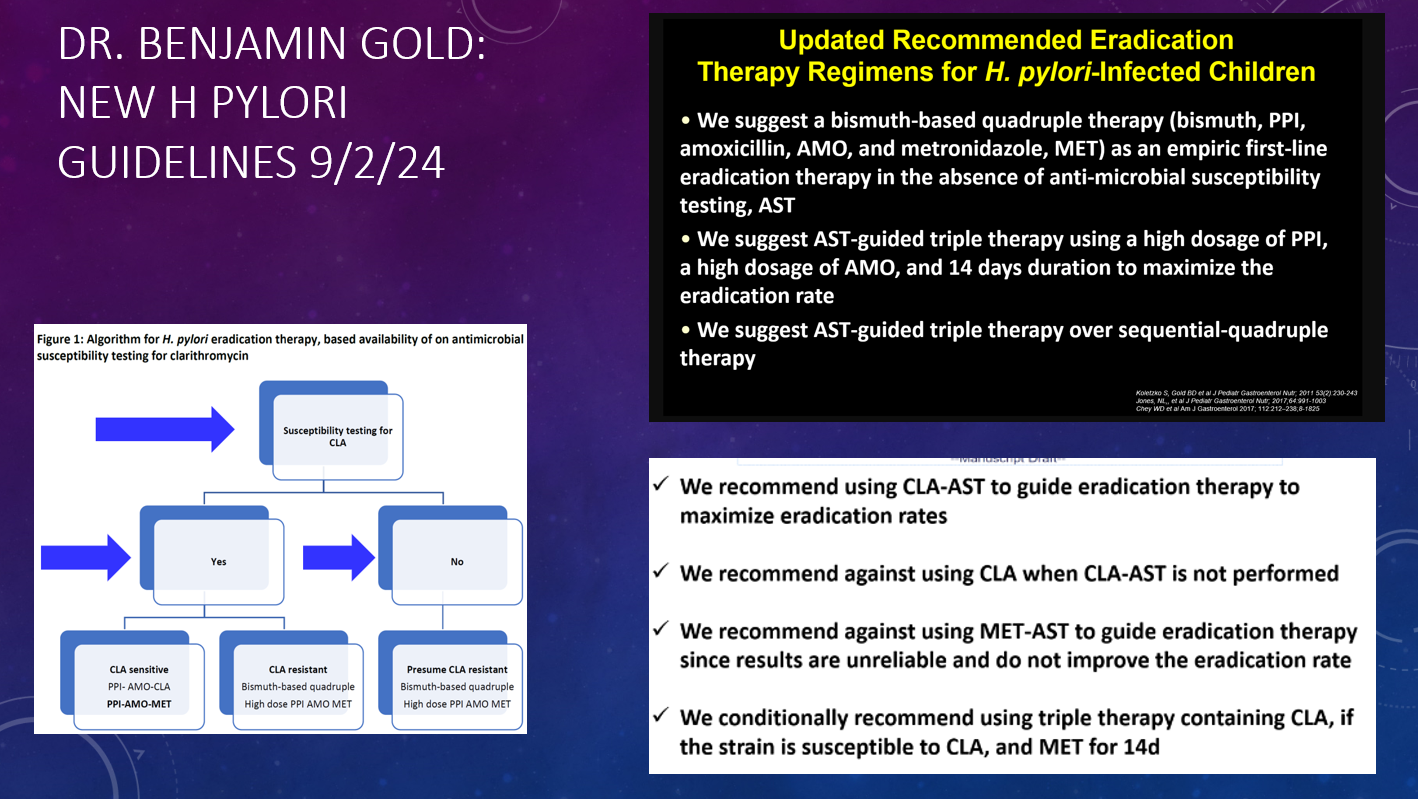
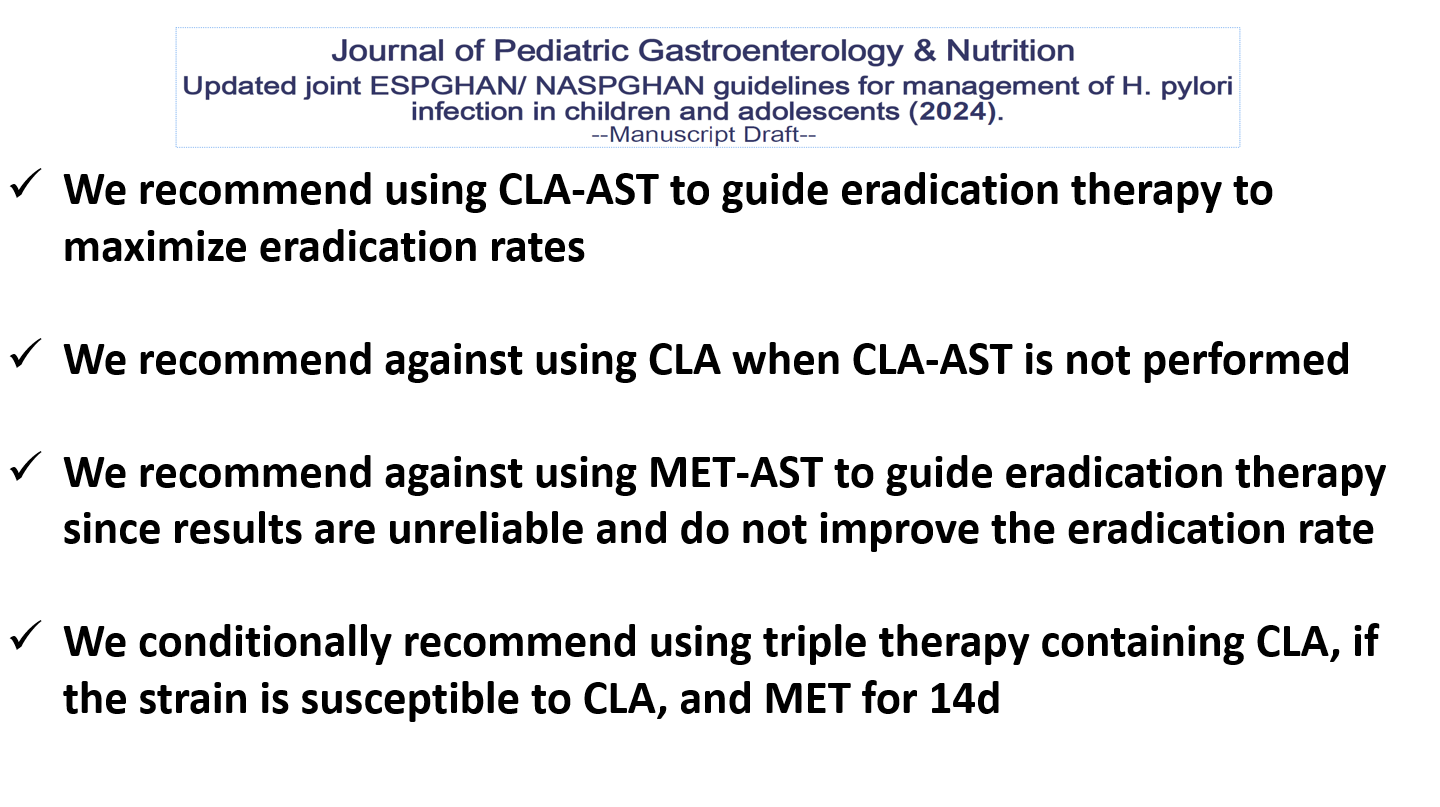
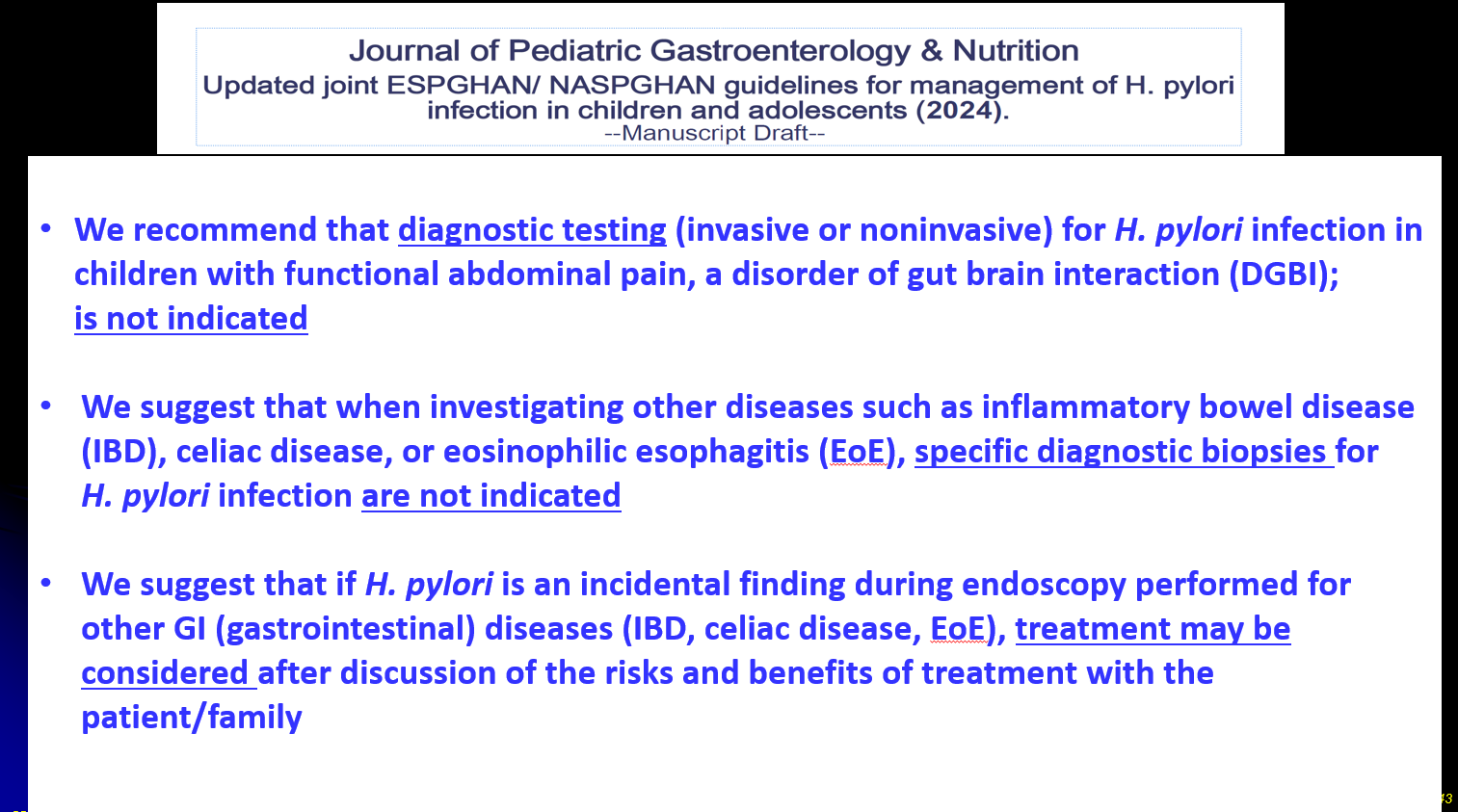
- Dr. Benjamin Gold: 2024 Pediatric H pylori Guidelines (Part One)
- Dr. Benjamin Gold: 2024 Pediatric H pylori Guidelines (Part 2)
- Excellent Review of H Pylori in Children Plus One on Healthy Aging
- Brief Updates: H pylori Resistance Rates, VEDOKIDS, Increasing Bariatric Surgery in Kids