TE and MRE did not have high correlation with liver biopsy in the detection of high-grade fibrosis
Fibrosis was identified in 90% of liver biopsies with bridging fibrosis in 15 (19%) and cirrhosis in 1 (1%)
AUROC curves of MRE and TE for detection of high-grade fibrosis were 0.817 and 0.750, respectively, and not significantly different.
The authors note that previous adults studies suggest that MRE is more accurate in the identification of liver fibrosis than TE (MRE detected ≥ F1 fibrosis with an AUROC of 0.82, while TE detected fibrosis with an AUROC of 0.67).20
My take: Trying to identify accurate non-invasive testing is crucial to help identify patients most in need of treatment and for limiting costs.
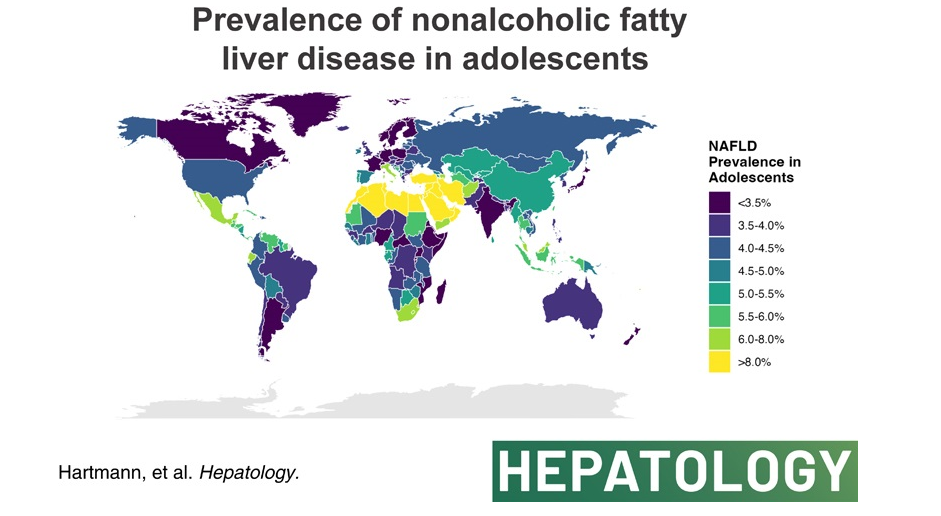
The authors analyzed data from the Global Burden of Disease Study 2019 to compare global, continental, and national prevalence rates of adolescent (15-19 yrs of age) NAFLD.
Key finding:
The global NAFLD prevalence in adolescents increased from 3.73% in 1990 to 4.71% in 2019 (a relative increase of 26.27%). NAFLD is now termed metabolic dysfunction-associated steatotic liver disease (MASLD).
High body mass index and not type 2 diabetes mellitus correlated with NAFLD prevalence in adolescents globally.
In the associated editorial (S Xanthakos, Hepatology78(4):p 1017-1019, October 2023, Rising tide of NAFLD in youth: A warning bell and call to action), some of the key points:
“The Global Burden of Disease (GBD) Study is the most comprehensive and long-standing effort to systematically and scientifically collate data on hundreds of diseases and injuries across the globe, including related clinical outcomes. Beginning in 1990, the GBD Study initially collected data on 106 conditions and 10 risk factors, across 5 age groups.1 Over time, the GBD Study has expanded through serial iterations to involve >9000 international researchers collecting data on 369 diseases and injuries across 204 countries and territories in the most recent 2019 report.1“
” From the GBD Study, we learned that NAFLD is the most rapidly rising cause of chronic liver disease in adolescents and adults,2 and the fastest-growing contributor to cirrhosis, liver cancer, and liver-related deaths globally.”
“The global prevalence of NAFLD in adolescents shows no sign of abating, rather has continued to increase steadily from 3.7% in 1990 to 4.7% in 2019.”
“As with all epidemiological research, the GBD study faces the primary limitation of relying on data sources that employ varying and less accurate measures of NAFLD prevalence (alanine aminotransferase and/or ultrasound primarily). However, the rigorous methodological approach employed by the GBD including frequent assessment of face validity, and the tremendous input of data sources (>80,000 in 2019) nonetheless results in the most comprehensive global data set available.”
My take (borrowed from editorial): Without intervention, “the increase in adolescent NAFLD certainly portends a future increase in NAFLD-related cirrhosis and liver-related deaths in young adults in the coming decades, and a likely escalation in cardiovascular and diabetes-related morbidity.
This article offers best practice advice -here are two of them:
#2: A Fibrosis 4 Index score <1.3 is associated with strong negative predictive value for advanced hepatic fibrosis and may be useful for exclusion of advanced hepatic fibrosis in patients with NAFLD.
#8 Patients with NAFLD and NITs (noninvasive tests) results suggestive of advanced fibrosis (F3) or cirrhosis (F4) should be considered for surveillance of liver complications (eg, hepatocellular carcinoma screening and variceal screening per Baveno criteria). Patients with NAFLD and NITs suggestive of advanced hepatic fibrosis (F3) or (F4), should be monitored with serial liver stiffness measurement; vibration controlled transient elastography; or magnetic resonance elastography, given its correlation with clinically significant portal hypertension and clinical decompensation.
In this study from U.S., patients (n=2523) were divided into three categories based on FIB-4 scores: (A) Fibrosis-4 (FIB-4) <1.3 and/or liver-stiffness measurement (LSM) measured by Fibroscan <8 kp, (B) FIB-4 1.31‒2.6 and/or LSM 8.1-12.5 kp, and (C) FIB-4 >2.6 and/or LSM >12.5 kp. However, those in class A with aspartate transaminase:alanine transaminase ratio >1 or platelets <150,000/mm3, or class B with aspartate transaminase:alanine transaminase ratio >1 or platelets <150,000/mm3 were upstaged by one class. The data were reviewed retrospectively from a prospective longitudinal cohort (TARGET-NASH)
Key findings: All adverse outcomes including liver and cardiovascular (see below) were correlated with FIB-4 staging.
Key findings: The prevalence of steatosis, severe steatosis, advanced fibrosis, and cirrhosis was 44.39%, 10.57%, 2.85%, and 0.87%, respectively in Chinese adults
Limitation: This data was derived from a health checkup cohort which could give different results than a random population sampling. Patients at health checkups may be more health conscious and/or be aware of underlying health concerns.
Prevalence of different grades of liver fibrosis in different age groups.
My take: Steatotic liver disease is a huge worldwide problem. The growing prevalence is going to result in extensive health issues.
—————
This year’s pumpkin 910/31/23):
It does not look like I will become a professional pumpkin artist anytime soon!
A total of 236 panelists from 56 countries participated in four online surveys and two hybrid meetings.
Key points:
Steatotic liver disease (SLD) was chosen as an overarching term to encompass the various “aetiologies” of steatosis.
The name chosen to replace NAFLD was metabolic dysfunction-associated steatotic liver disease (MASLD). There was consensus to change the definition to include the presence of at least one of five cardiometabolic risk factors (see 2nd figure).
The term steatohepatitis was felt to be an important pathophysiological concept that should be retained. Metabolic dysfunction-associated steatohepatitis (MASH) is the replacement term for NASH.
Those with no metabolic parameters and no known cause were deemed to have cryptogenic SLD.
A new category, outside pure MASLD, termed MetALD was selected to describe those with MASLD who consume greater amounts of alcohol per week (140 to 350 g/week and 210 to 420 g/week for females and males respectively).
AASLD News Digest: “MASLD, formerly known as NAFLD, is the most common chronic liver disease around the world, affecting more than 30% of global population. This was why it was vital that the global liver community coalesce around an affirmative, non-stigmatizing name and diagnosis. Ultimately, the global members of the Nomenclature Development Initiative were focused on ensuring the global community had better nomenclature that could be used around the world so that the research and funding could be better directed to save more people’s lives.”
My take: NAFLD is now MASLD –time to update patient handouts (hopefully someone at GIKids.org is on top of this). Aslo, if you have really bad disease, should it be called the ‘monster MASH’ ?
The authors included 10,040 participants from the Framingham Heart Study, the Coronary Artery Risk Development in Young Adults Study, and the Multi-ethnic Study of Atherosclerosis to assess the longitudinal association between liver fat (defined on CT) and incident cardiovascular disease (CVD).
Key finding:
Hepatic steatosis was associated with all-cause mortality after 12.7 years of mean follow-up when adjusting for baseline CVD risk factors, including body mass index (HR: 1.21, 1.04–1.40); however, the association between hepatic steatosis and incident CVD was not statistically significant after we accounted for body mass index in models considering baseline covariates or time-varying covariates. We observed no association between hepatic steatosis and CVD-related mortality or incident cancer.
My take: While CVD is the leading cause of mortality in patients with fatty liver disease, this study suggests that hepatic steatosis is a marker for this increased risk rather than an independent cause.
This lengthy article is loaded with data on trends and costs of liver transplantation in the U.S.
Key findings:
From 2016 to 2019, the estimated total number of LT-related hospitalizations in the US were 6685, 7075, 7260, and 7815 cases respectively.
There was a general increase in the total cost of LT-related hospitalizations over the years: $945.75, $1010.23, $1052.46, and $1143.84 in millions of dollars.
Editorial: A Kaplan et al.Liver Transplantation 2023; 29: 568-569. Open Access! Liver transplant at all costsKey points:
Mean costs per patient for transplant-related hospitalization were around $145,000.
“Lee and colleagues’ important study adds to the growing concern over rising costs for LT. However, LT is 1 of many fields that must utilize a scarce resource for the maximal benefit of society. Balancing costs with a life-saving procedure that is very expensive will continue to be a persistent challenge.”
My take: It is likely that the costs of liver transplantation are going to continue to rise unless we develop a shortage of suitable liver donors or a shortage of transplant personnel. Severe fatty liver disease and alcoholic liver disease continue to increase in frequency while hospital costs continue to soar. Reducing costs will rely on reversing the tide of these diseases.
Related blog posts:
Trends in Liver Diseases: Autoimmune Liver Diseases and Fatty Liver (2021). In 2019, among patients without HCC, NASH was the second leading indication for liver transplantation (28% of patients), after ALD (38% of patients). were chronic HCV infection (37%) and ALD (16%), whereas only 5% had NASH
This 38 page report has a ton of updated recommendations and useful advice –geared to adults with fatty liver disease. The last ~dozen pages are the 491 references.
Some of the useful points:
CVD and nonhepatic malignancies are the most common causes of mortality in patients with NAFLD without advanced fibrosis; death from liver disease predominates in patients with advanced fibrosis.
Initial lab evaluation in adults:
Statins are safe and recommended for CVD risk reduction in patients with NAFLD across the disease spectrum, including compensated cirrhosis.
Patients with NAFLD should be screened for the presence of T2DM. T2DM is the most impactful risk factor for the development of NAFLD, fibrosis progression, and HCC.108–111 Given the central pathogenic role that insulin resistance plays in the pathogenesis of both T2DM and NAFLD, it is not surprising that patients with T2DM have a higher prevalence of NAFLD (ranging from 30% to 75%)10,112,113 and a higher risk of developing NASH with fibrosis.93,114–117
Other important comorbidities: dyslipidemia, obstructive sleep apnea, cardiovascular disease, and chronic kidney disease
Lifestyle factors that can be beneficial:
Table 6 lists potential medications though there are no FDA approved treatments for fatty liver disease. Bariatric surgery is also a beneficial treatment option “in patients who meet criteria for metabolic weight loss surgery, as it effectively resolves NAFLD or NASH in the majority of patients without cirrhosis and reduces mortality from CVD and malignancy.”
Potentially useful medications include Vitamin E, Pioglitazone, Liraglutide, Semaglutide, Tirzepatide and SGLT-2i. “Semaglutide can be considered for its approved indications (T2DM/obesity) in patients with NASH, as it confers a cardiovascular benefit and improves NASH. Pioglitazone improves NASH and can be considered for patients with NASH in the context of patients with T2DM . Available data on semaglutide, pioglitazone, and vitamin E do not demonstrate an antifibrotic benefit, and none has been carefully studied in patients with cirrhosis.”
Treatments NOT Recommended: “Metformin, ursodeoxycholic acid, dipeptidyl peptidase-4, statins, and silymarin are well studied in NASH and should not be used as a treatment for NASH as they do not offer a meaningful histological benefit.”
This study, in agreement with prior studies of individuals with chronic liver disease, showed that statin use is associated with a lower risk of hepatocellular carcinoma in NAFLD as well, with a Hazard Ratio of 0.47 in a database with 272,431 adults with NAFLD. The authors note the concern about hepatotoxicity from statins; however, “severe liver injury from statins is fairly low. Indeed, the incidence of lovastatin-associated fulminant liver failure is about 2 in a million users.”
Porto‐sinusoidal vascular disorder (PSVD; also previously described as idiopathic noncirrhotic portal hypertension [NCPH]…”is a group of liver vascular diseases featuring lesions encompassing the portal venules and sinusoids unaccompanied by cirrhosis, irrespective of the presence/absence of portal hypertension. It can occur secondary to coagulation disorders or insult by toxic agents. However, the cause of PSVD remains unknown in most cases.”
Key findings:
In a group of 4 patients, a novel heterozygous mutation in the FCHSD1 gene was identified but not in 2 familial controls.
When this variant was introduced in mice using CRISPR, ” Nine out of the 15 mice carrying the human FCHSD1R183Wvariant mimicked the phenotype of human PSVD, including splenomegaly and enlarged portal vein.”
Aberrant FCHSD1 structure and function led to mTOR pathway overactivation
“Consumptive hypothyroidism (CH) is a rare form of hypothyroidism due to thyroid hormone inactivating enzyme type 3 (Deiodinase) overexpressed by hepatic/hepatic and cutaneous hemangiomas, and occasionally by some other extrahepatic visceral hemangiomas…Pediatric hepatologists should recognize the importance of periodical assessments of thyroid function in patients with hepatic hemangiomas”
“MRI of the abdomen in one of our patients (patient 1), before (A) and after (B) 19 months of treatment with propranolol/10 months of treatment with levothyroxine. The T2-weighted axial MRI images shows the regression of a diffuse infantile hepatichemangioma with innumerable T2 hyperintense masses throughout the liver with central hypointense central regions.”
In this prospective study with 204 children with severe obesity, intensive lifestyle changes were implemented. Key findings:
After 6 months, the median body weight loss was 16.0% in the 167 patients evaluated
Fibrosis improved in 75.0% (P < .001) (33% had F2 or higher fibrosis at baseline per elastography)
Fasting serum alanine aminotransferase and homeostasis model assessment of insulin resistance decreased significantly over the 1-year period (P < .001)
In this retrospective study with 784 children, Key findings:
Of these children, 168 (31%) had a BMIz (BMI z-score) change of >−.25 from baseline over a median of 367 days (IQR, 201-678 days). Thus, ~1/3rd of children achieved a drop in BMIz with lifestyle advice
A BMIz reduction of >.25 was associated with significant improvements in serum aminotransferase levels.
My take: These pediatric studies replicate similar findings from adult studies showing that modest reductions in weight are associated with improvement in NAFLD. However, most patients are not successful with lifestyle advice which underscores the need for pharmacotherapy.
In this single-center retrospective study (2017–2020), the authors reviewed the extent of testing and yield in children with suspected NAFLD. Criteria:
BMI >85th percentile
Persistently (>3 months) elevated ALT more than twice the ULN for age
Radiographic (ultrasound, computed tomography, and MRI) features of hepatic steatosis.
Key findings:
Eleven (11.6%) patients were ultimately diagnosed with a condition resulting from their abnormal bloodwork: infectious hepatitis (3, 9.8%), thyroid disease (2, 3.4%), celiac disease (4, 7.7%), AIH (1, 1.7%; diagnosis based on liver biopsy), and A1AT deficiency (1, 2.0%). It is likely that the yield would have been higher if all patients had more extensive testing
Only 9.5% of patients had comprehensive, additional testing performed per the 2017 North American Society of Pediatric Gastroenterology, Hepatology and Nutrition guidelines: infectious hepatitis serologies (Hepatitis A virus IgM, Hepatitis B surface antigen, anti–Hepatitis C virus), thyroid studies (thyroid-stimulating hormone [TSH]), ceruloplasmin, A1AT, liver autoantibodies (antinuclear antibody; anti-smooth muscle antibody; liver kidney microsome type 1 antibody), tissue transglutaminase IgA (TTG-IgA), total IgA, total IgG, and LAL blood spot
The costs of performing the recommended testing was estimated as $397.30 Canadian dollars
My take: In those with persistently elevated liver enzymes, additional blood tests are important to evaluate for chronic liver diseases, even in those suspected of NAFLD.
When investigating elevated liver enzymes in teenagers, serology for autoimmune hepatitis (AIH) is frequently obtained. In the face of overweight/obesity, the majority will have nonalcoholic fatty liver disease (NAFL). How many with elevated autoantibodies actually have autoimmune liver disease (ALD)? Some information regarding this issue is available in the article by Khayat et al.
Methods: A retrospective, cross-sectional study of 181 children with a biopsy-proven diagnosis of NAFL, NASH, autoimmune hepatitis (AIH), or primary sclerosing cholangitis (PSC) and a body mass index (BMI) >85th percentile treated between 2007 and 2016.
Key findings:
Antinuclear antibody (ANA), anti-actin antibody, and anti–liver kidney microsomal (LKM) antibody were positive in 16.1%, 13.8%, and 0%, respectively, of the patients with NAFL and in 32.8%, 15.5%, and 0%, respectively, of those with NASH
Total immunoglobulin G (IgG) was elevated in 27.3% of the patients with NAFL and in 47.7% of those with NASH, but in 100% of those with ALD. A normal IgG level was the “strongest negative predictor of ALD, followed by a negative ANA and actin.”
The positive predictive value of LKM was 100% for ALD but only 29% for ANA and 46% for anti-actin antibody. ANA positivity in this cohort was associated with more insulin resistance
ALD was present in 29/181 (16%). 12 (6.6%) with isolated ALD (AIH, PSC, or overlap), and 17 (9.4%) with combined ALD and NAFLD
BMI >98% “appears to be an important breakpoint above which ALD is less likely” even when IgG is high with a positive ANA
Limitations: Retrospective study, not every patient had all of the ALD serology tests
My take: Even heavy kids may have autoimmune liver disease. In those with abnormal serology, about 1 in 6 will have ALD, either in combination with NAFL or as the sole etiology of abnormal LFTs.