Background: “Given the invasiveness of liver biopsy, the development of accurate non-invasive biomarkers of MASLD severity remains an area of active investigation… clinical practice has been shifting towards the use of point-of-care vibration controlled transient elastography (VCTE), based on extensive cross-sectional and longitudinal validation data in adults.11 However, despite increasing clinical use of VCTE to determine MASLD presence and severity in children, this technique lacks well-validated cut-points in this age range and, importantly, there are no data evaluating the implications of longitudinal changes.12–15…While a high (>12 kPa) LSM is concerning for progression to advanced fibrosis in adults,11 the optimal cutoff for defining an elevated LSM in pediatric MASLD has yet to be established.16, 17“
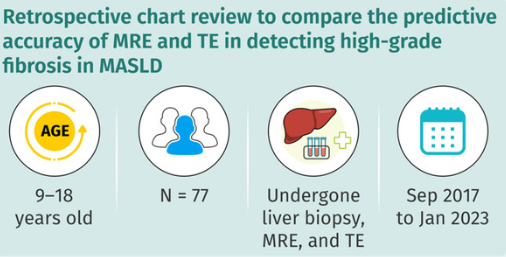
Methods: This was a longitudinal retrospective study of youth (n=149, mean age 14 yrs) with MASLD who underwent ≥2 VCTE studies.
Key findings:
- Controlled attenuation parameter (CAP) and liver stiffness measurements (LSMs) showed marked intraindividual variability.
- Changes in CAP and LSM did not predict categorical outcomes of ALT and GGT reduction, however were significantly positively associated with continuous ALT and GGT outcomes, independent of BMI percentile.
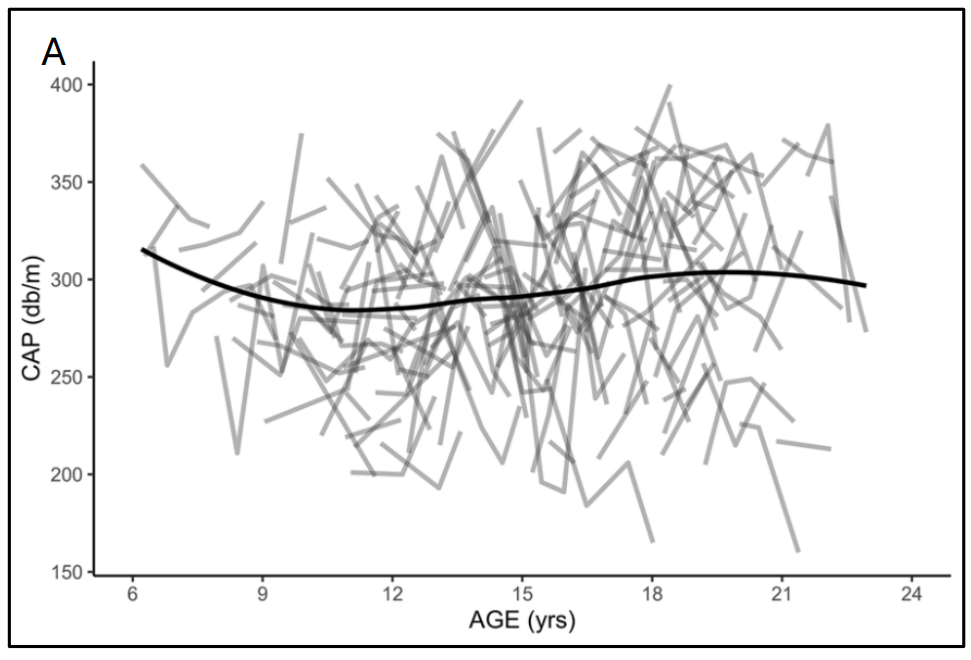
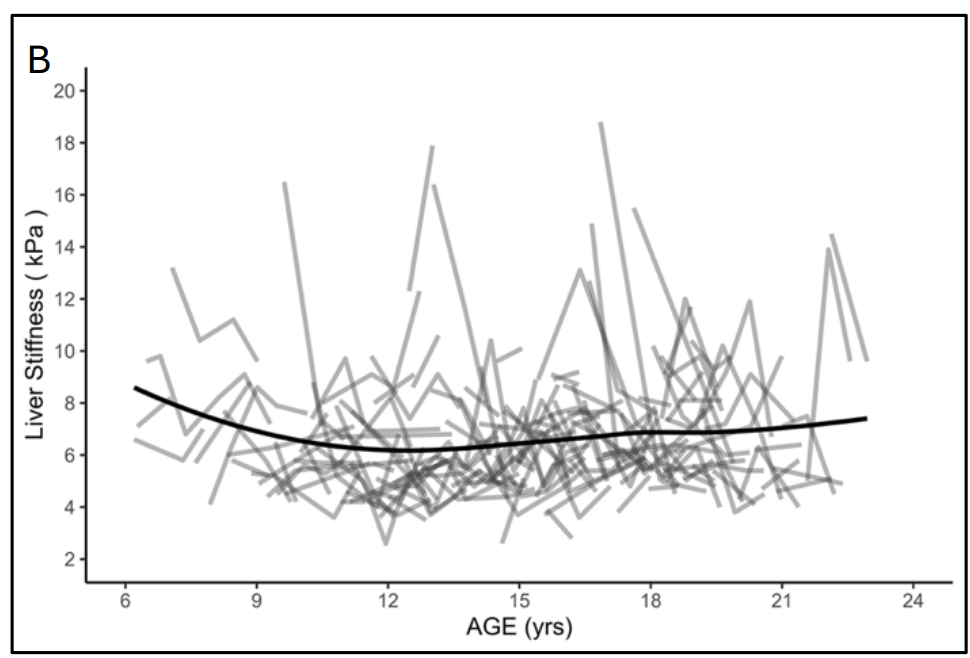
My take (borrowed in part from the authors): “Given the substantial intra-individual variation and the current lack of validated definitions for clinically significant change in VCTE measures (CAP and LSM) in children with MASLD, serial VCTE measurements in individual pediatric patients should be interpreted with caution and not relied upon in isolation for clinical decision-making.”
While transient elastography is not reliable in pediatric MASLD, a related article suggests that it is helpful for pediatric autoimmune hepatitis: W Janczyk et al. J Pediatr Gastroenterol Nutr. 2026;82:1349–1356. Transient elastography for accurate staging of liverfibrosis and predicting complications in children withautoimmune hepatitis
Related blog posts: