Although primary sclerosing cholangitis (PSC) is an infrequent liver problem in pediatrics, it remains important. PSC accounts for 2-3% of pediatric liver transplant cases. A recent report updates some of the challenges for pediatric hepatologists (Shneider BL. Liver Transplantation 2012: 18: 277-81).
First the article examines some of the salient differences between children and adults. The approach in adults may not apply well to children. Some inherited diseases and immunologic defects may produce a similar clinical picture. Specific differences include the following:
- Defects in the adenosine triphosphate-binding cassette B4 (ABCB4 gene) (multidrug resistance protein 3) may cause a number of small-duct PSC in children
- Cystic fibrosis can have a similar appearance
- Overlap syndrome with autoimmune hepatitis is more common in children
- Children with PSC often have higher alanine aminotransferase enzyme values than adults
- Cholangiocarcinoma is rare in childhood, with 17 being the youngest reported case
Diagnosis usually requires, in addition to blood tests, cholangiography (eg MRCP), liver biopsy or both. ERCP may not be needed depending on MRCP results.
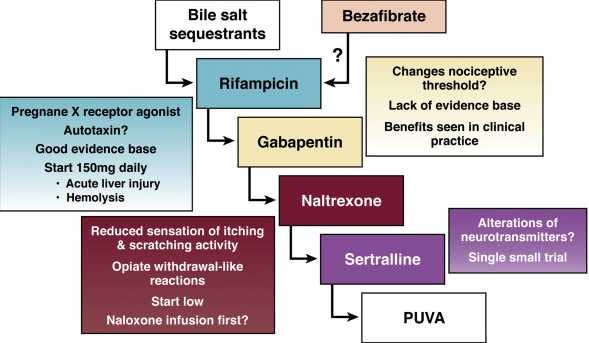
Management: Pruritus may be managed with ursodeoxycholic acid (UDCA), bile acid binding resins, and rifampin. Bone disease needs to be monitored along with fat soluble vitamin status.
- While pruritus may improve with UDCA, high-dose UDCA (28-30mg/kg/day) has been associated with increased likelihood of negative endpoints. It is not clear whether there may be detrimental effects at lower doses.
- What about immunosuppression? This (corticosteroids/thiopurines) is accepted in cases with AIH overlap. Of course, what constitutes overlap is not certain. So, in many cases, a trial of corticosteroids is considered.
- Antibiotics? Oral vancomycin has been tried in a small number with preliminary success.
As noted above, liver transplantation is a needed treatment in some cases. One concern with this approach has been recurrent PSC in about 10% at an average of 18 months after liver transplantation.
Additional references:
- -Am J Gastro 2011; 106: 1638. Use of high dose Urso increases risk of colonic neoplasia. n=150.
- -Hepatology 2011; 54: 1842. Guidelines on surveillance for PSC. IF IBD yearly scope. **Yearly U/S + CA 19-9 or yearly MRI.
- -Liver Transplantation 201; 17: 925-933. n=79 pediatric pts. 49% w IBD prior to OLT (46% w UC, 3%) & 9.8% developed IBD p OLT. 1 & 5yr survival for OLT 99% & 87%. Recurrence in 9.8%.
- -Clin Gastro & Hepatology 2011; 9: 434. 37% of PSC pts with CA 19-9 >129U/mL do NOT have cholangiocarcinoma. n=7.
- -Hepatology 2010; 51: 660-678. update on dx/mgt.
- -Gastroenterology 2010; 138: 1102. genome associations with PSC.
- -Hepatology 2009; 50: 808, 671 (ed). Use of urso ~30/kg associated w WORSE outcome @5yrs. n=76 (& 74 controls)
- -Clin Gastro & Hep 2009; 7:239. n=47 children w PSC. 59% w IBD, 25% w overlap syndrome
- -JPGN 2008; 47: 61. Use of oral vancomycin, 50mg/kg/day in patients with PSC/IBD was effective. n=14.
- -Liver Tx 2008; 14: 735. Review. 5 yr OLT survival 85% ReTx rate higher (9.6% vs 4.9%).
- -Hepatology 2008; 47: 9494-57. Asymptomatic PSC common in AIH –might be higher than 10%.
- -Gastroenterology 2008; 134: 975. Natural hx/o small duct PSC in 83 pts (compared to controls). Not likely increase in cholangiocarcinoma unless also large duct involvement.
- -Gastroenterology 2008; 134: 706. IAC is similar; IAC=IGG4 Associated Cholangitis
- -Hepatology 2008; 47: 949. 8/79 w AIH also had PSC.
- -J Pediatr 2007; 151: 255, 230. association of CFTR mutations in PSC (26%); also present in disease control group with IBD (43%).
- -Clin Gastro & Hep 2007; 5: 32. Review vis-a-vis possible cholangiocarcinoma.
- -Hepatology 2006; 44: 1063. Review along w secondary causes.
- -Liver Transplantation 2006; 12: 1813. Recurrence post Tx 22% AIH, 18% PBC, 11% PSC. (Review of 43 studies).
- -Gastroenterology 2005; 129:1464. High-dose actigall ineffective in 5 yr randomized controlled study.
- -Gastroenterology 2003; 125: 1364. Incidence of PSC.
- -JPGN 2003; 37: 345 (57A). Use of vanco 50/kg/day x 4-6weeks in PSC, n=10, (56A) some pts c normal cholangiograms.
- -Gastroenterology 2003; 124: 889. Urso prevents colon ca.
- -Am J Gastro 2001; 96: 1558-62. High dose UDCA, 25-30/kg/day may help long-term outlook
- -JPGN 2001; 33:296. PSC-IBD.
- -NEJM 2002; 346: 271-277. case c Crohn’s. PSC assoc c UC, celiac dz, pancreatic insufficiency.
- -Ann Intern Med 2001; 134: 89-95. Urso decreases colonic neoplasia in pts c UC & PSC.
-NEJM 1997; 336: 691. Ursodeoxycolic acid & PSC.
- -Gregorio et al. Autoimmune hepatitis/sclerosing cholangitis overlap syndrome in childhood: a 16-year prospective study. Hepatology 2001;33:544-553
NASPGHAN 2010 Pointers:
I. -“STOPSC criteria”: 2 of 3 diagnostic criteria needed:
1) elev GGT or alk phos
2) intra and/or extrahepatic bile duct irregularities on cholangiography (i.e. PTC, MRCP, ERCP) c/w PSC
3) liver biopsy abnormalities c/w chronic biliary injury
AND no evidence of a secondary cause of sclerosing cholangitis
II. SUMMARY OF KEY CLINICAL FEATURES:
- -Sclerosing cholangitis is associated with IBD, autoimmune and connective tissue disorders, abnormalities of immune function (i.e. immunodeficiencies, GvHD), infiltrative disorders (i.e. Langerhans cell histiocytosis, lymphoma).
- -PSC may sometimes affect only small intrahepatic bile duct (“small duct PSC”), which may have a better outcome based on adult studies
- -PSC may have overlapping features of AIH (“autoimmune sclerosing cholangitis”)
- -IgG4 –associated cholangitis: patients appear to have PSC with elev IgG4. They seem to respond very well to steroid therapy in adult studies
- -No therapy of proven benefit for PSC (ursodiol, antibiotics), some case series have suggested antibiotics may help PSC
- -5 times higher rate of Colorectal Ca when UC pt has PSC. Consider yearly endoscopy