W Gao et al. Gastroenterol 2026; 170: 1473-1483. Open Access! Vonoprazan-Tetracycline Dual Regimen as Rescue Therapy for Helicobacter pylori Infection: Randomized Controlled Trial
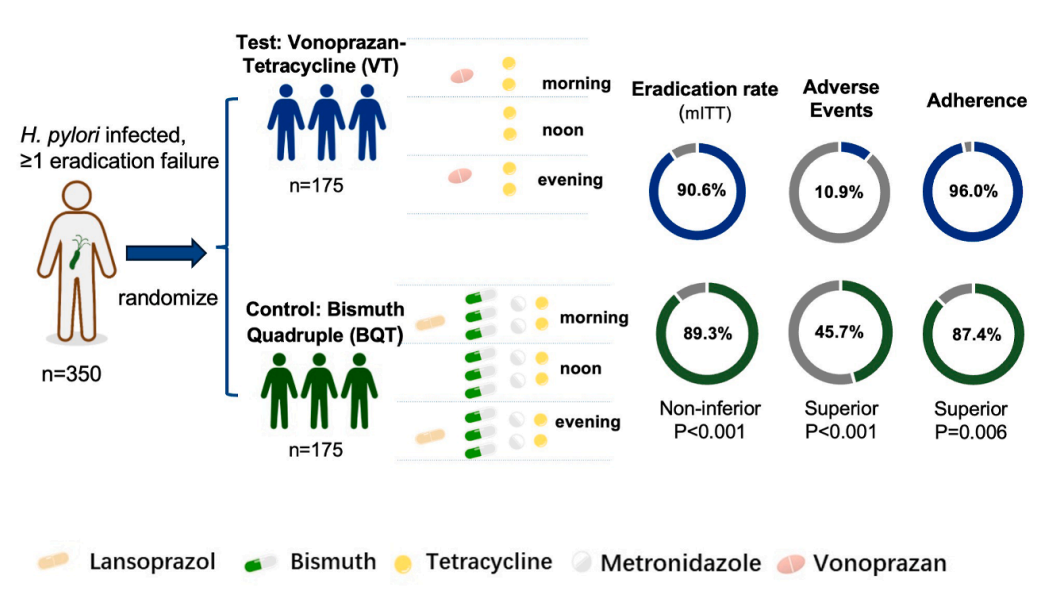
Methods: In this prospective, open-label, randomized controlled trial(n=350), H pylori–positive adults with at least 1 prior eradication failure were allocated 1:1 to VT dual therapy (vonoprazan [20 mg, twice a day] and tetracycline [500 mg, 3 times a day]), or bismuth quadruple therapy (BQT; lansoprazole [30 mg, twice a day], colloidal bismuth [150 mg, 3 times a day], tetracycline [500 mg, 3 times a day], and metronidazole [400 mg, 3 times a day]) for 14 days.
Key findings:
Discussion:
- “Potent acid suppression broadens the applicability of dual therapy, allowing a single sensitive antibiotic to achieve reliable eradication when gastric pH is maintained at ≥6 with potassium-competitive acid blockers.13–15“
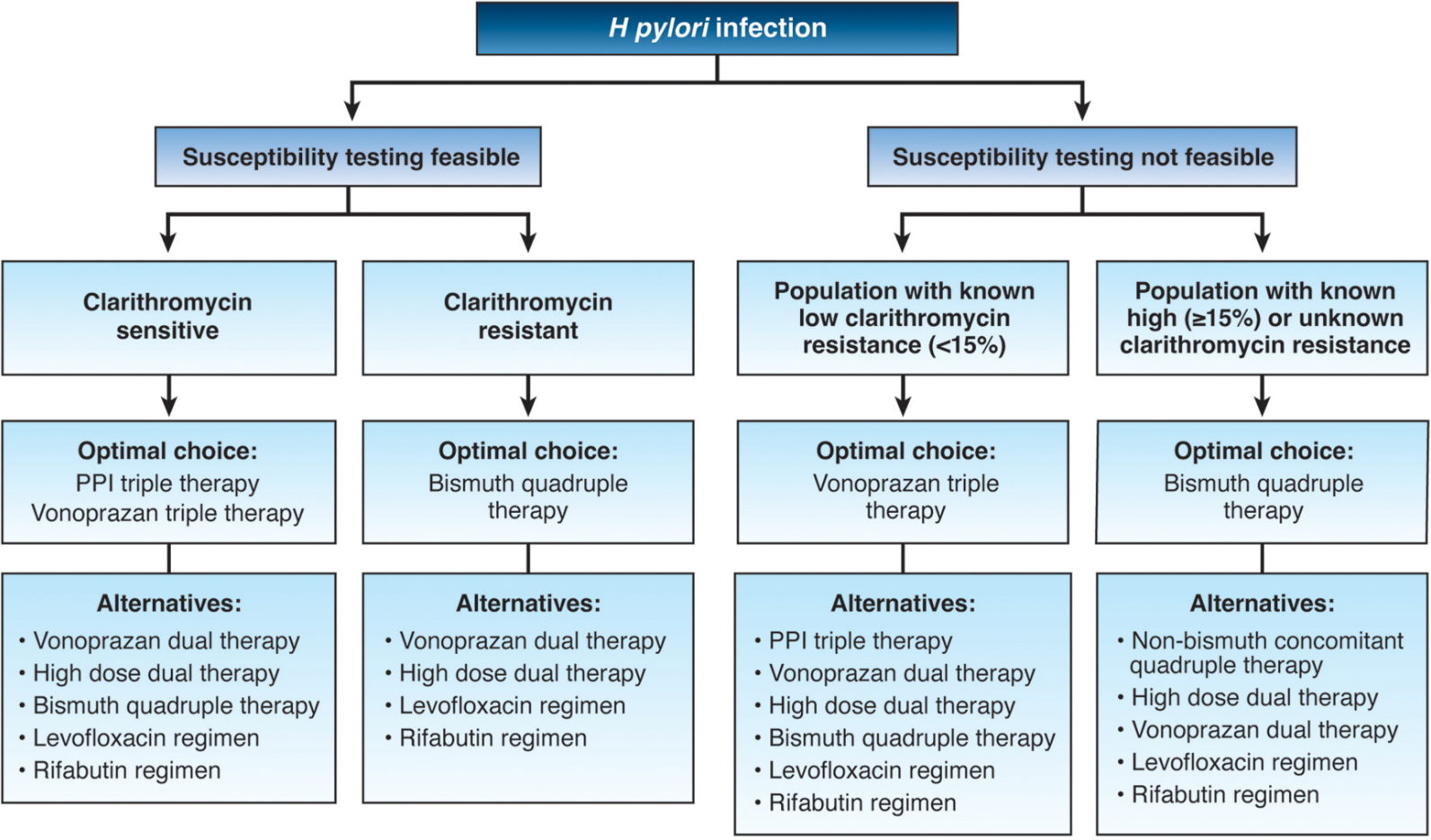
- “Antibiotic resistance is a major obstacle to the successful eradication of H pylori, particularly in rescue treatment. Surveillance data from the Asia-Pacific region (1990–2022) have shown persistently high resistance rates to metronidazole (52%), levofloxacin (26%), and clarithromycin (22%), whereas resistance to tetracycline and amoxicillin has remained low, both at ∼4%.17“
- “Although high-dose amoxicillin dual therapy has been well studied and incorporated into guidelines for first-line treatment, the clinical potential of tetracycline-based regimens deserves similar attention.19,20“
Limitations: This was an open-label trial from a single center and did not include antibiotic resistance testing, which may limit generalizability to other regions or clinical settings.
My take (borrowed from authors): Vonoprazan combined with tetracycline is a simplified, penicillin-free rescue regimen, and may offer a practical option for the rescue treatment of H pylori infection. Its eradication rate was comparable to that of traditional tetracycline-metronidazole–based bismuth quadruple therapy, and was associated with fewer adverse events and better adherence.
Related blog posts:
- Understanding FDA Approval of Vonoprazan-Based Therapies for Helicobacter Pylori
- “Evidence-Practice Gap” and How It Applies to H pylori Treatment
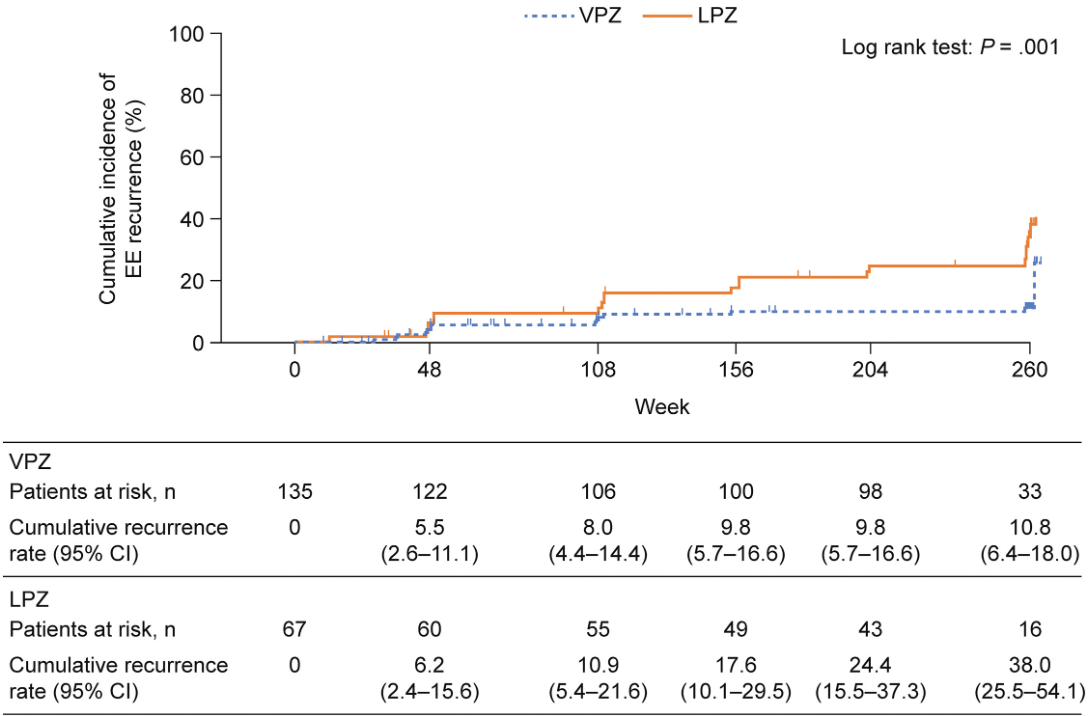
- VISION 5-Year Study Results: Safety of Vonoprazan in Erosive Esophagitis
- Practice Advice for Potassium-Competitive Acid Blockers (2024)
- Dr. Benjamin Gold: 2024 Pediatric H pylori Guidelines (Part One)
- Dr. Benjamin Gold: 2024 Pediatric H pylori Guidelines (Part 2)
- QI Project: Increasing H Pylori Eradication
- 5 Rights and H pylori Treatment
- Give the Right Dose (for H pylori) -It Works Better!
- Helicobacter Pylori Stool Susceptibility in Children –How Good Is It?
- Synergistic Dangers: Helicobacter Pylori and Cancer Genes
- AGA: Best Practice Advice for Refractory H pylori
- Treating Helicobacter Pylori Lowers The Risk of Gastric Cancer