
Author Archives: gutsandgrowth
NY Times: “Millions Take Gabapentin for Pain. But There’s Scant Evidence It Works.”
NY Times: “Millions Take Gabapentin for Pain. But There’s Scant Evidence It Works.”
Thanks to Stan Cohen for pointing out this reference.
An excerpt:
The drug was initially approved 25 years ago to treat seizure disorders, but it is now commonly prescribed off-label to treat all kinds of pain, acute and chronic…
Two doctors recently reviewed published evidence for the benefits and risks of off-label use of gabapentin (originally sold under the trade name Neurontin) and its brand-name cousin Lyrica (pregabalin) for treating all kinds of pain…
Gabapentin and Lyrica, both sold by Pfizer, have been approved by the Food and Drug Administration to treat only four debilitating pain problems: postherpetic neuralgia, diabetic neuropathy, fibromyalgia and spinal cord injury. Even for these approved uses, the evidence for relief offered by the drugs is hardly dramatic…
In many well-controlled studies they found there was less than a one-point difference on the 10-point pain scale between patients taking the drug versus a placebo, a difference often clinically meaningless….
the number of people taking gabapentinoids more than tripled from 2002 to 2015…
Related blog post: Brave New World: Psychotropic Manipulation and Pediatric Functional GI Disorders
Near Cathedral of Barcelona
Self-Service Health Care??
A provocative commentary (DA Asch et al. NEJM 2019; 380: 1891-3) notes that the current approach to improving health care costs needs to be reconsidered.
“The physician-patient encounter is health care’s choke point.” Instead of pushing for more primary care visits, the authors recommend greater use of automation. Examples in other industries have included:
- TurboTax -helped reduce need for tax preparer’s
- Automated tellers at banks -reduce costs at banks
- Self-checkout at grocery stores -reduce costs at grocery stores
- Websites to directly arrange travel rather than travel agents
Much of medical care can be algorithmic, including hypertension (which affects one-third of U.S. adults), hyperlipidemia, anticoagulation, diabetes, and “might be far more efficiently managed by a bot.”
“An efficient industry wouldn’t lead with primary care, but would reserve it for cases for which lower levels of support haven’t been enough.”
The authors note that efforts to promote this will require removal of state-based regulation. “There is not legitimate interest that benefits from making it hard for a patient in Kansas to get automated care with third-level support from a physician in Ohio.”
My take: The authors are right in their assertion: “Transformative change in any industry requires breakthroughs in productivity.” Some of these changes are likely to be implemented given the cost escalations facing health care.

Magic Fountain, Barcelona
“Physician-Patient Relationship is Not Necessary to Sue Docs for Malpractice”
A recent ruling from the Minnesota Supreme Court:
Thanks to Jeffrey Blumenthal for pointing out this reference. An excerpt:
The Minnesota Supreme Court issued a ruling on April 17 in the case of Warren v. Dinter holding that the existence of a physician-patient relationship is not a prerequisite for a medical malpractice action. Rather, a person may sue a physician for malpractice – even if that person was not a patient of the physician – if the harm suffered by the person was a “reasonably foreseeable consequence” of the physician’s actions….
The Warren v. Dinter case arises out of the care provided to a woman (Susan Warren), who complained of abdominal pain, fever, chills, and other symptoms to a nurse practitioner at Essentia Health Clinic in Hibbing. After testing showed that Warren had an elevated white blood cell count, the nurse practitioner suspected infection and sought hospitalization for her at Fairview Range Medical Center. The nurse practitioner’s call was randomly assigned to a hospitalist at Fairview to discuss admission.
After a brief conversation, during which the physician was unable to view the patient’s medical record, …the physician did not recommend hospitalization during the conversation and the nurse practitioner did not seek hospitalization for the patient following the conversation. The patient subsequently died from sepsis caused by an untreated staph infection. Warren’s family sued both the nurse practitioner and the physician for medical malpractice…
Before its ruling April 17, Minnesota law has generally required the existence of a physician-patient relationship to sustain a malpractice action against a physician. The Court’s decision to rely on a broader legal theory of “foreseeability” represents a troubling change that puts Minnesota in the minority of states that do not require the existence of a physician-patient relationship for a malpractice action.
My take: While “foreseeability” was used as a determinant in this case, observers may foresee that the court’s ruling could erode informal advice (aka. curbside consults) that generally improves patient outcomes. If physicians’ liability is significant, many may choose to not offer advice on patients that they have not fully evaluated.

Barcelona Esplanade/Adjacent to beach
Image Only: Total Colonic Aganglionosis
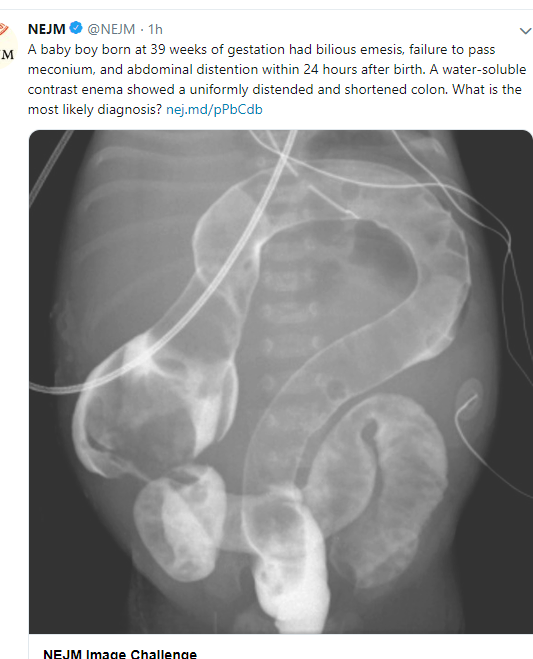
Hirschsprung’s disease with total colonic aganglionosis
Related blog posts:
Annual Costs: Generics vs. Brand-Name Medications
MDEdge: Cost gap widens between brand-name, generic drugs
An excerpt:
- The average cost of a brand-name drug was 18.6 times higher than its generic equivalent in 2017, and the size of that gap has more than tripled since 2013, according to a report from the AARP Public Policy Institute…
- In 2017, the average retail cost of 260 generic drugs widely used by older adults for chronic conditions was $365 for a year of therapy, compared with $6,798 for brand-name drugs. In 2013, that same year of therapy with an average brand-name drug ($4,308) was only 5.7 times more expensive than the generic ($751)…
- “Generics account for nearly 9 out of every 10 prescriptions filled in the U.S. but represent less than a quarter of the country’s drug spending,” Debra Whitman, executive vice president and chief public policy officer at AARP
My take (borrowed in part from Debra Whitman):
- “These results highlight the importance of eliminating anticompetitive behavior by brand-name drug companies so that we get more lower-priced generic drugs on the market”
- This data shows the alarming increase in cost of brand-name medications.
Related blog posts:
- Another Shady Pharmaceutical Business Practice: Citizen’s Pathway to Delay Competition | gutsandgrowth
- “This Is A Stick Up — Your Money or Your Life” | gutsandgrowth
- Exorbitant Medicine Costs -Even with Long-established Generics
- Turning Liquid into Gold: A Pharmaceutical Rumpelstiltskin Story | gutsandgrowth
- Orphan Drugs –Very Profitable | gutsandgrowth
- Public Shaming is Not an Effective Drug Pricing Policy | gutsandgrowth
- Drug Waste Costing Billions. Who benefits? Pharmaceutical Companies | gutsandgrowth
- Tackling High Drug Costs -Lessons from Australia and Brazil
- 5000% Increase for Well-Established Drug
- Drug Waste Costing Billions. Who benefits? Pharmaceutical Companies
- How to Undermine Value Care: Lessons from Pharmaceuticals
- The Solution to Drug Prices” | gutsandgrowth
- Cornering the Generic Markup | gutsandgrowth
- Upside Down Incentives in Pharmaceutical Development -Profit …
- “New Math on Drug Cost-Effectiveness”

Image Only: Increased Lawyer Reports of Kidney Disease Related to PPIs
Image
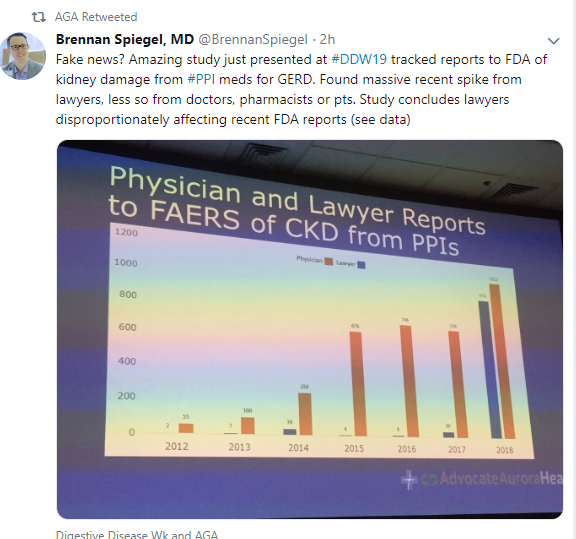
Image Only: Liver Involvement in Autosomal Dominant Polycystic Kidney Disease
Image

Capsaicin for Cannaboid Hyperemesis Syndrome
Capsaicin is the stuff in chili peppers that makes your mouth feel hot. But it also has some medical purposes. It’s a key ingredient in creams and patches that has been used for pain relief (e.g. joint, muscle, headaches).
From our recent hospital PNT meeting –information on using Capsaicin for Cannaboid Hyperemesis Syndrome (CHS).
What is cannabinoid hyperemesis syndrome (CHS)?
- Clinical syndrome in which marijuana users develop nausea, cyclic vomiting, and abdominal pain that improves with a hot water bath or cannabis cessation
- Often refractory to standard treatment for nausea/vomiting
- No laboratory or diagnostic tests for CHS
Capsaicin Mechanism for CHS
- Transient receptor potential vanilloid subtype 1 (TRPV1) receptor is expressed in the brain, along enteric and vagal nerves, and on cutaneous receptors in the skin
- Chronic cannabis use results in inactivation of TRPV1 receptor leading to nausea & emesis
- Nociceptive heat, such as topical capsaicin, acts as a TRPV1 agonist restoring gastric motility
- Activation of TRPV1 receptor results in potent anti-emetic effects
- Capsaicin exposure results in subsequent desensitization of the sensory axons and inhibition of pain transmission initiation.
Topical Capsaicin
- Product: Capsaicin cream 0.025% (Generic)
- Dosing: Apply thin film to affected area not more than 3 to 4 times/day
- Benefits:
- Less adverse effects than unconventional antiemetics (e.g., haloperidol)
- Cost-effective
- Adverse effects: “burning sensation” on skin
- Average wholesale price: $10 per 60 gram tube
Supporting literature
- Graham J, et al.
- Case series in which capsaicin was successfully used to treat CHS in two pediatric patients presenting to the emergency department (ED).
- In a 16 yo & 20 yo, each with two ED visits, on the 2nd visit: due to history of cannabis use, CHS became working diagnosis, patients agreed to try capsaicin cream (0.025%, 1 mm-thick coating) applied to the abdomen. Thirty minutes after capsaicin application, patients pain decreased to a 3 out of 10 and her nausea resolved
References:
- Moon AM, Buckley SA, Mark NM. Successful treatment of cannabinoid hyperemesis syndrome with topical capsaicin. ACG Case Rep J. 2018 Jan 3;5:e3.
- Graham J, Barberio M, Wang GS. Capsaicin cream for treatment of cannabinoid hyperemesis syndrome in adolescents: A case series. 2017 Dec;140(6): e20163795.
My take: Capsaicin use for CHS is supported by case reports.
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications/diets (along with potential adverse effects) should be confirmed by prescribing physician/nutritionist. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.

From Barcelona chocolate museum –everything is chocolate
Aprepitant for CVS
Last year at NASPGHAN meeting (NASPGHAN Highlights and Tweets), there was data presented on aprepitant for cyclic vomiting syndrome (CVS). This came up at a recent hospital PNT meeting as well.
- Aprepitant (Emend) is an anti-emetic that works by blocking the NK1 receptor.
- It has FDA approval for prevention of nausea and vomiting in moderate and highly emetogenic chemotherapy (adults and pediatrics) and prevention of post-operative nausea and vomiting (adult only).
Supporting Data for use of Aprepitant
An abstract published in 2006 reported on the use of aprepitant in 11 children (3-16 years)2. Patients were refractory to/had poor response to pizotifen (not available in US – serotonin and histamine antagonist), propranol, and ondansetron. Aprepitant was dosed at 80 mg/m2 up to twice weekly in combination with ondansetron. Nine out of 11 patients had reduction in cycle frequency, duration of vomiting episodes and intensity of vomiting. Three patients achieved complete cycle abolishment.
Cristoferi et al retrospectively reviewed 41 patients (age range 4-16.5 years, median 8 years) treated acutely or prophylactically with aprepitant.3 The primary outcome was decrease in frequency and intensity of CVS episodes. The follow up period was 18-60 months. The majority of patients failed cyproheptadine/pizotiphen, ondansetron, and amitriptyline as prophylactic medications.
Dosing regimens utilized in Cristoferi paper:
Prophylactic regimen (oral):
- < 40 kg, 40 mg twice/week = $220/week (average wholesale price)
- >40 kg to < 60 kg, 80 mg twice/week = $408/week
- > 60 kg, 125 mg twice/week = $612/week
Acute regimen (oral):
- >20 kg, 125 mg x 1 followed by 80 mg on day 2 and day 3 = $714
- 15-<20 kg, 80 mg x 3 days = $612
- < 15 kg, 80 mg x 1 followed by 40 mg on day 2 and day 3 = $424
Response rates:
- With the prophylactic regimen, the authors reported a complete response in 3/16 (19%) and a partial response 10/16 (62%) [partial response was considered if there was ≥50% decrease in CVS episode frequency and intensity].
- With the acute regimen, the authors reported 19/25 (76%) with a complete response and 3/25 (12%) with a partial response.
My take: Aprepitant appears promising as an agent for children who fail first-line therapies like periactin, tricyclic antidepressants, and ondansetron.
References
- Bhandari S and Venkatesan T. Novel treatments for cyclic vomiting syndrome: beyond ondansetron and amitriptyline. Curr Treat Options Gastro 2016;14:495-506.
- Russell RK, et al. NK1 receptor antagonism ameliorates nausea and emesis in typical and atypical variants of treatment refractory cyclical vomiting syndrome. J Pediatr Gastroenterol Nutr 2006;42:E13.
- Cristoferi F, et al. Efficacy of the neurokin-1 receptor antagonist aprepitant in children with cyclical vomiting syndrome. Aliment Pharmacol Ther 2014;40:309-17.
Related blog posts:
- Diet of drugs for CVS
- Costs/Yield of Diagnosing Cyclic Vomiting Syndrome
- Getting in the Shower for Emetic Symptoms
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications/diets (along with potential adverse effects) should be confirmed by prescribing physician/nutritionist. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.

