About gutsandgrowth
I am a pediatric gastroenterologist at GI Care for Kids (previously called CCDHC) in Atlanta, Georgia. The goal of my blog is to share some of my reading in my field more broadly. In addition, I wanted to provide my voice to a wide range of topics that often have inaccurate or incomplete information.
Before starting this blog in 2011, I would tear out articles from journals and/or keep notes in a palm pilot. This blog helps provide an updated source of information that is easy to access and search, along with links to useful multimedia sources.
I was born and raised in Chattanooga. After graduating from the University of Virginia, I attended Baylor College of Medicine. I completed residency and fellowship training at the University of Cincinnati at the Children’s Hospital Medical Center. I received funding from the National Institutes of Health for molecular biology research of the gastrointestinal tract.
During my fellowship, I had the opportunity to work with some of the most amazing pediatric gastroenterologists and mentors. Some of these individuals included Mitchell Cohen, William Balistreri, James Heubi, Jorge Bezerra, Colin Rudolph, John Bucuvalas, and Michael Farrell. I am grateful for their teaching and their friendship. During my training with their help, I received a nationwide award for the best research by a GI fellow.
I have authored numerous publications/presentations including original research, case reports, review articles, and textbook chapters on various pediatric gastrointestinal problems. In addition, I have been recognized by Atlanta Magazine as a "Top Doctor" in my field multiple times.
Currently, I am the vice chair of the section of nutrition for the Georgia Chapter of the American Academy of Pediatrics. In addition, I am an adjunct Associate Clinical Professor of Pediatrics at Emory University School of Medicine. Other society memberships have included the North American Society for Pediatric Gastroenterology Hepatology and Nutrition (NASPGHAN), American Academy of Pediatrics, the Food Allergy Network, the American Gastroenterology Association, the American Association for the Study of Liver Diseases, and the Crohn’s and Colitis Foundation.
As part of a national pediatric GI organization called NASPGHAN (and its affiliated website GIKids), I have helped develop educational materials on a wide-range of gastrointestinal and liver diseases which are used across the country. Also, I have been an invited speaker for national campaigns to improve the evaluation and treatment of gastroesophageal reflux disease, celiac disease, eosinophilic esophagitis, hepatitis C, and inflammatory bowel disease (IBD). Some information on these topics has been posted at my work website, www.gicareforkids.com, which has links to multiple other useful resources.
I am fortunate to work at GI Care For Kids. Our group has 17 terrific physicians with a wide range of subspecialization, including liver diseases, feeding disorders, eosinophilic diseases, inflammatory bowel disease, cystic fibrosis, DiGeorge/22q, celiac disease, and motility disorders. Many of our physicians are recognized nationally for their achievements. Our group of physicians have worked closely together for many years. None of the physicians in our group have ever left to join other groups. I have also worked with the same nurse (Bernadette) since I moved to Atlanta in 1997.
For many families, more practical matters about our office include the following:
– 14 office/satellite locations
– physicians who speak Spanish
– cutting edge research
– on-site nutritionists
– on-site psychology support for abdominal pain and feeding disorders
– participation in ImproveCareNow to better the outcomes for children with inflammatory bowel disease
– office endoscopy suite (lower costs and easier scheduling)
– office infusion center (lower costs and easier for families)
– easy access to nursing advice (each physician has at least one nurse)
I am married and have two sons (both adults). I like to read, walk/hike, bike, swim, and play tennis with my free time.
I do not have any financial relationships with pharmaceutical companies or other financial relationships to disclose. I have helped enroll patients in industry-sponsored research studies.

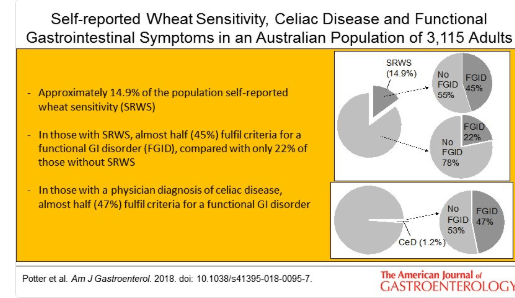
A recent study (MDE Potter et al. Am J Gastroenterol 2018; 113: 1036-44 -thanks to Ben Gold for this reference) examined the frequency of wheat intolerance and chronic gastrointestinal symptoms in a randomly selected population of 3542 in Autstralia via a mail survey.
Key findings:
- Self-reported wheat sensitivity was 14.9%
- Prevalence of celiac disease (CD) was 1.2%
- A doctor-diagnosis of CD was associated with functional dyspepsia with an odds ratio (OR) of 3.35.
- Self-reported wheat sensitivity was independently associated with irritable bowel syndrome with an OR of 3.55 and almost half (45%) have an underlying functional GI disorder.
In a related editorial (pgs 945-8), Imran Aziz makes several useful points:
- Gluten-free industry has boomed in U.S. with retail sales going from $0.9 billion in 2006 to ~S24 billion in 2020.
- While previous studies have shown that gluten can induce symptoms in the absence of CD (Biesiekierski JR et al. Am J Gastroenterol 2011; 106: 508-14), more recent rigorous studies have indicated that “gluten-per-se accounts for 1-in-6 cases with the remaining majority either due to fructans (a type of FODMAP or a nocebo effect.”
- There are no accurate biomarkers of wheat intolerance
- Dr. Aziz also cautions against adopting a gluten-free diet without proper counseling. “The greatest concern is whether these diets are safe in the long-run, given the emerging data suggesting cardiovascular, nutritional, metabolic, and microbial changes.”
My take: This study shows that about 1 in 10 individuals have self-reported wheat intolerance; gluten, though, is the actual culprit in less than 20%.
Related Blog Posts:
A recent study (L Norsa et al. JPGN 2018; 67: 361-6) examines data from 197 patients with celiac disease (CD) (out of a cohort of 337) who had a diagnosis established before 1985. The authors examined three groups: lifelong strict GFD (n=133), discontinued GFD (n=29), and no GFD (22). A total of 63 had follow-up endoscopy data available, with 29 in lifelong GFD, 20 in discontinued GFD, and 14 in no GFD.
Key findings:
- In those with followup endoscopy, in those with lifelong GFD 27 of 29 (93%) had no atrophy (Marsh 0-1-2) on histology, in those with discontinued GFD 12 of 20 (60%) had no atrophy on histology, and in those with no GFD 8 of 14 (57%) had no atrophy on histology.
- Thus, among the group with long-term poor adherence to gluten-free diet, almost two-thirds showed no recurrence of villous atrophy on duodenal biopsies.
- In the entire cohort of 197, there were no apparent differences in autoimmune diseases between those receiving lifelong GFD (26%) compared to the other two groups, 17% and 23% respectively.
Limitations:
- retrospective design.
- initial diagnosis was more than 30 years ago & there are significant differences in the diagnostic approach currently
- sample size
My take: This study indicates that some individuals who have been diagnosed with celiac disease may be OK with ongoing gluten consumption. Those who maintained a GFD were much more likely to have no villous atrophy on duodenal biopsies.
Related blog posts:

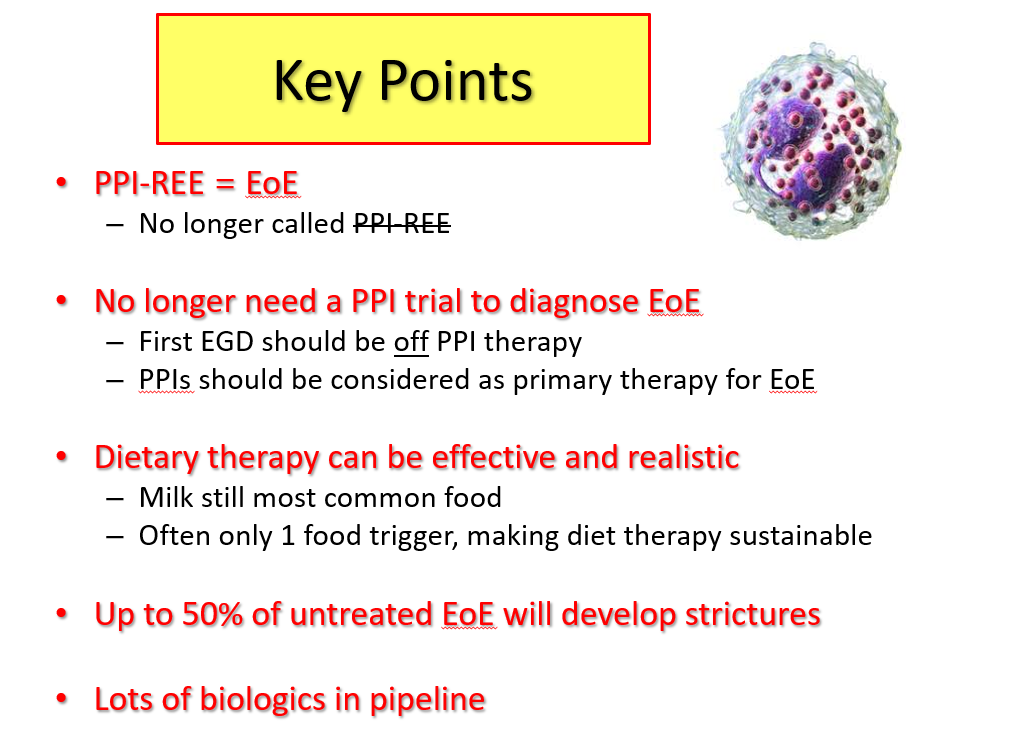
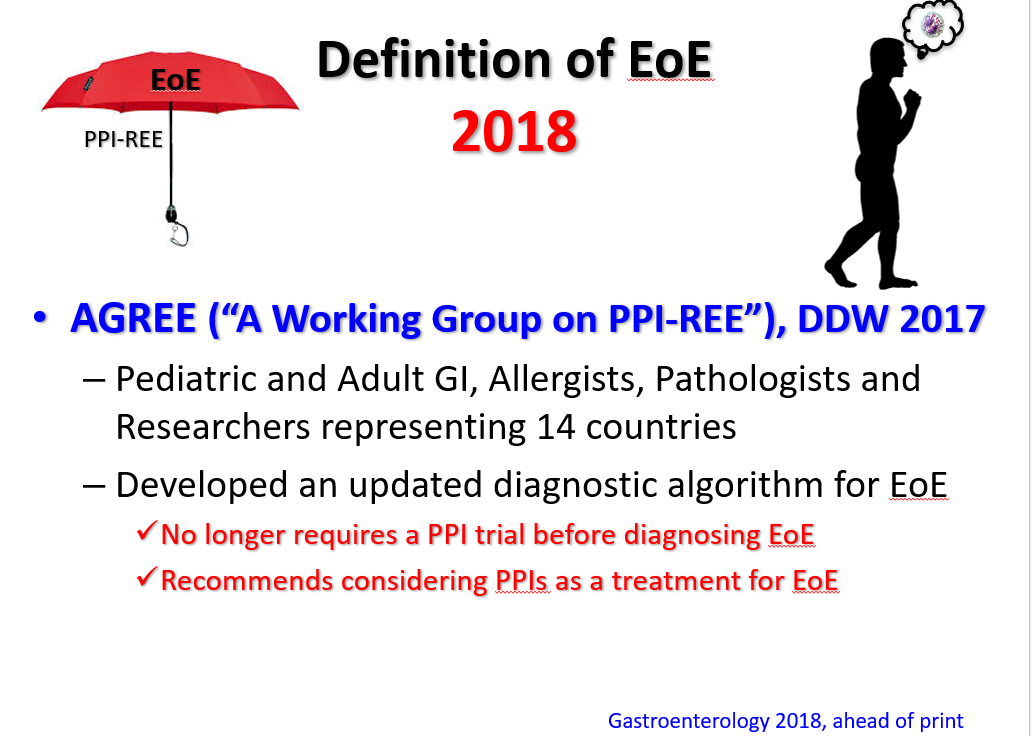
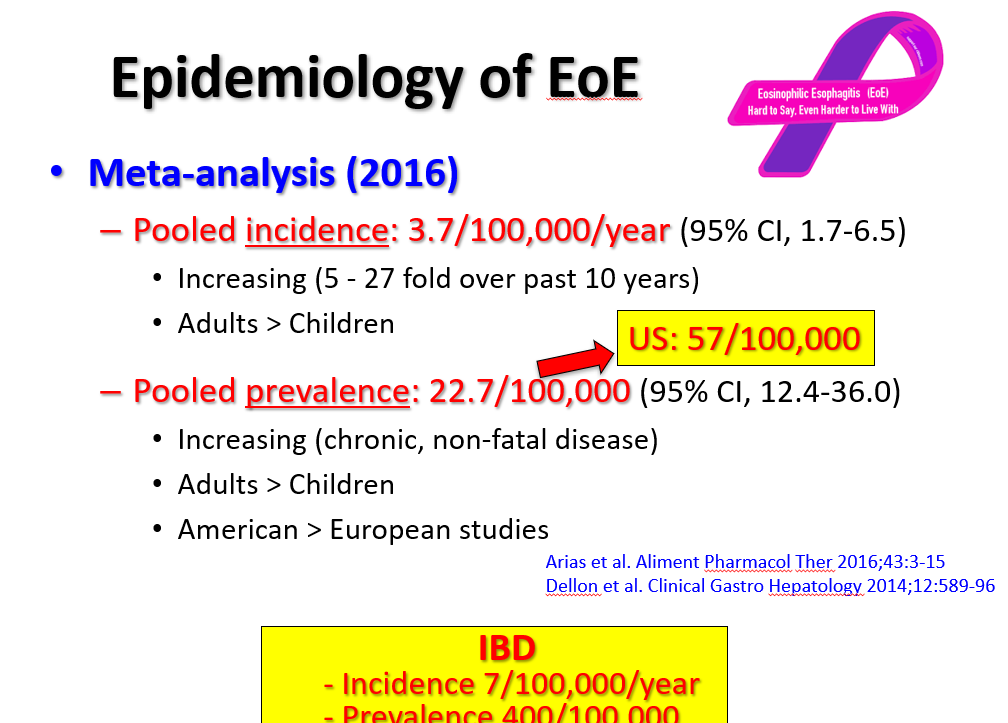
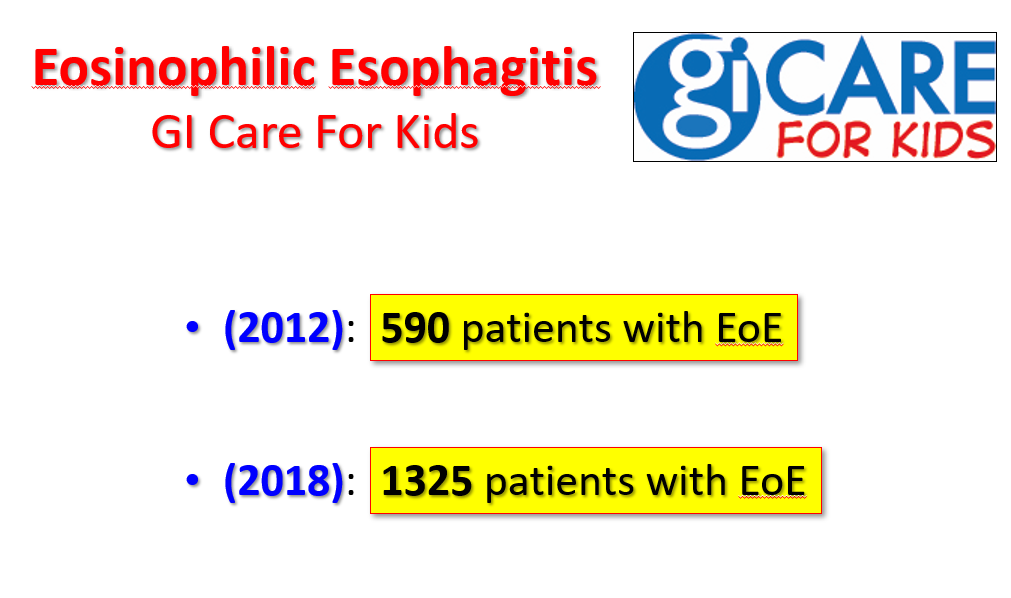
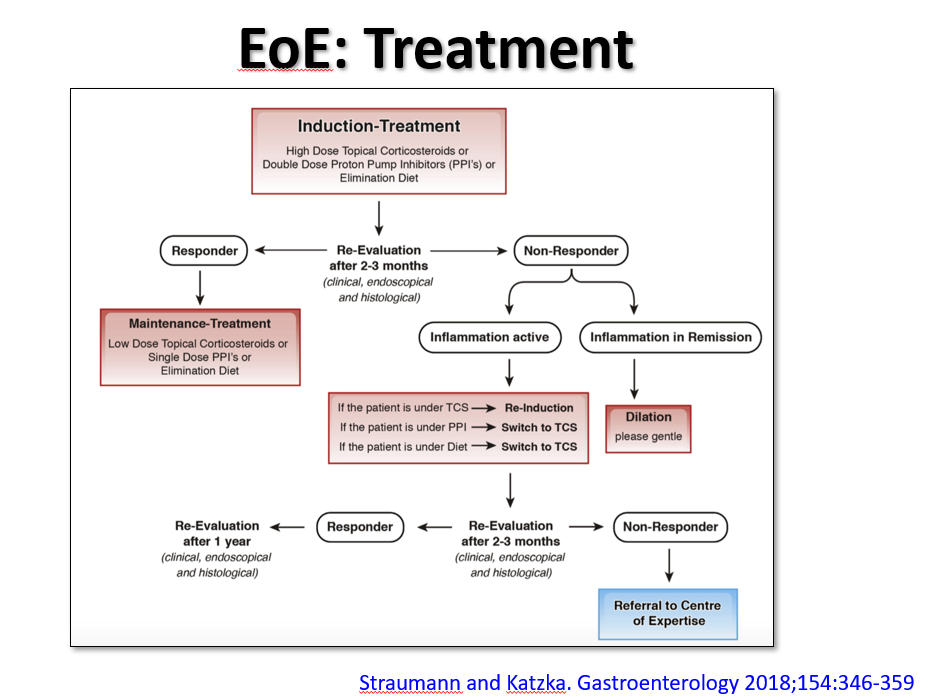
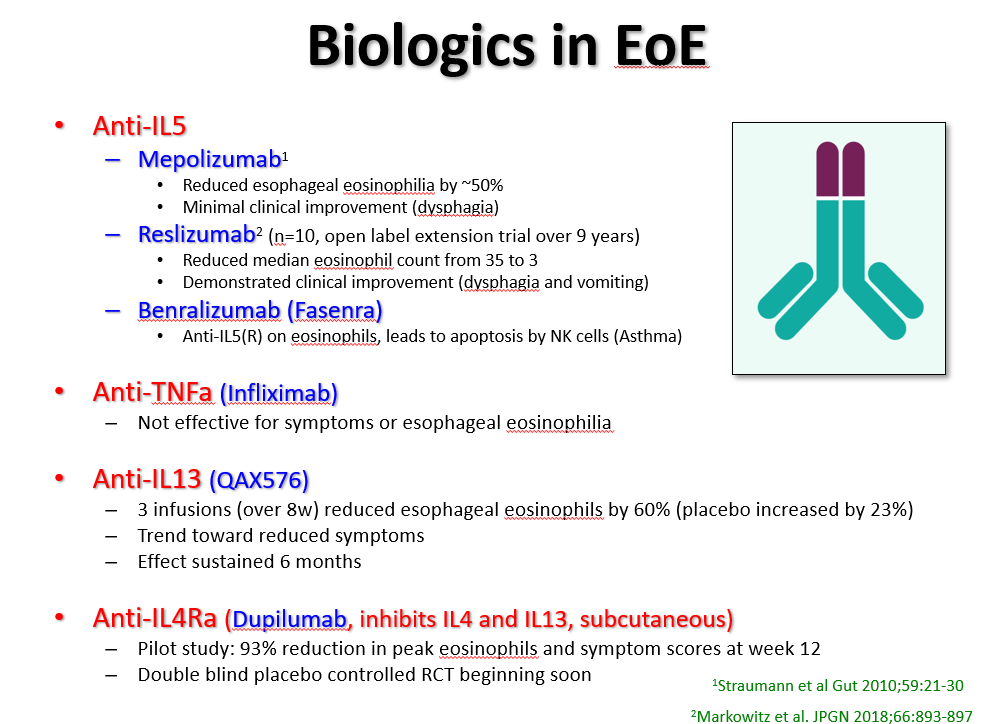
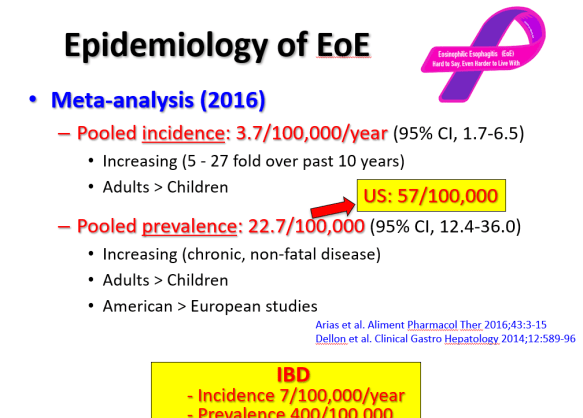
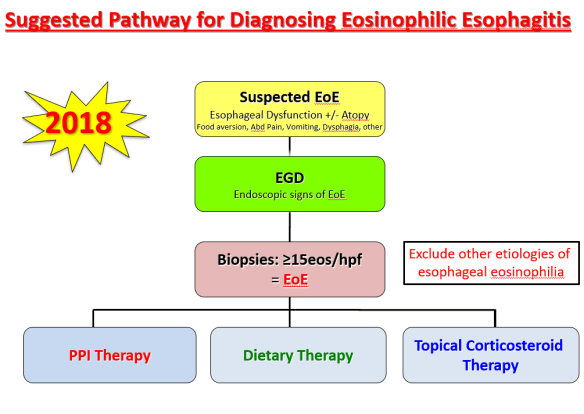
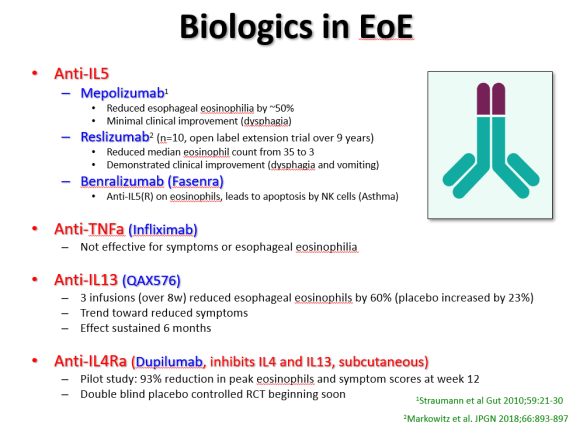
At a recent morning clinical conference, Dr. Seth Marcus provided a terrific update on eosinophilic esophagitis (EoE). I am placing some of the slides below and the following is a link to the full lecture: The Evolution of EoE -Seth Marcus
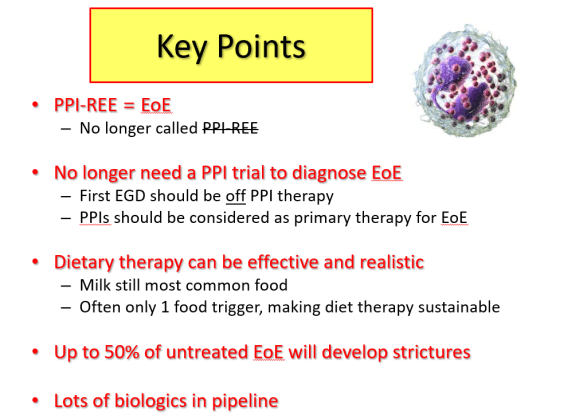

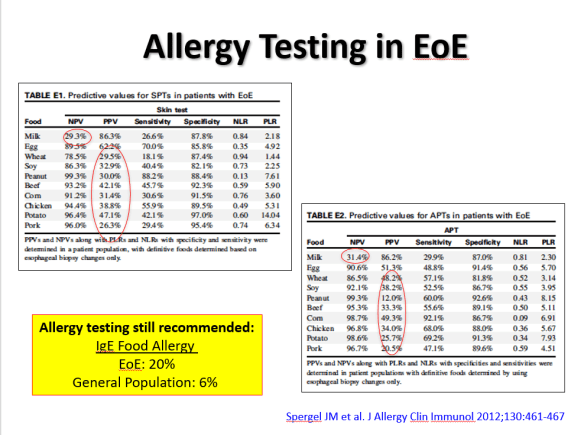
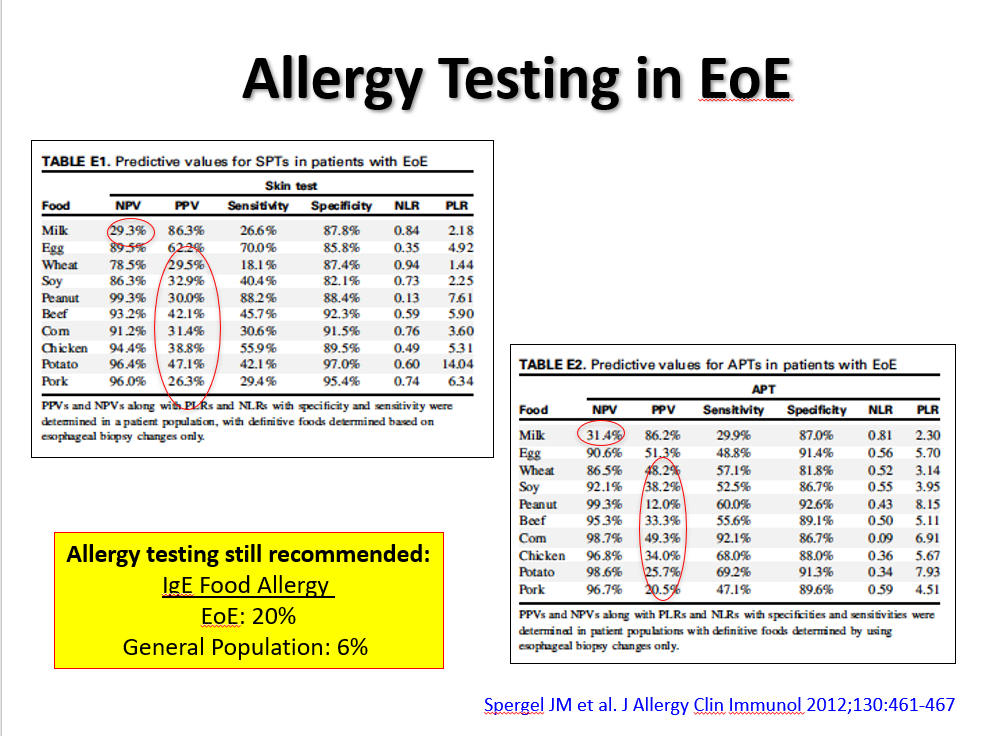
During this part of the presentation, there was a discussion regarding the role of allergists. Due to the poor predictive value (negative and positive) of allergy testing (skin tests and blood tests), the consensus is that routine allergy evaluation is NOT needed for children with EoE. However, IgE-mediated food allergies along with other atopic diseases are common in children with EoE and selected patients could benefit from allergy referral.
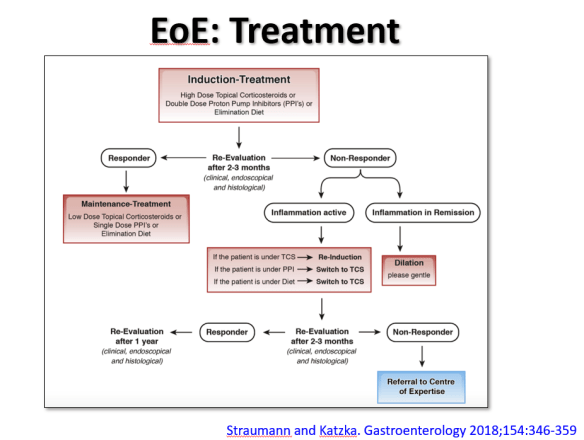
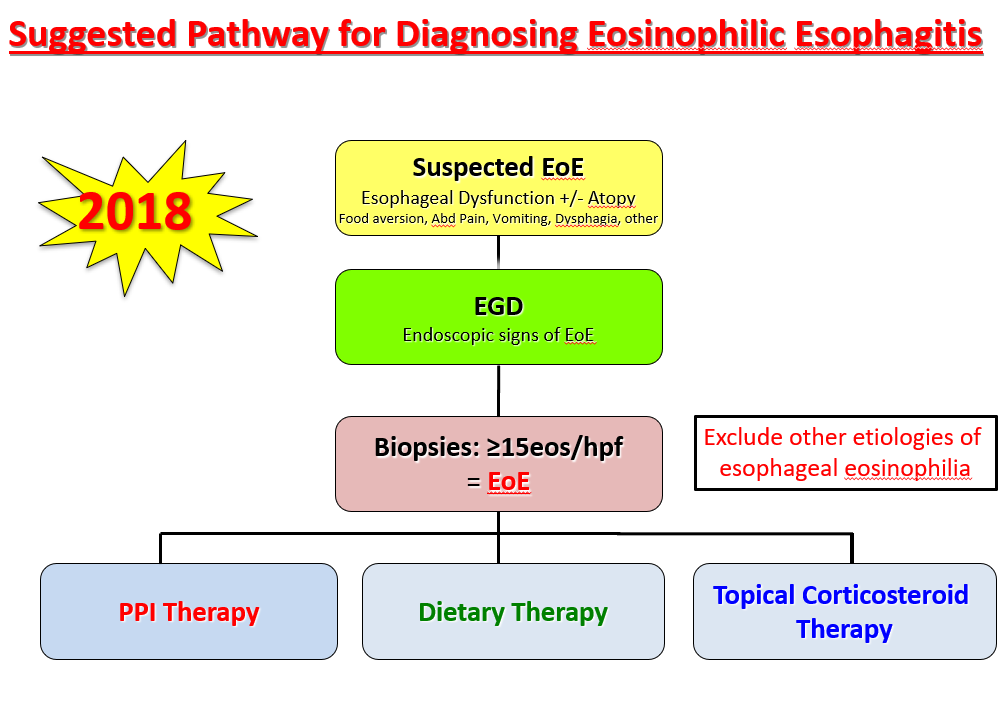
The slide above reviews the main treatment options: topical corticosteroids, proton pump inhibitor therapy, and elimination diet. While all of these are reasonable as first-line approaches, many in the group favored proton pump inhibitor (PPI) treatment as initial therapy. In those with a very good response (<5 eos/hpf at followup), this would allow lower dose PPI as a maintenance option. Another point of discussion was the fact that PPI responders tend to more favorably metabolize the PPIs to achieve higher therapeutic levels. It is anticipated that future treatment could be influenced by knowing the individual’s CYP2C19*17 Polymporphisms (#NASPGHAN17 EoE Session)
Related blog posts:
A recent prospective case-control study (J Molina-Infante et al. Am J Gastroenterol 2018; 113: 972-9 -thanks to Ben Gold for this reference) examined the potential connection between Helicobacter pylori and eosinophilic GI diseases. They examined 808 individuals (404 cases of eosinophilic esophagitis [EoE], 404 controls). Key findings:
- H pylori prevalence was not different between cases and controls (37% vs. 40%, odds ratio 0.97). The authors conclude that H pylori which has declined in prevalence globally is not inversely associated with EoE as had been suggested in some previous reports
In an associated editorial, (pg 941-4), the authors note that there has been a dramatic increase in atopic diseases over the past 30 years. One hypothesis has suggested that these epidemiologic changes are related to a changing microbiome. This in turn may be related to frequent antibiotic usage. An example of the proliferation of antibiotics: “20-25% of Swedish adults receive an antibiotic prescription annually.”
While H pylori may be a biomarker associated with poor hygiene/less antimicrobial exposure, it does not appear to be directly related to EoE. The authors indicate that until we have a better understanding, “in the meantime attention to healthier diets and minimizing antibiotic exposure may optimize public health in terms of atopic disease risk.”
My take: Since our genetics do not change quickly, the dramatic changes in disease frequency of conditions like EoE and Crohn’s disease must be influenced by environmental exposures. How to lower the risk of these conditions remains uncertain.
Related blog posts:

Not a joke –WIFI hotspot at Sunshine Meadows, Banff National Park
Briefly noted: B Singh et al. J Pediatr 2018; 200: 79-83. In this study of 87 infants witth birth weights 1500-2000, avoiding routine assessment of gastric residual volumes before feeding advancement did not shorten the time to reach full feeds. However, checking these residuals provided no clear advantages and have some potential disadvantages:
- Time-consuming to check and may inaccurate depending on size/location of orogastric/nasogastric tube
- Discarding gastric contents results in loss of gastric enzymes and acid
The authors note that prior studies have shown that gastric residuals are “unreliable predictors of feeding intolerance” studies have had discrepancies with regard to whether they are predictive of necrotizing enterocolitis.
Related blog post: When to Check Gastric Residuals in Preterm Infants

NY Times Commentary by Marcia Angell: Transparency Hasn’t Stopped Drug Companies From Corrupting Medical Research
Dr. Angell, a former editor of the New England Journal of Medicine examines the recent outrage regarding Dr. José Baselga who resigned from his position as chief medical officer at Memorial Sloan Kettering Cancer Center after “ProPublica and The New York Times revealed that he’d received millions of dollars from drug and device companies … Most of his outside income was not disclosed to the journals in which he published, in violation of their requirements.” Dr. Baselga has had a huge impact in cancer research; his work led to the discovery of Herceptin, a widely used treatment for breast cancer.
- She argues that disclosure alone is not sufficient to prevent pharmaceutical companies from corrupting research:
- “Drug company involvement biases research in ways that are not always obvious, often by suppressing negative results. A review of 74 clinical trials of antidepressants, for example, found that 37 of 38 positive studies — that is, studies that showed that a drug was effective — were published. But 33 of 36 negative studies were either not published or published in a form that conveyed a positive outcome.”
- “Bias can also be introduced through the design of a clinical trial. For example, the sponsor’s drug may be compared with another drug administered at a dose so low that the sponsor’s drug looks more powerful.”
- “Disclosure is better than no disclosure, but it does not eliminate the conflict of interest. It’s simply a way of … leaving it to readers to decide whether the research was biased. But most people — even doctors and science reporters — aren’t really equipped to make those judgments, particularly when data are suppressed.”
- She argues that drug companies should have “no control over the design, interpretation and publication of trial results” and that “doctors should not accept gifts from drug companies, even small ones, and they should pay for their own meetings and continuing education, as is standard in other professions.”
My take (borrowed from author): “we should not let drug companies buy the hearts and minds of researchers. The cost of this is high, and not just in drug prices. It means both doctors and patients believe prescription drugs are better and safer than they really are.”
Related posts:


Hillel quote at Mercedes Benz Stadium
A recent retrospective study (G Aljomah et al. JPGN 2018; 67: 351-5) provides some useful information about anemia in the pediatric inflammatory bowel disease (IBD) population. This study included 153 patients, though the diagnostic tests varied considerably; for example, only 42 patients had a serum transferrin receptor (sTR) assay available at followup.
Key points:
- 67.3% of patients had anemia at diagnosis. 38.5% had anemia of chronic disease (ACD) and the remainder had either iron deficiency anemia (IDA) or IDA in combination with ACD.
- 20.5% had anemia at followup approximately 1 year after diagnosis. 5.1% with ACD alone and 15.4% had IDA or IDA in combination with ACD.
- In a subset of patients with more complete data, it was shown that anemia was much more common in patients with Crohn’s disease: 91.2% at diagnosis and 27.3% at followup compared with patients with ulcerative colitis with 40.0% at diagnosis and 7.7% at followup.
The authors used the sTR index (sTR/log ferritin index) to determine if ACD was present. “This index can differentiate IDA from ACD; however, it cannot separate IDA from the combination of IDA/ACD. IDA or IDA/ACD were considered to be present if the sTR index was greater than 1.03. An sTR index of <1.03 was taken to be indicative of the presence of ACD.”
Briefly noted: MR Serpico et al. JPGN 2018; 67: 341-5. This retrospective study examined the use of allopurinol to optimize thiopurine levels. 32 of 52 patients remained on the combination for 1 year. In this group, median alanine transaminase decreased to 19 from 77 (P<0.001) and median 6-TG levels increased to 322 from 166 (P<0.001). In addition, steroid-free remission rates improved to 82% (23 of 28). About 40% of the initial cohort of 52 patients were switched to antitumor necrosis factor therapy.
My take: The initial study shows that anemia is frequent in pediatric IBD, especially at diagnosis (67%). Even at followup, 20% of patients had ongoing anemia.
Related blog posts:
A recent study (M-L Blank, et al. JPGN 2018; 67: 335-40) showed that proton pump inhibitors (PPIs) do not appear to increase the risk of pneumonia in otherwise healthy infants.
This study used a cohort of 21,991 patients (2005-2012) in New Zealand and examined the use of a PPI (omeprazole, lansoprazole, or pantoprazole) and its association with lower respiratory tract infections (566 validated cases) and 65 cases of radiography-confirmed community acquired pneumonia (CAP). For each LRTI and each CAP, there were 10 matched controls.
Key findings:
- Neither current nor recent use of a PPI was associated with an increased risk of CAP or LRTI resulting in hospitalization or death.
- The matched odds ratio for CAP with current or past use of PPI was 0.88 and for all LRTI cases the matched odds ratio was 1.13.
My take: This study indicates that PPIs are unlikely to contribute to respiratory infections in otherwise healthy infants. The larger question is how many of these infants really should be receiving PPIs and what other adverse consequences that may occur.
Related blog posts:

A recent study (K Wong et al. J Pediatr 2018; 200: 188-95) examined a longitudinal cohort of 323 females in the Australian Rett Syndrome Study.
Key findings:
- 30.3% of the cohort underwent gastrostomy placement
- BMI was greater in individuals with gastrostomy placement
- Median age of gastrostomy placement was 9 years
- The all-cause mortality rate was greater in those who had gastrostomy placement compared with those who had not (hazard ratio 4.07, CI 1.96-8.45)
- Survival: 66.1% of the entire cohort was alive at 20 years of age (median survival was 33 years). The survival was 87.3% in those without a gastrostomy.
- Placement of a gastrostomy tube was not associated with fewer hospitalizations or improvement in parental physical or mental health
While the mortality was higher in those who received a gastrostomy tube, the study’s nonrandomized design does not allow definitive assessment of whether a gastrostomy tube is detrimental to long-term survival. Children who received gastrostomy tube may have had additional comorbidities.
My take: In adult medicine, it is generally accepted that Gtube placement does not prolong life (Clin Gastro & Hep 2007; 5: 1372). This study indicates that a Gtube may not improve longevity in many pediatric disorders as well.
Related blog posts: