A recent study (J-M Schwarz et al. Gastroenterol 2017; 153: 743-52, editorial MB Vos, IR Goran Gastroenterol 2017; 153: 642-5 ) showed that restriction of fructose quickly improved fatty liver disease.
Several points from the editorial:
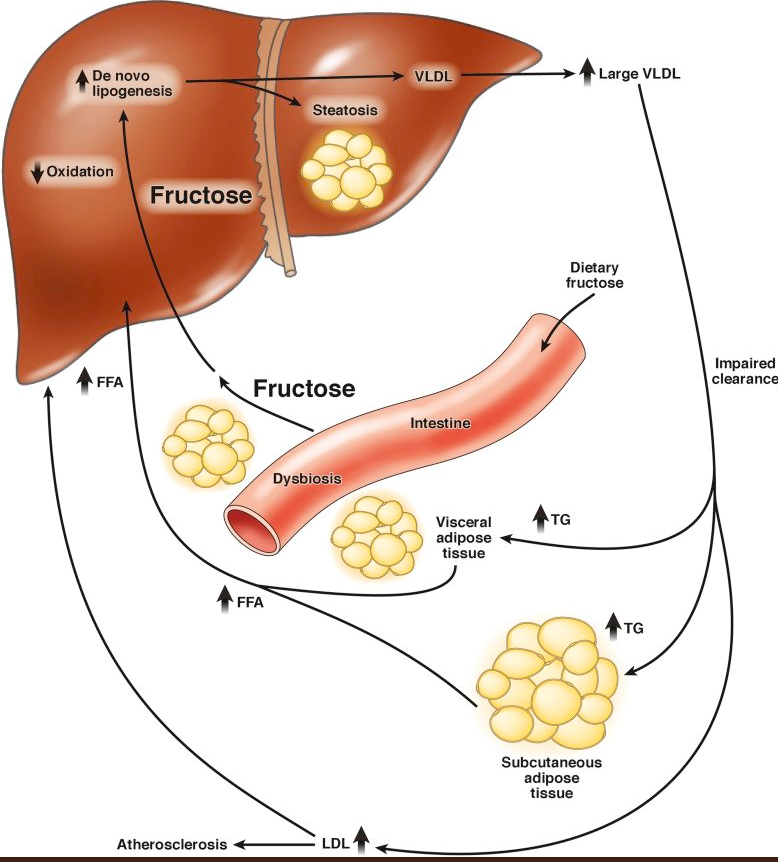
- “The metabolic driver of buildup of fat storage in the liver is de novo lipogenesis (DNL) and fructose is a major substrate of DNL”
- “In the healthy state, DNL is not expected to be a major contributor to lipid accumulation in the liver….[but] in a fatty liver, it has been estimated that 26% of the fat originates from DNL.”
- Fructose is “limited in a natural diet…However, it is added to many processed foods and drinks in the form of cane sugar..and other types of sugars, going by ≥57 different names.”
- Fructose is “commonly used in animal models to induce hepatic steatosis.”
The study is summarized in a recent AGA Journals Blog: Can Restricting Fructose Intake Reduce Fatty Liver Disease in Children?
An excerpt:
Jean-Marc Schwarz et al performed a clinical trial to investigate the effects of reducing fructose intake for 9 days in obese Latino and African American children with habitual high sugar consumption (fructose intake >50 g/day). They measured the effects of isocaloric fructose restriction on de novo lipogenesis, liver fat, visceral fat, subcutaneous fat, and insulin kinetics.
In their study, 41 children, 9−18 years old, had all meals provided for 9 days. The meals had the same energy and macronutrient composition as their standard diet, but with starch substituted for sugar, yielding a final fructose content of 4% of total kilocalories. The authors measured metabolic factors before and after fructose restriction. They measured liver fat, visceral fat, and subcutaneous fat by magnetic resonance spectroscopy and imaging.
Schwarz et al found that on day 10 of the diet, liver fat decreased from a median 7.2% at baseline to 3.8%, and visceral fat decreased from 123 cm3 at baseline to 110 cm3. Liver fat decreased in all but 1 of the 38 participants for whom paired data were available…
De novo lipogenesis decreased significantly after 9 days of fructose restriction; the de novo lipogenesis area under the curve value on day 10 decreased from 68% at baseline to 26% after the diet, in childen with low or high baseline levels of liver fat.
Insulin secretion during fasting and in response to an oral glucose tolerance test decreased significantly in children with low and high baseline levels of liver fat…
In an editorial that accompanies the article, Miriam B. Vos and Michael I. Goran say that it will be important to determine whether the effects of fructose reduction are sustained past 9 days…Vos and Goran state that it is important for physicians, nutritionists, schools, and parents to find ways to reduce fructose in the diets of children and patients with NAFLD.
Related posts:
- Proof that Diet Changes Can Improve a Fatty Liver
- When Will MRI Obviate the Need for a Liver Biopsy in Pediatric NAFLD?
- Concise Review: Fatty Liver in Pediatrics
- Reaching Consensus on Bariatric Intervention in Children and Adolescents
- Fatty Liver Improved with Exercise