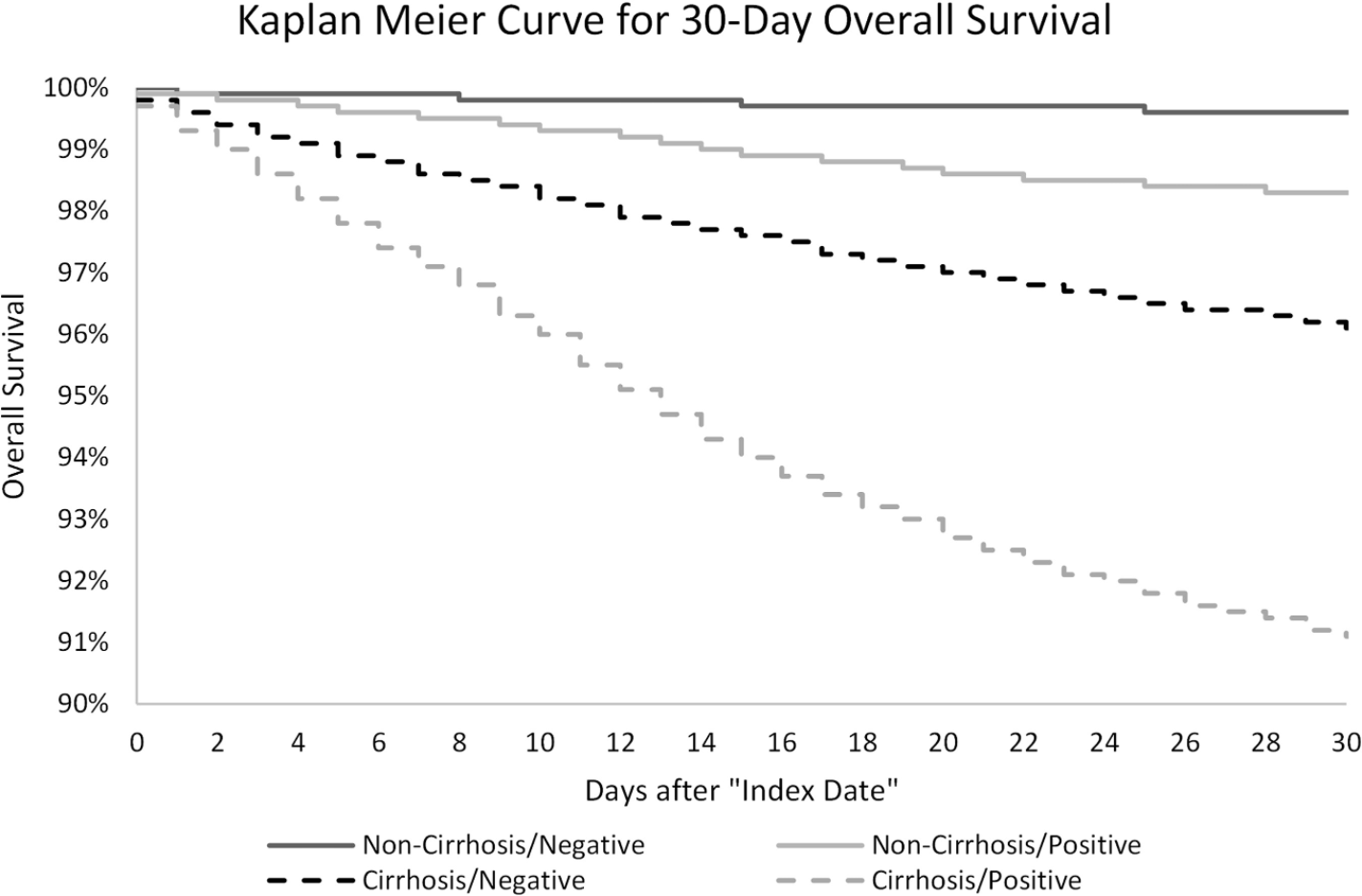
Key finding: “In this study of approximately 221,000 nationally representative, diverse, and sex-balanced patients with CLD; we found SARS-CoV-2 infection in patients with cirrhosis was associated with 2.38 times mortality hazard, and the presence of cirrhosis among patients with CLD infected with SARS-CoV-2 was associated with 3.31 times mortality hazard”
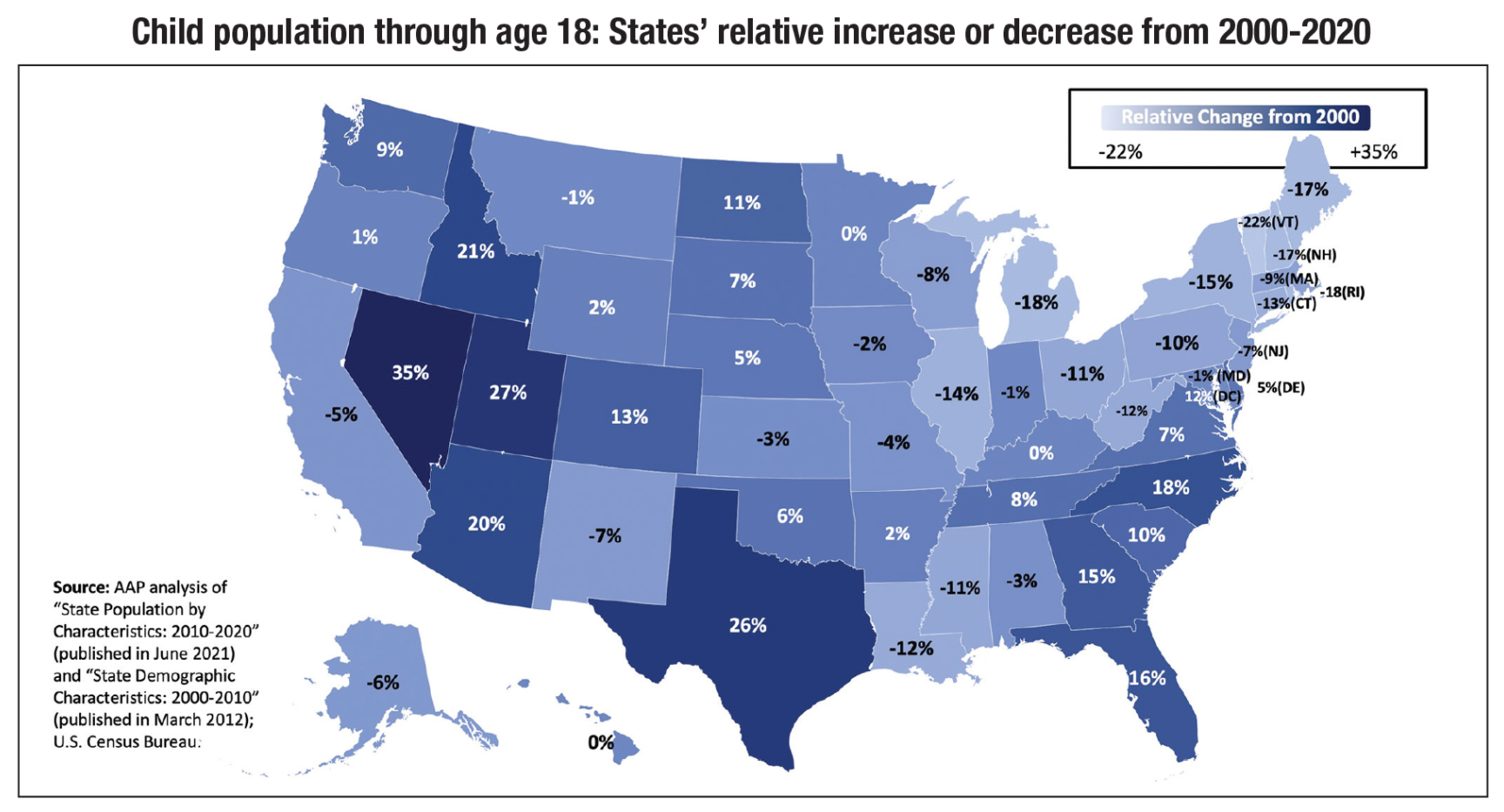
“An estimated 77 million children under age 19 live in the United States, according to the 2020 census. From 2000-’10, the U.S. child population grew by 2.1 million, but since 2010, there has been a decrease of 1.6 million children”
“Texas, Florida, North Carolina and Georgia are especially noteworthy. These are states with large populations that also had among the largest relative increases in the number of children. Since 2000, the number of children in Texas increased by 1.6 million, in Florida by 630,000, in North Carolina by 370,000 and in Georgia by 340,00”
“In 2020, children who are identified as non-White made up 50% of the child population compared to 39% in 2000. In 2020, Hispanic children made up 26%, Black children made up 14% and Asian children made up 5% of the child population”
“When faced with someone in a white coat, don’t go mute. Assert yourself, particularly if you’re confused. Try repeating what you’re hearing”
“People recalled less than half of what their doctors told them a week earlier”
”In practice, though, patients bring up as many as 15 different issues during a visit. Show up with a list of the three main things you want to talk about, and go over all three before your doctor starts talking.”
“Communication onus should be on medical providers. Still, as a patient, you have agency. ‘When people participate, they remember better'”
My take: This article makes some good points. I think in this era, more written information (after visit instructions) are being provided which helps as well.
To protect children from serious illness, long-term sequelae, hospitalization and death. USA Today recently estimated that less than 700 children have died from COVID-19 -which is still a lot of vaccine-preventable illness (yearly flu deaths in children are closer to about 100 per year). Link (10/8/21) How bad is COVID-19 in kids? See the latest data and charts on kids cases; hospitalizations; deaths
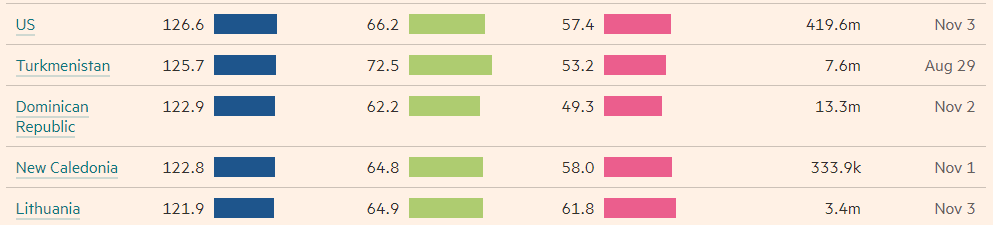
To protect everyone else (from Eric Topol twitter feed):
“Remarkably safe and highly effective mRNA COVID-19 vaccines are now available for widespread use and should be given to all adult patients with CLD and LT recipients. The online companion document located at https://www.aasld.org/about-aasld/covid-19-resources will be updated as additional data become available regarding the safety and efficacy of other COVID-19 vaccines in development.”
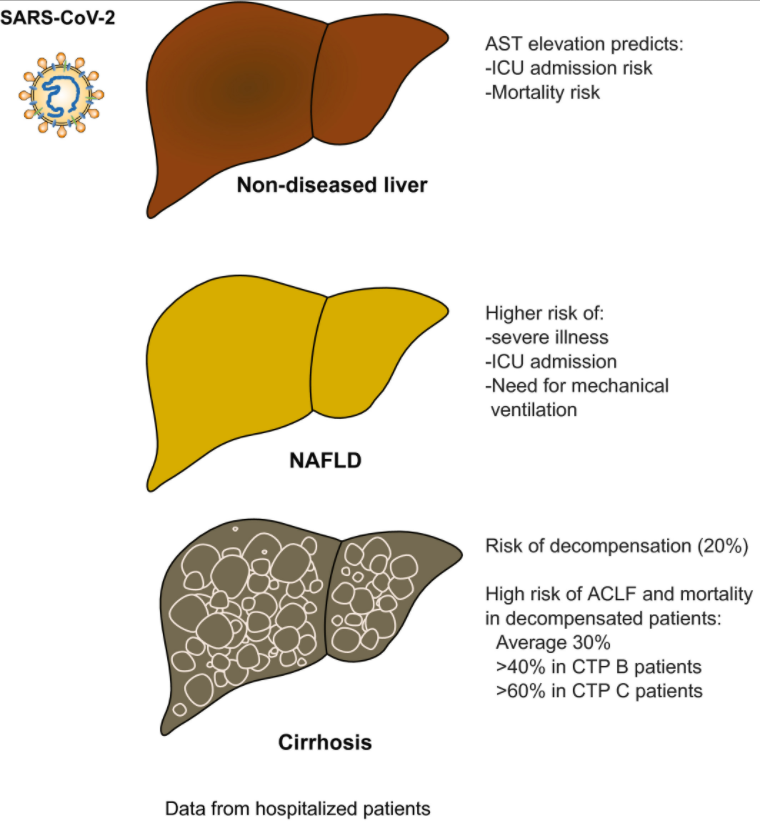
“The presence of liver injury is a surrogate marker for more severe disease and higher mortality in patients with COVID-19. An elevated AST level is the most robust predictor of poor outcome.”
“Liver injury and mortality in COVID-19 are likely multifactorial, driven by a sustained and excessive systemic release of proinflammatory and prothrombotic cytokines following SARS-CoV-2 infection, iatrogenic injury caused by DILI, hemodynamic changes associated with mechanical ventilation or vasopressor use, and worsening of underlying liver injury in those with CLD.”
“Risk of de novo liver injury appears limited in patients without CLD, and only rare cases of COVID-19–related ACLF [acute-on-chronic liver failure] were observed.”
“COVID-19–related liver injury and mortality in patients who were hospitalized with and without chronic liver disease (CLD). Patients without CLD usually present with AST elevation, which correlates with ICU admission and mortality. Among patients with CLD, NAFLD has the highest risk of severe illness, ICU admission, and need for mechanical ventilation. Patients with cirrhosis are at risk for decompensation, and patients who are decompensated have a high risk of acute-on-chronic liver failure (ACLF) and mortality.”–Abbreviations: CTP, Child-Turcotte-Pugh; ICU, intensive care unit.
“We are caring for young people with soaring rates of depression, anxiety, trauma, loneliness, and suicidality that will have lasting impacts on them, their families, their communities, and all of our futures,” said AACAP President Gabrielle A. Carlson, M.D. “We cannot sit idly by. This is a national emergency, and the time for swift and deliberate action is now.”
These organizations make several recommendations to policy makers including more access for mental health services. (I worry that we do not have sufficient numbers of qualified mental health practitioners to meet the challenge.)
“According to the study in Pediatrics, one of every 168 American Indian/Alaska Native children, one of every 310 Black children, one of every 412 Hispanic children, and one of every 612 Asian children have lost a caregiver, compared to one in 753 white children.”
This study which encompassed 397,395 total serum bilirubins provides an updated normogram for serum bilirubins in the first days of life. The data for this nomogram is based on 140 times the number of subjects and is derived from 15 years of universal bilirubin screening (Intermountain Healthcare Hospitals).
Key points:
The authors state that this study is one step “toward evidence-based phototherapy decision-making”
“We are currently using this nomogram [figure below] routinely in our hospitals in Utah for phototherapy initiation (when a neonate has a TSB exceeding the 95th percentile) and for discharge risk stratification.”
“This reduces phototherapy usage…to about 5% of well babies, whereas we had previously been administering phototherapy in 8-10% of well babies.”
“Newborns with TSB>75 percentile…receive a recommendation for follow-up within 24 hours.”
The authors acknowledge the limitations of their study and caution that more long term outcome data are needed in evaluation of their approach.
My take: Overall, the data is fairly similar to prior data but adoption of these slightly higher values would likely reduce the number of infants requiring phototherapy.
While pediatric gastroenterologists typically are not coordinating the management pediatric patients with Type 2 Diabetes Mellitus (T2DM), we certainly see many with T2DM and often are involved in some aspects of their care (eg. fatty liver disease).
This “TODAY2” study annually followed 500 participants from the TODAY trial (2011). The age of the participants was 26.4±2.8 years, and the mean time since the diagnosis of diabetes was 13.3±1.8 years.
Key definitions:
Hypertension: At 95% or greater for age (at least SBP 130 or DBP 80) on 3 consecutive visits and/or needing medical therapy
Dyslipidemia: Consecutive LDL values of at least 130, consecutive triglycerides of at least 150, or values requiring medical therapy
Albuminuria: ratio of urine albumin to creatinine of at least 30
Diabetic Nerve Disease: based on scores of Michigan Neuropathy Screening Instrument -consecutive values of at least 2 or more (scores range from 0 to 8)
Diabetic Eye Disease: based on a grade of at least 20 according to criteria of Early Treatment Diabetic Retinopathy Study criteria (grades range from 10 to 85)
Key findings:
The cumulative incidence of hypertension: 67.5%
The incidence of dyslipidemia: 51.6%
The incidence of diabetic kidney disease:54.8%
The incidence of nerve disease: 32.4%.
The prevalence of retinal disease: 13.7% (2010 to 2011) and 51.0% (2017 to 2018)
The authors note that the high incidence of complications is “most likely related to extreme metabolic phenotype (which includes severe insulin resistance and rapid worsening of beta-cell function) and to challenging socioeconomic circumstances.”
Study strengths: 15 years of prospective, extensive data and population representative of U.S.
My take: “Taken together, these data illustrate the serious personal and public health consequences of youth-onset” T2DM by age 26 years!! Unless medical therapies improve further, these consequences argue for careful consideration of bariatric surgery.
After expending a great deal of time and effort on prior authorizations lately, this recent satirical explanation on prior authorizations and the purpose of insurance companies hits the target. Though, insurance companies do make money off interest, I think the main goal of PA is to limit care costs. Some patients will not get the care their doctor recommends due to stalling by the insurance company. Many times it takes a physician hours in order to get approvals. If a patient’s physician is not willing to do this, many times the patient will not get the treatment.