COVID-19 Advice from CHOA:

D Kim et al. Clin Gastroenterol Hepatol 2021; 19: 1469-1479. Full text: Predictors of Outcomes of COVID-19 in Patients With Chronic Liver Disease: US Multi-center Study
Key findings:
- The overall all-cause mortality in this cohort with chronic liver disease was 14.0% (n = 121 of 867), and 61.7% (n = 535) had severe COVID-19
- Liver-specific factors associated with independent risk of higher overall mortality were alcohol-related liver disease (ALD) (hazard ratio [HR] 2.42), decompensated cirrhosis (HR 2.91) and hepatocellular carcinoma (HCC) (HR 3.31)
- Related blog post: Aspen Webinar 2021: COVID-19 and the Liver
BK Elmunzer et al (>120 authors!) Clin Gastroenterol Hepatol 2021; 19: 1355-1365. Full text: Digestive Manifestations in Patients Hospitalized With Coronavirus Disease 2019
Key findings:
- In this cohort with 1992 patients hospitalized with COVID-19, gastrointestinal symptoms and liver test abnormalities were common, but the majority were mild and their presence was not associated with a more severe clinical course: GI symptoms had OR of 0.93 and liver test abnormalities had OR of 1.31 for mechanical ventilation or death.
- Common GI symptoms: diarrhea (34%), nausea (27%), vomiting (16%), and abdominal pain (11%). 35% of patients developed an abnormal alanine aminotransferase or total bilirubin level; these were increased to less than 5 times the upper limit of normal in 77% of cases.
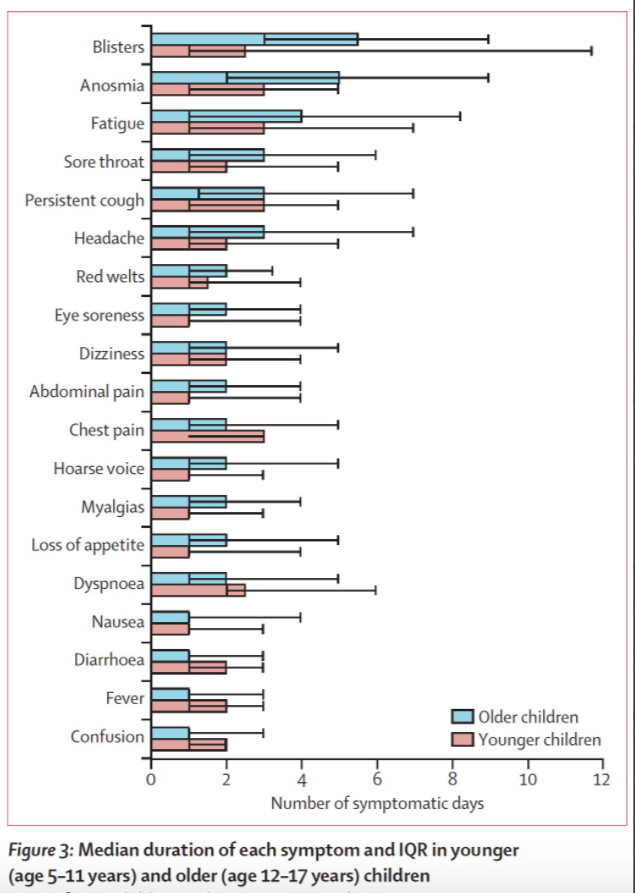
Lancet Child Adolesc Health 2021. Published Online August 3, 2021. https://doi.org/10.1016/S2352-4642(21)00198-X. Open Access: Illness duration and symptom profile in symptomatic UK school-aged children tested for SARS-CoV-2.
- Key finding: In this prospective cohort study, 25 of 1379 (1.8%) children (5-17 yrs) had symptoms lasting at least 56 days and 4.4% had symptoms lasting more than 4 weeks.

Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.