JD Groarke, et al. NEJM 2024; 391: 2291-2303. Ponsegromab for the Treatment of Cancer Cachexia
Background: “Growth differentiation factor 15 (GDF-15) is a stress-induced cytokine that binds to the glial cell–derived neurotrophic factor family receptor alpha-like protein (GFRAL) in the hindbrain.12 The GDF-15–GFRAL pathway has emerged as a main modulator of anorexia and body-weight regulation and is implicated in the pathogenesis of cachexia.13 …Ponsegromab (PF-06946860) is a potent, highly selective, humanized monoclonal antibody that binds to circulating GDF-15, thereby inhibiting the interaction with its GFRAL receptor.”
“A recent guideline supports low-dose olanzapine to improve appetite and weight in patients with advanced cancer,3 a recommendation that is largely based on a single-center study.4 Safe, effective, and targeted therapies for cancer cachexia are needed.10,11“
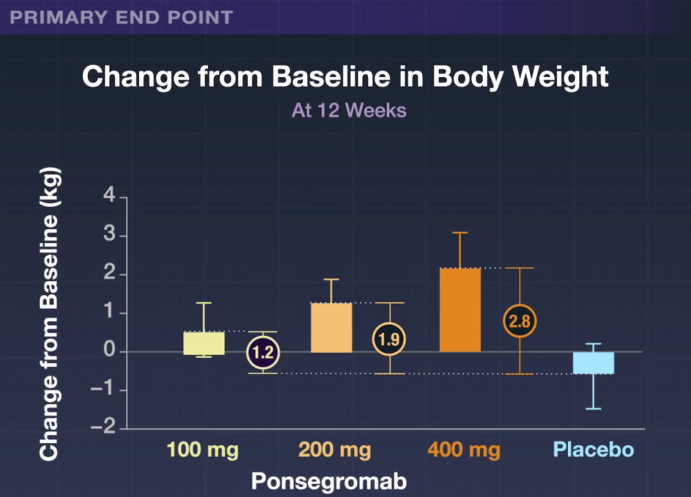
Methods: In this phase 2, randomized, double-blind, 12-week trial, we assigned patients with cancer cachexia and an elevated serum GDF-15 level (≥1500 pg per milliliter) in a 1:1:1:1 ratio to receive ponsegromab at a dose of 100 mg, 200 mg, or 400 mg or to receive placebo, administered subcutaneously every 4 weeks for three doses. N=187. Of these patients, 40% had non–small-cell lung cancer, 32% had pancreatic cancer, and 29% had colorectal cancer.
Key findings:
- Over the 12-week trial, patients treated with ponsegromab had as much as a 2.8 kg weight gain compared to placebo.
- Improvements were observed across measures of appetite and cachexia symptoms, along with physical activity, in the 400-mg ponsegromab group relative to placebo.

My take: This study explains a key driver of cachexia in cancer and shows that inhibition of GDF-15 can improve weight gain and physical activity.