Notes from this year’s Aspen Webinar 2021. This blog entry has abbreviated/summarized some of these presentations. Though not intentional, some important material is likely to have been omitted; in addition, transcription errors are possible as well. The first talk was excellent.
What’s Hot -COVID-19 and the Liver William Balistreri
This lecture covered a ton of information and publications with regard to COVID-19 and the liver.
Key points:
Numerous studies generally show that liver problems related to COVID-19 are mild, particularly in children
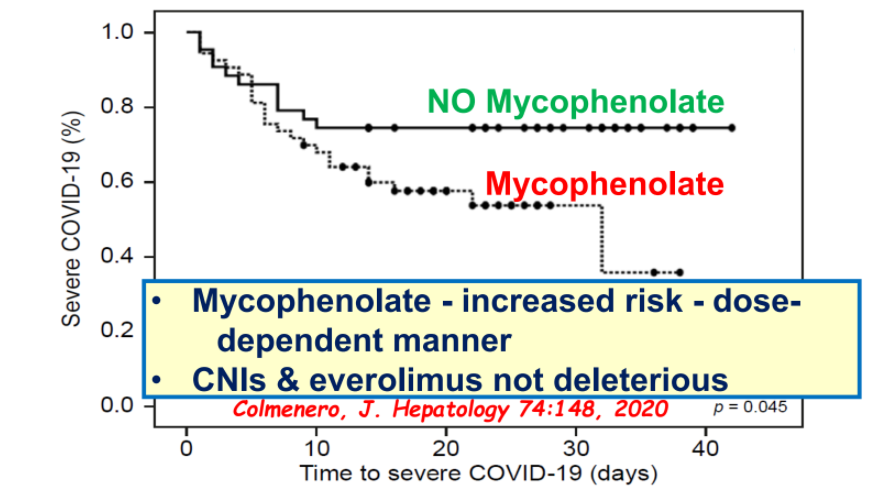
Most immunosuppression agents do not worsen outcomes with COVID-19 and should not be reduced in autoimmune hepatitis or liver transplantation; the exception, mycophenolate has been associated with worsened outcomes
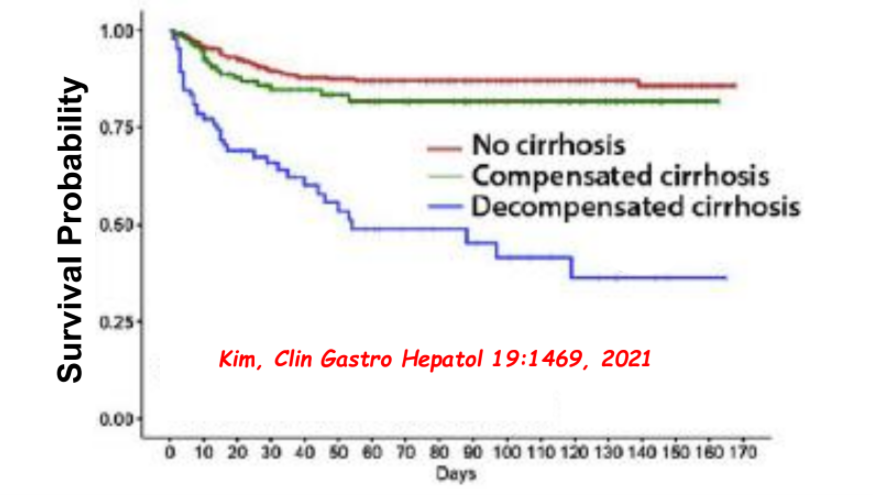
Cirrhosis is associated with worse outcomes in patients with COVID-19
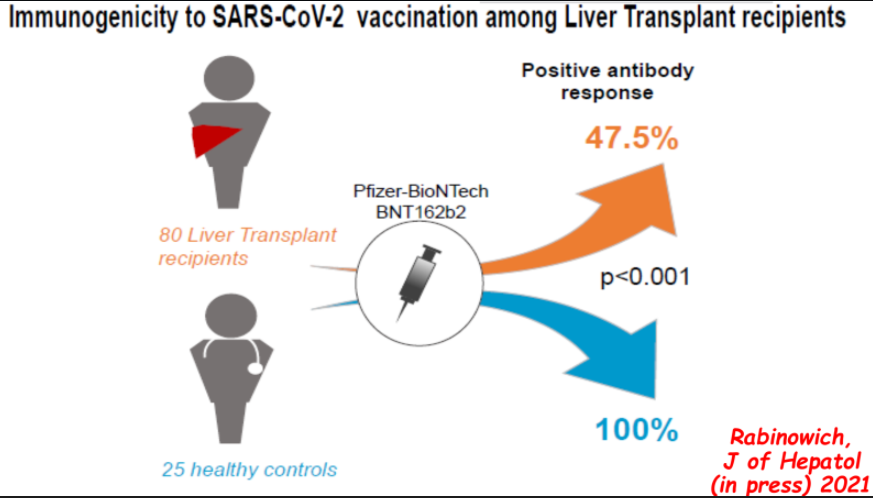
Vaccine response is blunted in immunocompromised patients with 40-50% developing antibody response after two doses of mRNA vaccines and generally lower titers. 3rd dose of vaccine may improve response.
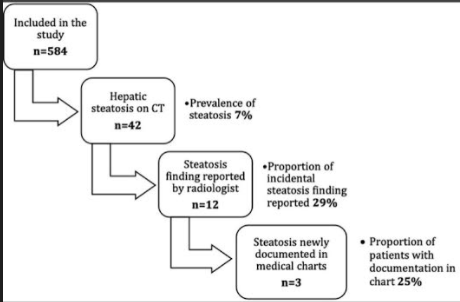
Using absolute liver attenuation <48 Hounsfield units (HU), the prevalence was 7% (n = 42/584). Steatosis was reported for only 12 of 42 (28%) of these patients and was documented in clinical notes in only 3 of those cases
232 (40%) had liver enzymes available within 24 hrs of CT scan. 79 had elevated ALT values; steatosis accounted for only 22% of those with elevated ALT values
In those with liver attenuation < 48 HU, nearly all had abnormal ALT values and the median was 52 U/L
Patients with steatosis had an 8-fold likelihood of overweight/obesity
Discussion:
These findings are similar to an adult study of 1290 patients in which 26% had steatosis but only 5% had those findings identified and documented beyond the radiology report. (N Kutaiba et al. J Med Imaging Radiat Oncol 2019; 3: 431-8)
CT findings are considered much more accurate than ultrasonography.
The authors argue that identification of NAFLD is “crucial” to allow for further specialty evaluation and to exclude secondary causes of steatosis.
My take: This study shows that there is an opportunity to improve identification of incidental steatosis. If identified, this can/should be addressed by their primary care team to emphasize improved diet choices and physical activity.
This single-center retrospective study with 43 patients (over 11 year timeframe) identified etiology and outcomes for neonatal acute liver failure (NALF).
Key findings:
Etiologies included viral infection (23%), gestational alloimmune liver disease with neonatal hemochromatosis (GALD-NH) (21%), cardiac-associated ischemia (16%), other ischemia (14%), genetic etiologies (9%), Trisomy 21-associated myelodysplasia (TAM) (7%), hemophagocytic lymphohistiocytosis (HLH) (2%), and not identified (7%)
Infants with viral etiologies had the highest alanine aminotransferase (ALT) at presentation (1179 IU/L, interquartile range [IQR] 683–1585 IU/L) in contrast to low levels in GALD-NH (23 IU/L, IQR 18–64 IU/L)
Across all etiologies, only 33% were alive at 1 year
Among laboratory values at presentation, alpha-fetoprotein (AFP) was significantly higher in patients that survived with their native liver (P = 0.04)
Figure 4 provides a helpful management algorithm for NALF. Figure 4 is similar to the slide below (shared by lead author).
-Consider empiric acyclovir in those with INR >/= 2.0 in the first 30 days of life
-In those with normal to low elevation of aminotransferases, consider empiric IVIG while undergoing workup. Part of workup should include either MRI or lip biopsy for GALD
-In those with moderate to severe elevation of aminotransferases, workup should include assessment for viral, HLH and genetic etiologies. Fulminant viral hepatitis or HLH likely with Ferritin levels >10,000. Hypoglycemia and hyperammonemia is suggestive of metabolic/mitochondrial disorder
-Liver biopsy may be needed if etiologies not identified
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
This is highly technical study of 60 patients with AIH. “Our key finding was a clearly biased signature of TRBV-J gene usage in peripheral and liver-infiltrating T-cells of patients with AIH, independent of AIH predisposing HLA-DRB1 alleles. This signature was unaffected by immunosuppressive treatment and not related to complete biochemical disease remission. This suggests that treatment acted on T-cell functionality rather than on the underlying pathological T-cell architecture in this disease that has a high relapse rate.”
My take (borrowed from authors): “Patients with AIH show profound and persisting T-cell architectural changes that may explain high relapse rates after tapering immunosuppression.”
Using a community-based sample of 235 children, the authors found that there was a significant negative relationship between liver MRI-PDFF and BMD z score R = −0.421, P < .001).
There was no significant association between vitamin D status and BMD z score (P = .94).
Children with clinically low BMD z scores were found to have higher alanine aminotransferase (P < .05) and gamma-glutamyl transferase (P < .05) levels compared with children with normal BMD z scores.
My take: This study shows another organ that is affected in children with fatty liver disease; other associated problems include increased risk for cardiovascular disorders, pancreatic dysfunction/diabetes, cancer, polycystic ovary syndrome, and neurologic disorders
A Louvet et al. Hepatology 2021; 73: 1945-1955. Acute Liver Injury With Therapeutic Doses of Acetaminophen: A Prospective StudyThis prospective study (2002-2019) showed that 89 of 400 adult patients with acetaminophen-induced acute liver injury (ALI) had received therapeutic doses of acetaminophen (<6 g). Especially in individuals with underlying alcoholic liver disease or fasting, acetaminophen (more than 2 gm/day) can trigger liver injury.
JE Eaton et al. Hepatology 2021; 73:1868-1881.Early Cholangiocarcinoma Detection With Magnetic Resonance Imaging Versus Ultrasound in Primary Sclerosing Cholangitis This multicenter retrospective study showed that MRI is superior to ultrasound for the detection of early-stage CCA in patients with PSC. Identification of CCA before the onset of symptoms with MRI is associated with improved outcomes. The authors note that individuals diagnosed with CCA while asymptomatic had a 36% reduction in 5-year mortality and that MRI allowed for a 77% reduction in 5-year mortality among asymptomatic persons. One important limitation of this study would be lead-time bias; that is, those with disease detected at an earlier stage will live longer than those detected at a later stage and thus earlier diagnosis may be ascribed as conferring a greater longevity even with no intervention.
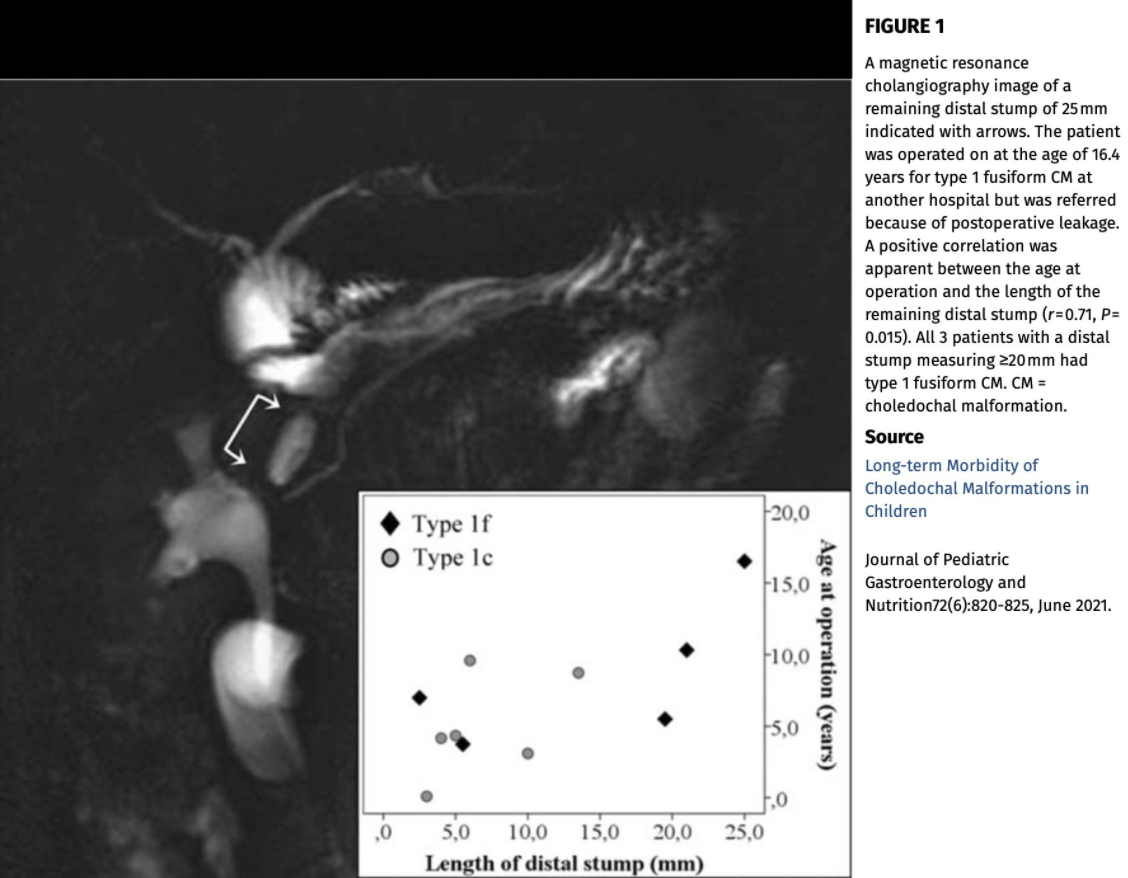
This single-center retrospective study (n=55 median f/u 6 years) provides data on long-term morbidity of choledochal malformations. Key findings:
21% had long-term complications including cholangitis in 9 (>2 episodes in 5) patients, anastomotic stricture in 2, adhesive volvulus in 1 and hepatocellular carcinoma in 1.
Magnetic resonance cholangiography (MRCP) performed 6.4 (3.6–16) years after hepaticojejunostomy, diameters of both main intrahepatic ducts had decreased significantly to 3.0 (2.5–3.5) mm (P = 0.0001) but a distal cyst stump was remaining in 30% with a length of 6.0 (4.0–20) mm
My take: Despite surgical management (hepaticojejunostomy), biliary tract malignancy is still possible in patients with choledochal cysts. Regular CA 19-9 testing is probably worthwhile, especially in teens and older. The authors note that in patients with type 1 choledochal malformations, some have recommended annual liver biochemistries and ultrasonography following successful surgery (J Gastroenterol Hepatol 2019; 34: 966-974).
METHODS: Multicenter, retrospective cohort study of patients aged ≤18 years with overweight and obesity and evidence of elevated serum aminotransferases and/or hepatic steatosis on imaging, referred for suspected NAFLD to Cincinnati Children’s Hospital Medical Center (2009–2017) or Yale New Haven Children’s Hospital (2012–2017). Testing was performed to exclude the following: autoimmune hepatitis (AIH), Wilson disease, viral hepatitis (B and C), thyroid dysfunction, celiac disease, α-1 antitrypsin deficiency, and hemochromatosis
RESULTS: A total of 900 children with overweight and obesity (63% boys, 26% Hispanic ethnicity) were referred, with a median age of 13 years (range: 2–18). Most had severe obesity (n = 666; 76%) with a median BMI z score of 2.45 (interquartile range [IQR]: 2.2–2.7). Median alanine aminotransferase level at presentation was 64 U/L (IQR: 42–95). A clinically indicated liver biopsy was performed in 358 children (40%) at a median of 6 months (IQR: 1–14) post initial visit; of those, 46% had confirmed nonalcoholic steatohepatitis. Positive autoantibodies were observed in 13% of the cohort, but none met criteria for AIH. Only 19 (2%) were found to have other causes of liver disease, with no cases of viral hepatitis or Wilson disease detected.
Specific diseases included thyroid dysfunction in 11 (1.2%), celiac disease in 3 (0.4%), A1AT deficiency in 3 (0.4%), and non-Hodgkin’s lymphoma in 1. A prior study had indicated that AIH was the second-most common etiology (Aliment Pharmacol Ther 2013; 38: 1267-77); this study indicated a much higher rate of alternative diagnosis (24%) in children undergoing a liver biopsy for suspected NAFLD (see related blogs: Screening for NAFLD and Concise Review: Fatty Liver in Pediatrics).
My take: The yield of extensive testing in children with suspected fatty liver disease is very low. I suspect that a cost-effective analysis would indicate a much more limited role for further liver evaluations.
Between February 2016 and December 2017, 2171 results were reported. Median turnaround time was 21 days.
583 pathogenic (P) variants, 79 likely pathogenic (LP) variants, and 3117 VOUS; 166 P/LP variants and 415 VOUS were novel.
The panel’s overall diagnostic yield was 12% (n = 265/2171) representing 32 genes with mutations identified (the panel tested up to 66 genes).
The top five genetic diagnoses for the group, in order: JAG1 + NOTCH2 (Alagille syndrome), ABCB11, SERPINA1, ABCB4, and POLG. (Table 3 lists all of the findings)
Other reports in the same issue describe a normal-GGT cholestasis due to USP53 deficiency
Methods: N=85. Liver stiffness measurement (LSM), by vibration-controlled transient elastography and noninvasive fibrosis scores (Firbosis-4, aspartate aminotransferase-platelet ratio index), were obtained before and 12 months after eradication with ledipasvir-sofosbuvir.
Key findings:
Overall, median baseline LSM was 5.8 (IQR, 4.2-6.5) and at follow-up 5.1 kPa (IQR, 4-6 kPa) (P = .045)
16 patients (19%) experienced regression, and 46 (54%) nonprogression of LSM
The median baseline FIB-4 and aspartate aminotransferase-platelet ratio index scores were 0.34 (IQR, 0.22-0.47) and 0.35 (0.24-0.57), and at follow-up 0.3 (IQR, 0.22-0.34) and 0.2 (0.18-2.8) (P < .001, <.001), respectively
Limitations: In Egypt, HCV genotype 4 is predominant; thus, findings could be different with other HCV genotypes. In addition, the ‘gold’ standard in assessing fibrosis remains a liver biopsy.
In many liver conditions, effective therapy has been associated with histologic improvement/regression. So, while the findings in this study are expected, it is still nice to see more evidence of this outcome.
My take: This study supports the notion that elimination of HCV is associated with either regression or non-progression of liver fibrosis. Treatment prior to extensive liver damage is likely both effective and cost-effective.
Previous studies have indicated that prolonged cholestasis before liver transplantation is associated with adverse neurodevelopmental outcomes. LH Rodijk et al (JPGN 2021; 72: 592-596. Full text: Early Motor Repertoire in Infants With Biliary Atresia: A Nationwide Prospective Cohort Study) prospectively investigate early neurologic impairment in infants with biliary atresia (n=35).
The author’s utilized Prechtl’s General Movement (GM) Assessment which is a noninvasive, cost-effective, and worldwide used method to identify infants who are at risk of neurodevelopmental impairments. This requires video recordings of 10 minutes; this was avoided in the 24 hours following liver biopsy or general anesthesia.
Key finding:
The proportion of infants with atypical GMs was significantly higher in BA (46%) than in 2 reference groups of healthy infants (vs 10%, P < 0.001; vs 18%, P < 0.001).
My take (from authors): “At the time of diagnosis, almost half of the infants with BA showed an atypical early motor repertoire, suggesting that neurological impairment is present already in early infancy. Compared to healthy infants, approximately 2 to 3 times more infants showed an atypical motor repertoire.”
Related blog posts:
Neurodevelopmental Outcomes in Biliary Atresia -same group of authors ( LH Rodijk et al) published data showing a fairly high rate of neurodevelopmental problems in children with BA (25% requiring special education)