

Category Archives: Uncategorized
PEG Placement in Cystic Fibrosis
A small retrospective study (RT Khalaf et al.NCP 2018; LINK: doi.org/10.1002/ncp.10219) showed that PEG placement was associated with a trend (not statistically significant) towards improved lung function in children with cystic fibrosis (CF). Reference from Kipp Ellsworth twitter feed. There were 20 patients who had PEG placed compared to 40 patients who did not.
Findings:
- BMI percentile increased per month for those with PEG (0.51, 95% confidence interval (CI) = −0.05–1.08, P = .08), but decreased for those without PEG (−0.03, 95% CI = −0.33–0.28, P = .86); however, the difference (0.54; 95% CI = −0.10–1.18, P = .10) was not statistically significant.
- FEV1 change with time showed a decrease for patients with PEG (−0.04; 95% CI = −0.30–0.22, P = .74) and those without PEG (−.22; 95% CI = −0.45–0.01, P = .06). Although the FEV1 decrease for those without PEG was higher than those with PEG, the difference between the groups was not statistically significant (0.18; 95% CI = −0.17–0.52, P = .32)
My take: While the differences are not statistically-significant, this study indicates that PEG placement is NOT detrimental to lung function in CF and may be beneficial.
Related blog posts:
- Why Do Canadians with Cystic Fibrosis Live Longer?
- Gastrostomy Tubes for Children with Cystic Fibrosis
- Lumacaftor-Ivacaftor for Cystic Fibrosis
- Ivacaftor for Cystic Fibrosis | gutsandgrowth
- CFTR Modulators for Cystic Fibrosis
- FDA Expands Use of Cystic Fibrosis Medication | gutsandgrowth
- “Origins of Cystic Fibrosis Lung Disease”

Near Banff

Fish Oil for Ulcerative Colitis?
A small randomized, double-blind, placebo-controlled study (E Scaioli et al. Clin Gastroenterol Hepatol 2018; 16: 1268-75) examined the use of Eicosapentaenoic acid-Free Fatty Acid Form (EPA-FFA) a component of n-3 fish oil for patients with ulcerative colitis UC).
From 2014-2016, the investigators enrolled 60 patients who had partial Mayo score <2 and fecal calprotectin >150 mcg/g who had been receiving stable therapy for at least 3 months. Then they were randomized 1:1 to receive EPA 1000 mg BID or placebo for 6 months.
Key findings:
- 19 of 30 (63%) EPA-FFA group compared with 4 of 30 (13.3%) of placebo-treated group had achieved the primary endpoint of a 100-point reduction in fecal calprotectin at 6 months. OR 12.0, P<.001
- The secondary endpoint of clinical remission was noted in 23 of 30 (77%) in the EPA-FFA group compared with 15 of 30 (50%), OR 3.29, P=.035)
- No serious adverse effects were reported.
Limitations:
- Small number of patients from a single center
- Short follow-up
- In those without clinical relapse, a followup colonoscopy was not performed
My take: In this study EPA-FFA was associated with lower calprotectin and higher rates of remaining in remission. More data are needed.
Related blog posts:
- Spice it up? Curcurmin for ulcerative colitis
- Herbal Medicines for IBD and IBS | gutsandgrowth
- The Search for a Dietary Culprit in IBD | gutsandgrowth
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.

Near Banff

How to Rectify the Problem of Missed Impactions
Blog Note: This blog site was recently upgraded such that blog followers should not see wordpress.com ads and the domain name is officially gutsandgrowth.com rather than gutsandgrowth.wordpress.com.
A recent study (S Pradhan, B Jagadisan. JPGN 2018; 67: 570-5) describes the yield of digital rectal exam (DRE) for detecting impaction in the setting of functional constipation.
Methods: In this prospective, observational study with an initial cohort of 233 (from a tertiary center) with a history of suggestive of constipation, the authors identified 169 who satisfied Rome III criteria for functional constipation. After excluding 48 who had impactions detected without DRE and another 24 who had DRE not performed (24 due to fissures, 2 due to recent enema, and 2 due to parental preference), there were 93 who had DRE.
Key finding: “Children satisfying Rome III criteria without requiring digital rectal examination …have impaction detectable only by DRE in 30.1%” (28 of 93).
My take: Since treatment is modified in those with an impaction, DRE remains important part of the examination in children with constipation or symptoms attributed to constipation.
Related posts:
- Don’t Let the Chief of Staff Review this Study on Constipation
- Stimulants for constipation
- Diagnostic tests hardly ever help patients poop
- What’s Wrong with Ordering an AXR for Constipation in the ER …
- Miralax Safety | gutsandgrowth
- Updated Pediatric Expert Constipation Guidelines | gutsandgrowth
- AGA Constipation Guidelines | gutsandgrowth
- “Simple Remedies for Constipation” | gutsandgrowth
- Reliability of colonic manometry | gutsandgrowth
- …ER Performance for Suspected Constipation | gutsandgrowth

Near Banff


Romaine Lettuce and E coli Outbreak
According to the CDC update (Nov 26, 2018) –Outbreak of E. coli Infections Linked to Romaine Lettuce: “43 people infected with the outbreak strain of E. coli O157:H7 have been reported from 12 states. A list of the states and the number of cases in each can be found on the Map of Reported Cases page.
Illnesses started on dates ranging from October 8, 2018 to October 31, 2018. Ill people range in age from 1 to 84 years, with a median age of 25. Sixty-nine percent of ill people are female. Of 38 people with information available, 16 (42%) have been hospitalized, including one person who developed hemolytic uremic syndrome, a type of kidney failure. No deaths have been reported.”
“CDC is advising that U.S. consumers not eat and retailers and restaurants not serve or sell any romaine lettuce harvested from the Central Coastal growing regions of northern and central California. If you do not know where the romaine is from, do not eat it.”
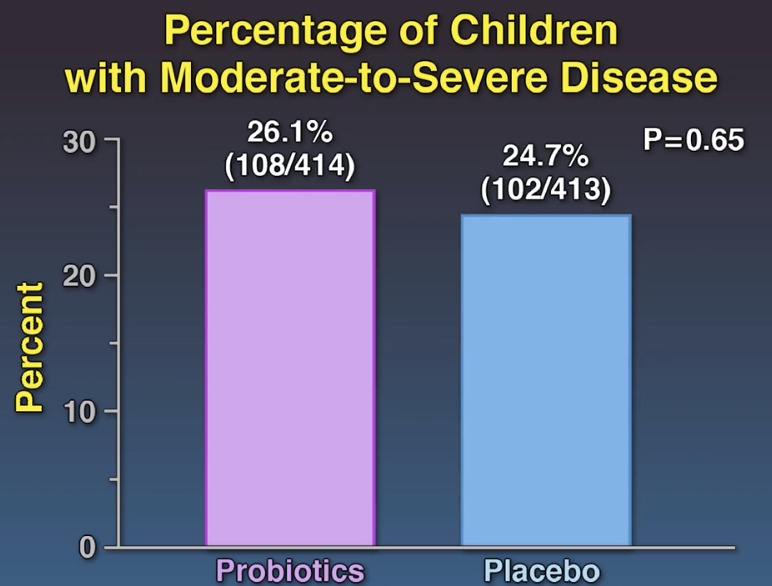
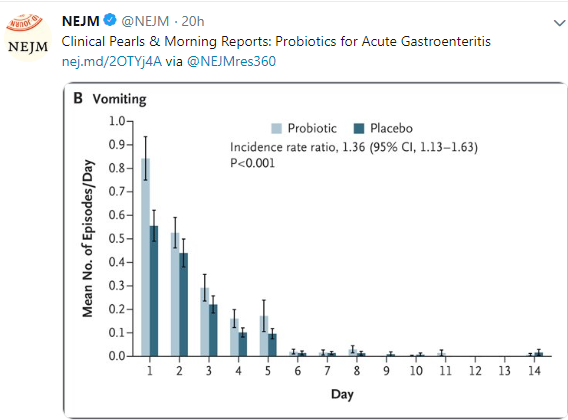
Probiotics -Lack of Efficacy for Acute Gastroenteritis (Part 2)
This blog post highlights a second study showing a lack of efficacy of probiotics for acute gastroenteritis. Link to 2 minute Summary: Quick Take on Probiotics for AGE
My take: While some probiotic strains have been shown to be helpful in some conditions (eg. antibiotic associated diarrhea), this study indicates that probiotics are likely ineffective in altering the course of acute gastroenteritis.
SB Freedman et al. N Engl J Med 2018; 379:2015-2026 Link to abstract: Multicenter Trial of a Combination Probiotic for Children with Gastroenteritis

Related blog posts:
- The Truth about Probiotics: Constipation Version
- Are Probiotics Effective in Changing the Microbiome?
- Lactobacillus rhamnosus GG Associated with Increased Necrotizing Enterocolitis in Observational Study
- How helpful are probiotics?
- Balanced summary of probiotics & Microbiome effects on brain
- Probiotics for Crohn’s Disease –No Beneficial Effects Noted | gutsandgrowth
- Probiotics For Fatty Liver Disease | gutsandgrowth
- “Low quality of evidence; strong recommendation” for Probiotics in Gastroenteritis
- Probiotics for Colic
- Do Probiotics Really Help Crying Infants? | gutsandgrowth
- Pushback on Probiotics
- One More Day Syndrome & Necrotizing Enterocolitis | gutsandgrowth
- Probiotics, Atopy, and Asthma | gutsandgrowth
One for the Probiotic Skeptics: Lack of Efficacy in Acute Gastroenteritis (Part 1)
My opinion has been that probiotics are generally over-hyped and are likely ineffective for many conditions in which they are commonly used (see related blog posts below).
A recent study (D Schnadower et al.N Engl J Med 2018; 379:2002-2014) provided more data to support this skeptical view when probiotics are utilized for acute gastroenteritis. Another study in the same issue will be highlighted tomorrow and reaches a similar conclusion.
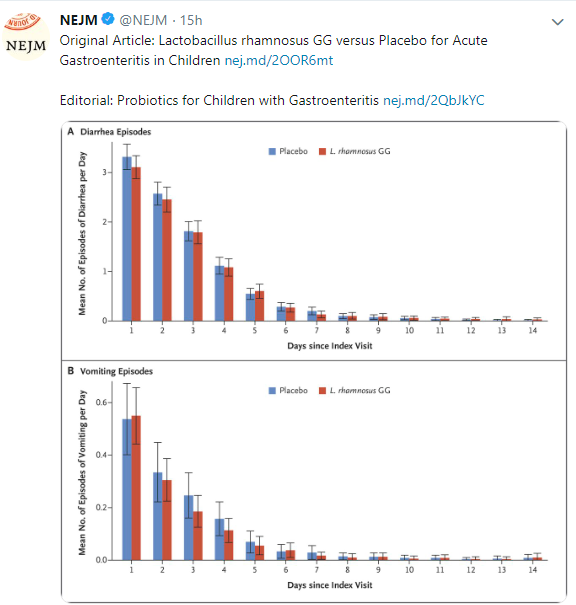
Link to Abstract: Lactobacillus rhamnosus GG versus Placebo for Acute Gastroenteritis in Children
METHODS: We conducted a prospective, randomized, double-blind trial involving children 3 months to 4 years of age with acute gastroenteritis who presented to one of 10 U.S. pediatric emergency departments. Participants received a 5-day course of Lactobacillus rhamnosus GG … twice daily or matching placebo…
RESULTS Among the 971 participants, 943 (97.1%) completed the trial…There were no significant differences between the L. rhamnosus GG group and the placebo group in the duration of diarrhea (median, 49.7 hours in the L. rhamnosus GG group and 50.9 hours in the placebo group; P=0.26), duration of vomiting (median, 0 hours in both groups; P=0.17), or day-care absenteeism (median, 2 days in both groups; P=0.67) or in the rate of household transmission (10.6% and 14.1% in the two groups, respectively; P=0.16).
CONCLUSIONS Among preschool children with acute gastroenteritis, those who received a 5-day course of L. rhamnosus GG did not have better outcomes than those who received placebo
My take: While some probiotic strains have been shown to be helpful in some conditions (eg. antibiotic-associated diarrhea), this study indicates that probiotics are likely ineffective in altering the course of acute gastroenteritis.
Related blog posts:
- The Truth about Probiotics: Constipation Version
- Are Probiotics Effective in Changing the Microbiome?
- Lactobacillus rhamnosus GG Associated with Increased Necrotizing Enterocolitis in Observational Study
- How helpful are probiotics?
- Balanced summary of probiotics & Microbiome effects on brain
- Probiotics for Crohn’s Disease –No Beneficial Effects Noted | gutsandgrowth
- Probiotics For Fatty Liver Disease | gutsandgrowth
- “Low quality of evidence; strong recommendation” for Probiotics in Gastroenteritis
- Probiotics for Colic
- Do Probiotics Really Help Crying Infants? | gutsandgrowth
- Pushback on Probiotics
- One More Day Syndrome & Necrotizing Enterocolitis | gutsandgrowth
- Probiotics, Atopy, and Asthma | gutsandgrowth
FDA IBD Workshop -Take-Home Points

From a previous blog lecture from Athos Bousvaros (NASPGHAN Postgraduate Course 2014)
Off-label does not equate to experimental
FDA Statement: The FD&C Act does not, however, limit the manner in which a physician may use an approved drug. Once a product has been approved for marketing, a physician may prescribe it for uses or in treatment regimens or patient populations that are not included in approved labeling. Such “unapproved” or, more precisely, “unlabeled” uses may be appropriate and rational in certain circumstances, and may, in fact, reflect approaches to drug therapy that have been extensively reported in medical literature.

A Bunch of Data on Vedolizumab
DE Yung et al. Inflamm Bowel Dis 2018; 24: 2327-38. This systematic review and meta-analysis of four studies “did not detect an increased risk of postoperative complications with preoperative vedolizumab” (VDZ). This study included 281 patients who received VDZ.
SC Ng et al. Inflamm Bowel Dis 2018; 24: 2431-41. The authors examined the frequency of opportunistic infection among 4 VDZ trials and postmarketing surveillance, accounting for ~114,000 patient-years of exposure. The most common infection was C difficile (0.5 per 100 patient-years); tuberculosis was reported at 0.1 per 100 patient years. This study showed “that the rate of serious opportunistic infections in patients receiving VDZ was low and most patients could continue VDZ treatment.”
SL Gold et al. Gastroenterol 2018; 155: 981-2. This clinical image showed a case of Henoch-Schonlein Purpura (HSP) that developed in a 53 year receiving VDZ.
E Shmidt et al. Inflamm Bowel Dis 2018; 24: 2461-7. This retrospective review of a prospectively maintained IBD registry provides information of risk factors for VDZ loss of response and management. 444 patients out of 788 who received VDZ had a significant response.The majority of VDZ recipients 75) had failed prior anti-TNF Rx. Key points:
- Loss of response (LOR) at 6 months and 12 months was 20% and 35% respectively
- UC patients compared to Crohn’s disease (CD) patients were more likely to have LOR with R of 1.54.
- Shortening VDZ infusion interval from q8 weeks to q4-6 weeks recaptured response in 49% and led to remission in 18% of this cohort.
- LOR was more common (2-fold) among those who had a LOR to anti-TNF agent. Patients with primary nonresponse were less likely to have LOR with VDZ.
U Kopylov et al. Inflamm Bowel Dis 2018; 24: 2442-51. This retrospective multicenter study examined VDZ effectiveness among anti-TNF naive patients, n=184.
- For CD, 42/50 (82%) responded by week 14, and 32 (64%) were in clnical remission. At last followup (30-52 weeks), clinical remission was noted in 24/35 (69%)
- For UC, 116/134 (79%) responded at week 14 and 53 (40%) were in clinical remission. At last followup (30-52 weeks), 67% were in remission (69/103)
The authors conclude that VDZ is similarly efffective for anti-TNF naive CD and UC patients.
My take: These studies show that we still have a lot to learn about the effectiveness of VDZ as its use becomes more widespread.
Related blog posts:
- Vedolizumab and Extraintestinal Manifestations
- VICTORY consortium showing good results for vedolizumab
- Summary of latest information on Vedolizumab
- GI Care for Kids Data on Vedolizumab 2017
- Latest on Vedolizumab
- Pediatric Experience with Vedolizumab | gutsandgrowth
- Vedolizumab -another new IBD treatment | gutsandgrowth

Jasper, Canada
Increased Risk of Eosinophilic Esophagitis in Esophageal Atresia Patients
Briefly noted: U Krishnan et al. Analysis of eosinophilic esophagitis in children with repaired congenital esophageal atresia. JACI 2018. Published online Oct 24, 2018.
This retrospective, single-center study examined 4 eosinophilic esophagitis (EoE) study cohorts and identified EoE in 20 of 110 patients (18%) who had surgically-repaired esophageal atresia.
This association has been seen previously: World J Gastroenterol. 2014 Dec 21; 20(47): 18038–18043. This case study stated ” We are suggesting that EoE is a frequent concomitant problem in patients with history of congenital esophageal deformities, and for this reason any of these patients with refractory reflux symptoms or dysphagia (with or without anastomotic stricture) may benefit from an endoscopic evaluation with biopsies to rule out EoE.”

Related blog posts:
