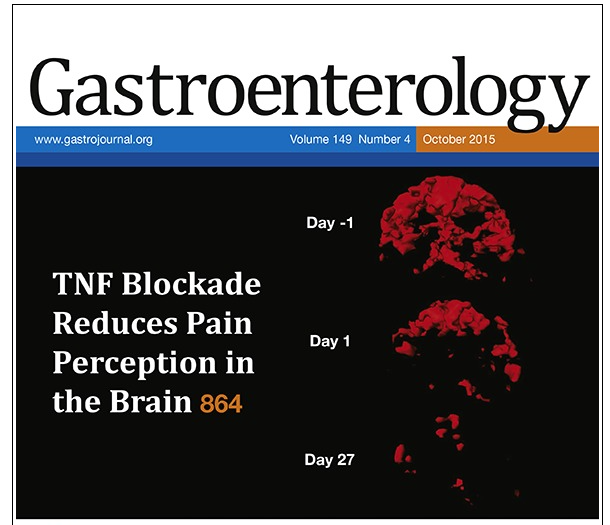
A pretty cool use of technology provides strong evidence that decreased pain perception in the brain of patient’s with Crohn’s disease (CD) occurs well before anti-inflammatory effects like mucosal healing (A Hess et al. Gastroenterol 2015; 149: 864-66). In this study, the authors prospectively identified 4 patients with CD and performed functional MRI on day -1, day 1, and day 27. Key findings:
- In three patients, who responded with a decrease in Harvey-Bradshaw Index by ≥2 points 14 weeks after anti-TNF initiation, the pain signal induced by either finger tapping or compression (see cover below) was markedly improved 1 day after anti-TNF initiation.
- In the CD non responder, there was only slight reduction in signals at 24 hours and no improvement from baseline at day 27.
My take: This study explains why so many patients with severe symptoms can be managed quickly as outpatients. The effects of anti-TNF therapy on pain occur within 24 hrs! Pretty cool.