Methods: Here we characterize the trajectory by which the gut microbiome recovers its taxonomic and functional profile after antibiotic treatment in mice on regular chow (RC) or Western Diet (WD).
Key findings: “Only mice on RC undergo a rapid successional process of recovery. Metabolic modelling indicates that a RC diet promotes the development of syntrophic cross-feeding interactions, whereas in mice on WD, a dominant taxon monopolizes readily available resources without releasing syntrophic byproducts. Intervention experiments reveal that an appropriate dietary resource environment is both necessary and sufficient for rapid and robust microbiome recovery, whereas microbial transplant is neither.”
Conclusion (from authors): “Our data challenge widespread enthusiasm for faecal microbiota transplant (FMT) as a strategy to address dysbiosis, and demonstrate that specific dietary interventions are, at a minimum, an essential prerequisite for effective FMT, and may afford a safer, more natural and less invasive alternative.”
My take: This study suggests that the best way to get a “healthy” microbiome is to eat a healthy diet rather than to try to alter with FMT. This finding likely would be the same for probiotics as well.
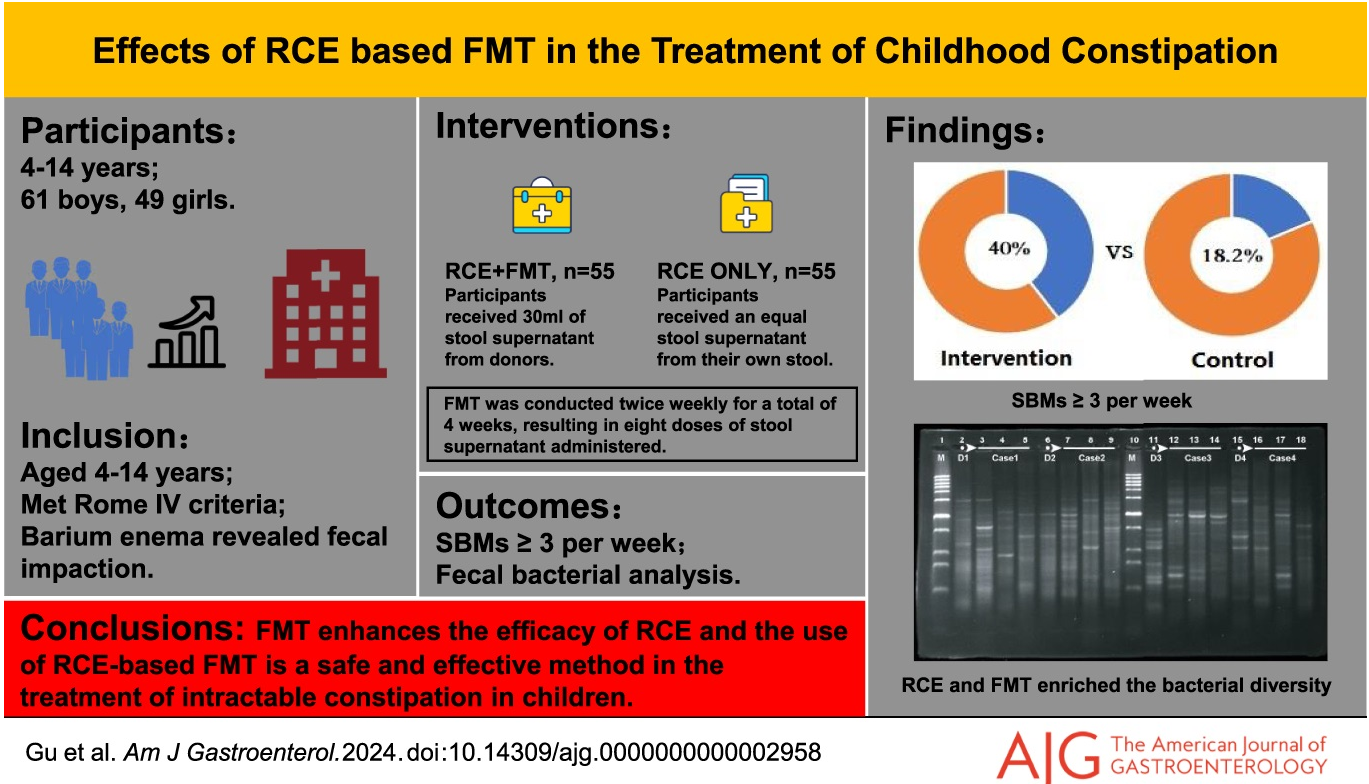
Methods: The efficacy of retrograde colonic enema (RCE) with fecal microbiota transplantation (FMT) was studied in a randomized, double-blind, controlled trial with 110 children. The initial cohort recruited was 576 patients; however, 466 were excluded for not meeting inclusion criteria. All participants received a daily RCE, followed by a 4-week FMT treatment (twice a week) and a 12-week follow-up period.
Key findings:
At the end of the follow-up period, 22 patients (40.0%) in the FMT with RCE group and 10 patients (18.2%) in the placebo with RCE group had ≥ 3 spontaneous bowel movements per week
There was a low response to RCE alone which the authors attributed in part to the severity of constipation in the cohort. It is unclear the degree of compliance with the treatment protocol which was done in the home setting. There was a prior open-label study with NJ FMT which improved constipation in half of participants.
My take: Modulating the microbiome can have beneficial effects on stool frequency. This can be through diet and possibly FMT in severe cases of constipation. The availability of capsules could make this type of therapy easier but perhaps less palatable. Even if FMT proves to be a useful treatment, the optimal treatment regimen is not clear.
On September 29, 2024, OpenBiome will voluntarily suspend the distribution of investigational Fecal Microbiota Transplants (FMT) for patients with recurrent Clostridioides difficile infection (C. diff)...
Recent interaction with the FDA has informed our decision to voluntarily suspend the distribution of all investigational FMT as we continue to seek clear direction on aligning our operations with the final Enforcement Policy published in 2022. Our commitment has always been to adhere to FDA regulations and guidelines for the manufacture and distribution of investigational FMT as a therapeutic option for patients with C. diff. Thus, this is not a safety or quality matter. Investigational FMT preparations provided by OpenBiome are manufactured and distributed in compliance with current good manufacturing practices (cGMP).
We continue to hear from clinicians, our frontline partners, that despite the availability of FDA-approved therapeutics, there remain patients who do not respond to these treatments and, according to clinical guidelines, should have access to traditional FMT. ..
Contact us. If you have a patient suffering from severe or fulminant C. diff, please contact us at 617-575-2201 or info@openbiome.org to discuss options.
Share your thoughts. We believe the FDA would benefit greatly from hearing directly from survivors and their advocates about the urgent need for continued access to rigorously screened and tested FMT. If you or your C. diff patients are willing, please submit comments to ocod@fda.hhs.gov with a copy to Dr. David Kaslow, director Office of Vaccines Research and Review, at david.kaslow@fda.hhs.gov, and Dr. Peter Marks, director of the Center for Biologics Research and Evaluation at peter.marks@fda.hhs.gov. Or you may share your experiences with us directly using this FORM.
My take: As FDA-approved therapeutics have not received a pediatric indication, NASPGHAN involvement to try to keep FMT available for children would be a worthwhile endeavor. In the absence of having FMT available from OpenBiome, NASPGHAN experts could provide guidance on best practices for refractory C diff.
In the first study by Chehade et al, the authors analyzed six RCTs involving 324 patients. Key findings:
Compared with placebo, FMT has significant benefit in inducing combined clinical and endoscopic remission (odds ratio, 4.11; 95% confidence interval, 2.19-7.72; P < .0001)
clinical remission with FMT was 46.2% compared 22.5% for placebo
clinical response with FMT was 51.6% compared to 30.1% for placebo
endoscopic remission with FMT was 18.9% compared to 6.1% for placebo
endoscopic response with FMT was 36.7% compared to 22.4% for placebo
Discussion Points:
“The studies included in our article indicate that there is a shift in the microbiota composition of responders in the FMT group to resemble the profile of healthy donors”
FMT delivery via upper GI tract was equally effective as delivery via lower GI tract in these studies in inducing combined remission
“The understanding of FMT effectiveness for IBD is in its infancy.”
In the case report by Alomomen et al, a 34 year old with refractory ulcerative colitis and PSC (post-transplant) had not responded to infliximab, vedolizumab, adalimumab, tofacitinib or 10 months of ustekinumab (every 4 weeks). In addition, he was receiving tacrolimus therapy due to his liver transplant. His colonoscopy demonstrated a continuous Mayo 3 colitis. Subsequently, vancomycin therapy was added to his treatment (500 mg BID); he continued ustekimumab. Six months afterwards, his fecal calprotectin had dropped to 277 from 1600 and his CRP and hemoglobin had normalized. Repeat colonoscopy demonstrated complete endoscopic healing.
My take: There are many patients who do not respond to current IBD therapies. These two studies show that both FMT and vancomycin could be useful in selected patients.
Lego Art at Tucson Botanical GardensLego LionLego Panther
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
In this multicenter retrospective cohort (n=42), the authors examined the efficacy and safety of fecal microbiota transplantation (FMT) in immunocompromised (IC) children with Clostridioides difficile infection (CDI). Etiology of IC included: solid organ transplantation (18, 43%), malignancy (12, 28%), primary immunodeficiency (10, 24%), or other chronic conditions (2, 5%)
Key findings:
23 (55%) of FMT was delivered via colonoscopy, 17 (40%) were delivered via enteric tube, and 2 (5%) via capsule
Success rate was 79% after first FMT and 86% after 1 or more FMT.
There were serious adverse events (SAEs) in 13 out of 42 (31%) patients; 4 (9.5%) of which were likely treatment-related (all patients recovered). These events included cecal perforation, aspiration pneumonitis, diarrhea and fever. Given retrospective design of study, AEs were likely underreported
My take: Though there are the potential for significant adverse effects, FMT is effective in a high percentage of immunocompromised children with CDI.
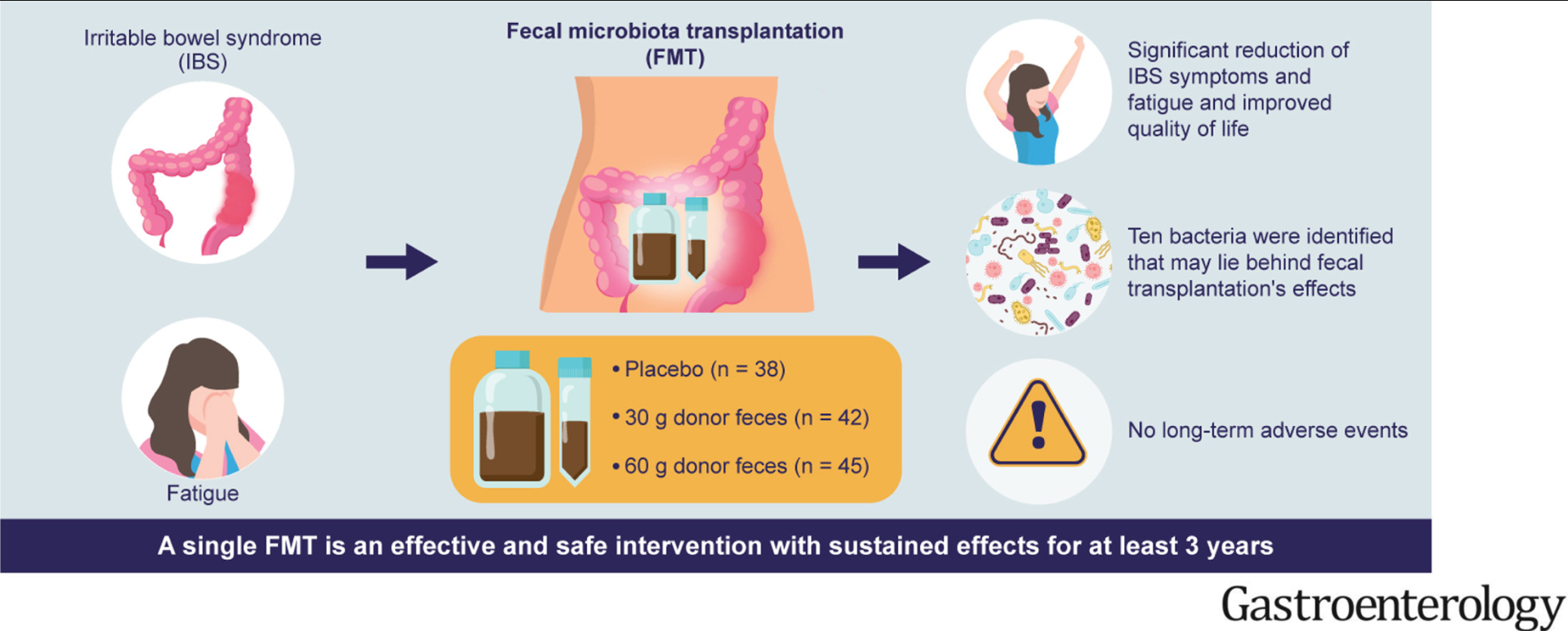
Background: “Fecal microbiota transplantation (FMT) might be a promising treatment for IBS, and this has been investigated in 7 randomized controlled trials (RCTs). 2 In 4 of these, FMT reduced symptoms and improved the quality of life of patients with IBS, whereas no effects were indicated in the other 3. 2 The difference in these results was likely because of differences in the protocols used, the selected donors, the cohort of treated patients, the fecal transplant dose, and the route by which the transplant was administrated.2“
Methods: In this placebo-controlled trial with 125 patients, fecal microbiota transplantation (FMT) was administered into duodenum (30 g or 60 g). The donor was a healthy male aged 36 years with a normal body mass index who was born via vaginal delivery, breastfed, a nonsmoker, was not taking any medication, was only treated a few times with antibiotics, exercised regularly, and consumed a sport-specific diet that was richer in protein, fiber, minerals, and vitamins than the average diet.
Key findings:
Response rates were 26.3%, 69.1%, and 77.8% in the placebo, 30-g, and 60-g groups, respectively, at 2 years after FMT, and 27.0%, 64.9%, and 71.8%, respectively, at 3 years after FMT.
Fluorescent signals of 10 bacteria had significant correlations with IBS symptoms and fatigue after FMT in the 30-g and 60-g groups.
No long-term adverse events were recorded. The authors note in the discussion rare serious safety issues with FMT but indicate in this population without systemic diseases or immune deficiency, that adverse effects were mild and self-limited gastrointestinal symptoms
The editorial suggests that overall response is modest bust similar to FDA-approved medications for IBS. The number needed to treat (NNT) would be 4-5 patients to reduce the proportion with severe IBS-SSS based on per-protocol analysis (most IBS medications range from 6 to 10).
My take: This study strengthens the notion that alterations in our microbiome can the outcomes of patients suffering from IBS. Now, we have to identify which patients will benefit from this approach and how to optimally modify the microbiome. In addition, this study suggests that finding an optimal FMT donor will impact results given variability in prior trials.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
This good update provides a lot of useful information regarding fecal microbiota transplantation (FMT) and a word of caution regarding its future availability.
Key pointsregarding FMT:
Long-term safety remains unknown. FMT may lead to susceptibility to chronic inflammatory, allergic, and autoimmune diseases. “FMT has been associated with durable transmission of pro-carcinogenic bacteria from adult donors to pediatric recipients…although the long-term consequences…are unknown.”
Due to transfer of extended spectrum beta-lactamase (ESBL) E coli to 2 immunocompromised adult recipients, further screening of FMT was implemented.
Though there is no published evidence of SARS-CoV-2 fecal transmission, the FDA “advised additional precautions and testing in March 2020; “however, there are no molecular tests with stool…which have received emergency use authorization.” Hence, most FMT programs were on hold as of January 2021.
After 2021, OpenBiome, whose product was recently available again, is expected to stop distribution of FMT donor product due to increased costs of screening and the “promising biotherapeutics” that are in phase III trials.
Biotherapeutic is “loosely defined as drug therapy products where the active substance is extracted from a biological specimen.” The new products are likely to have “increased standardization, safety and practicality.”
The problem in pediatrics: none of these biotherapeutic products have started trials in children. This will lead to treatment problems. Even if one wanted to set up donor-directed FMT, it will be difficult to complete all of the screening recommended by the FDA. It could lead to self-administration by families with uncertain risks.
My take: My first reaction to this article: ‘Oh crap!’ It is sad and ironic that I will miss having available commercial stool for FMT.
In this prospective study (2012-2018) with 609 patients (median age 56 years), the authors studied long-term outcomes. Key findings:
At 1 year, 9.5% reported additional CDI episodes. Diarrhea occured in more than half of all patients, although it lasted for than a week in most patients.
Among 477 with long-term data, 188 patients post-FMT developed new medical conditions/symptoms.
Weight gain was reported by 46 patients (10.3%) post-FMT. In these patients, the median weight gained was 30 pounds (range, 10–70). Of these patients, 11 (23%) had preexisting obesity.
Approximately 3% of patients each reported new-onset diabetes mellitus and dyslipidemia, whereas 2.3% reported thyroid disease.
Gastrointestinal symptoms were the second most frequently reported (13.4%). New-onset IBS was reported by 4%, IBD by 0.3%, chronic diarrhea by 5.0%, and chronic constipation by 1.6% of patients.
Serious infections were reported by 11.8% of patients: CDI in 5.7%, Pneumonia in 4.5%, UTI in 1.8% and Sepsis in 1.2%. Median time to the infections was 29 months (range, 0–73) following FMT; only 1 patient reported an infection (CDI) within the first month after FMT.
No deaths were considered related to FMT
Limitation: no control group
My take (borrowed from authors): “FMT appears safe and effective, both in the short-term and long-term. Several new medical conditions were reported post-FMT, in particular, weight gain and IBS.”
In The Shawshank Redemption, Andy Dufresne (Tim Robbins) manages to escape prison by crawling through 500 yards of a filthy sewage pipe. It seems like a similar effort will be needed to find out how to benefit from fecal transplantation when given for problems like irritable bowel syndrome and metabolic disease/obesity. Some recent studies and associated editorials are noted below.
Key finding: At week 12, 56% of patients given donor stool reported improvement in both primary endpoints compared with 26% of patients given placebo (P = .03).
This editorial stresses that trials of FMT in IBS have had inconsistent results and risks are unclear. “How many clinicians inform patients receiving FMT that the donor microbiota might include components that increase (or decrease) one’s risk of colorectal cancer?” Part of the problem is “due, in part, because a normal microbiome has not been defined.”
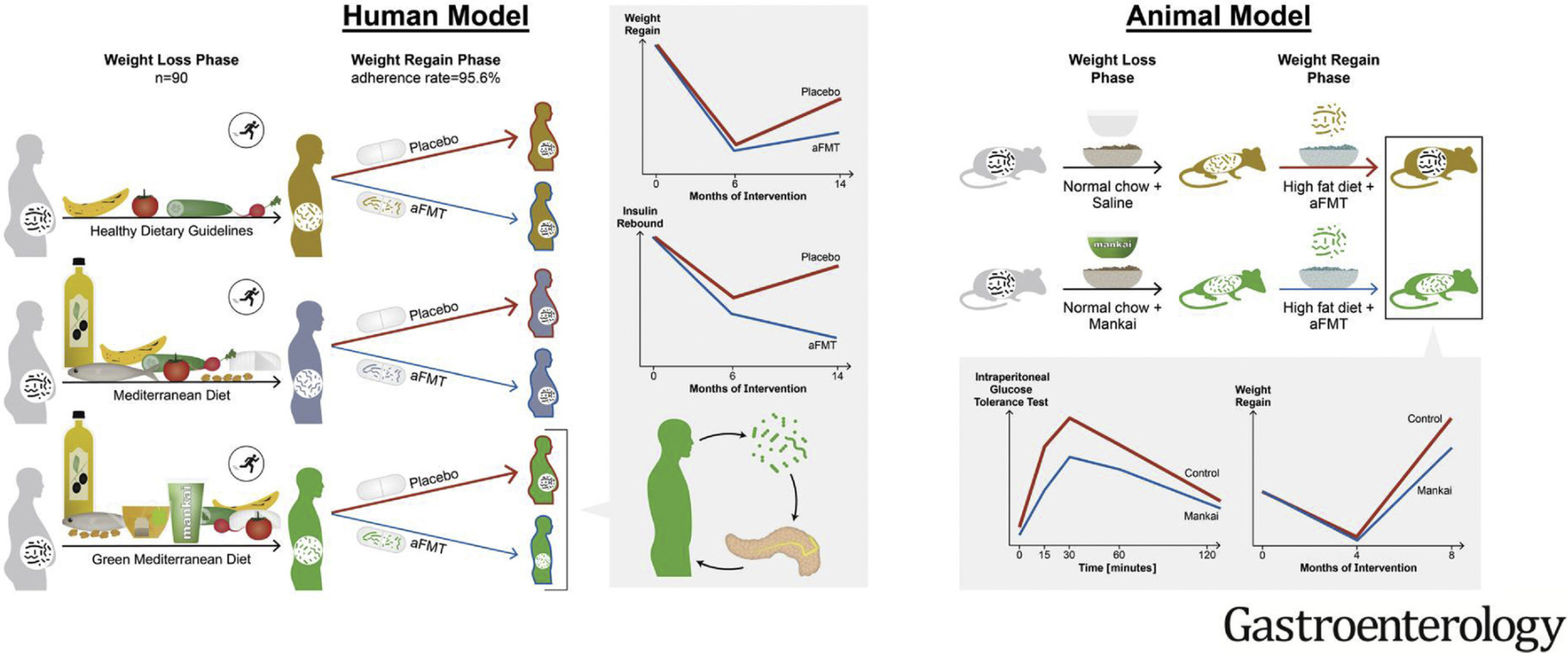
In this randomized controlled trial with 90 participants, autologous FMT (aFMT) significantly attenuated weight regain in the green-Mediterranean group (aFMT, 17.1%, vs placebo, 50%; P = .02) and improved insulin resistance: insulin rebound (aFMT, –1.46 ± 3.6 μIU/mL vs placebo, 1.64 ± 4.7 μIU/mL; P = .04) (Graphical abstract below)
In mice, Mankai-modulated aFMT in the weight-loss phase compared with control diet aFMT, significantly prevented weight regain and resulted in better glucose tolerance during a high-fat diet–induced regain phase (all, P < .05).
“These findings add support to the current body of evidence that the gut microbiota have a role in weight gain and metabolism. However, many questions remain. Indeed, although studies have shown varying degrees of effectiveness of FMT in the improvement of metabolic parameters in human participants, there has been no evidence yet that FMT can induce weight loss in obese patients.”
“The finding that maintenance of weight loss was only seen in the one dietary group consuming the Mediterranean diet plus green tea and Mankai supplement who received autologous FMT, would suggest that specific microbial profiles may be involved and that weight loss per se may not result in the required microbial profiles.”
Figure 1 from editorial: Challenges associated with the use of fecal microbial transplantation (FMT) as treatment
My take: Both of these studies show that modulation of the fecal microbiome may be helpful under the right set of circumstances to help with both irritable bowel syndrome and metabolic syndrome. However, ‘hundreds of yards’ of more research is needed to determine if this is really feasible and to assure that the benefits outweigh the potential risks.
Methods: Single course of oral encapsulated fecal microbiome from 4 healthy lean donors or saline placebo.
Key findings:
In this randomized, double-masked, placebo-controlled trial of 87 adolescents with obesity, FMT alone did not lead to weight loss at 6 weeks.
There were no observed effects on insulin sensitivity, liver function, lipid profile, inflammatory markers, blood pressure, total body fat percentage, gut health, and health-related quality of life
In post-hoc exploratory analyses among participants with metabolic syndrome at baseline, FMT led to greater resolution of this condition (18 to 4) compared with placebo (13 to 10) by 26 weeks (adjusted odds ratio, 0.06; 95% CI, 0.01-0.45; P = .007)