S Saha et al. Gastroenterol 2021; 160: 1961-1969. Full text PDF: Long-term Safety of Fecal Microbiota Transplantation for Recurrent Clostridioides difficile Infection
In this prospective study (2012-2018) with 609 patients (median age 56 years), the authors studied long-term outcomes. Key findings:
- At 1 year, 9.5% reported additional CDI episodes. Diarrhea occured in more than half of all patients, although it lasted for than a week in most patients.
- Among 477 with long-term data, 188 patients post-FMT developed new medical conditions/symptoms.
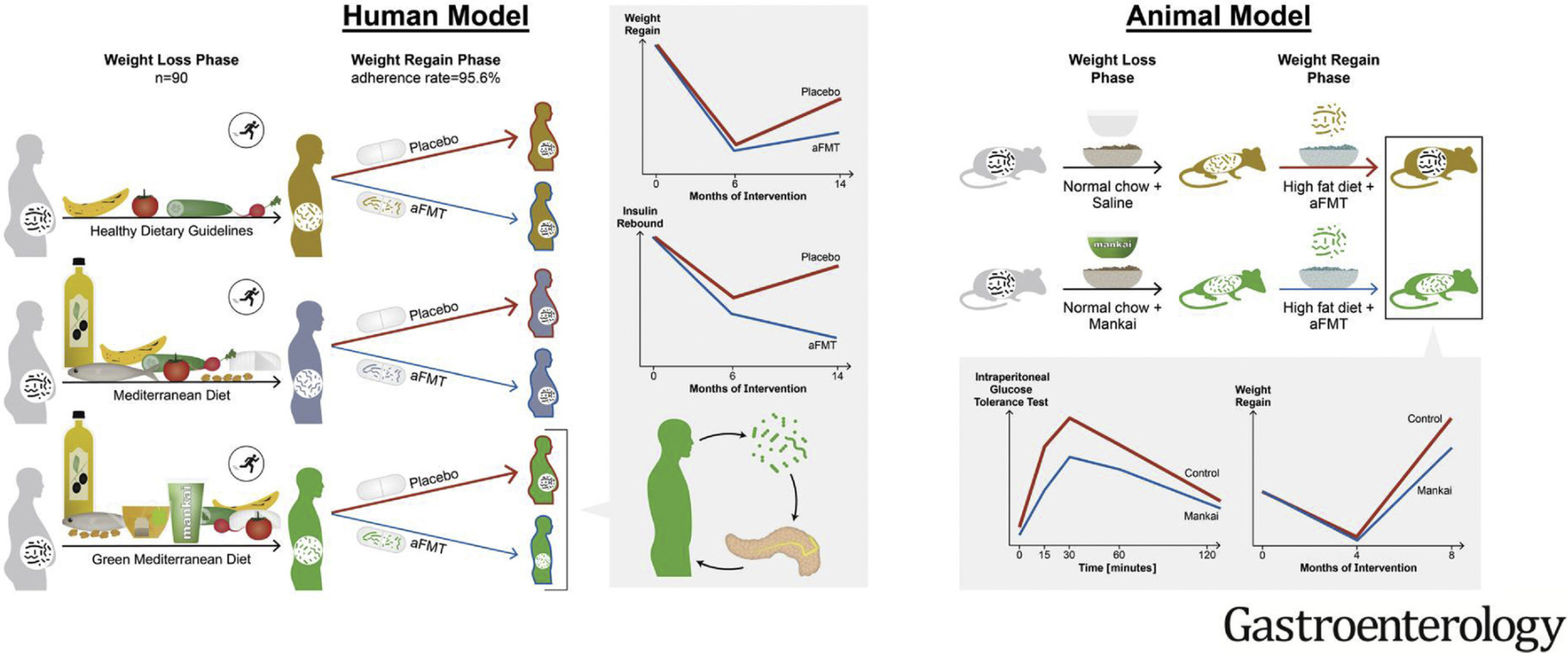
- Weight gain was reported by 46 patients (10.3%) post-FMT. In these patients, the median weight gained was 30 pounds (range, 10–70). Of these patients, 11 (23%) had
preexisting obesity. - Approximately 3% of patients each reported new-onset diabetes mellitus and dyslipidemia,
whereas 2.3% reported thyroid disease. - Gastrointestinal symptoms were the second most frequently reported (13.4%). New-onset IBS was reported by 4%, IBD by 0.3%, chronic diarrhea by 5.0%, and chronic constipation by 1.6% of patients.
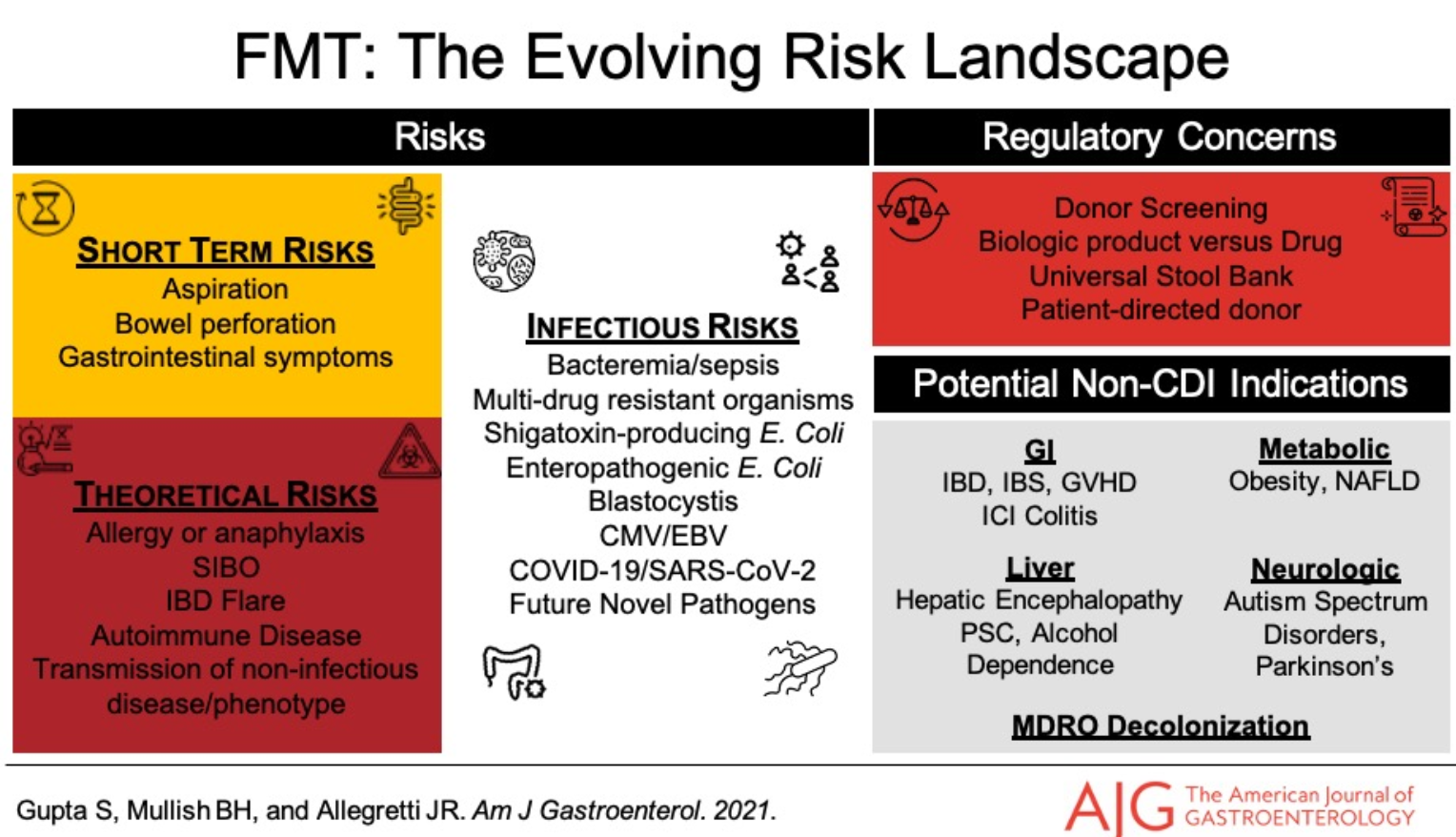
- Serious infections were reported by 11.8% of patients: CDI in 5.7%, Pneumonia in 4.5%, UTI in 1.8% and Sepsis in 1.2%. Median time to the infections was 29 months (range, 0–73) following FMT; only 1 patient reported an infection (CDI) within the first month after FMT.
- No deaths were considered related to FMT
- Limitation: no control group
My take (borrowed from authors): “FMT appears safe and effective, both in the
short-term and long-term. Several new medical conditions were reported post-FMT, in particular, weight gain and IBS.”
Related blog posts:
- Real-world Efficacy for FMT
- Large Study Show FMT Efficacy/Safety in Children (n=335)
- Clostridium difficile/Fecal Microbiota Transplantation Video
- Fecal Microbial Transplantation -Evidence for Use Beyond Recurrent Clostridium Difficile | gutsandgrowth
- Effects of FMT on Adolescents with Obesity
- How Much Do We Really Know About Fecal Microbiota Transplantation? | gutsandgrowth
- FMT Research and the Shawshank Redemption