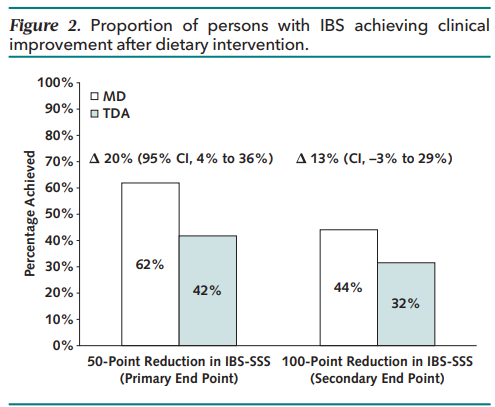
Methods: Randomized noninferiority clinical trial (n=139 Adults from UK) — 6 weeks of the MD (Mediterranean diet) (n = 68) versus TDA (traditional diet advice) (n = 71). Primary end point was the proportion achieving clinical response, defined as 50-point or greater reduction in IBS Symptom Severity Scale (IBS-SSS).
Traditional dietary advice’s main elements are to “adopt sensible eating habits and avoid excess fatty foods, spicy foods, processed foods, caffeine, fizzy drinks, and alcohol. The principal components of the MD are a diet rich in fruit, vegetables, pulses (aka legumes), whole grains, nuts, fish, and olive oil.”
Key findings:
The primary end point was met by 62% following a MD versus 42% following TDA (P = 0.017)
There was a greater reduction in the mean IBS-SSS after a MD than TDA (−101.2 vs. −64.5)
My take: I agree with the authors: The Mediterranean diet “represents a viable first-line dietary intervention for IBS.”
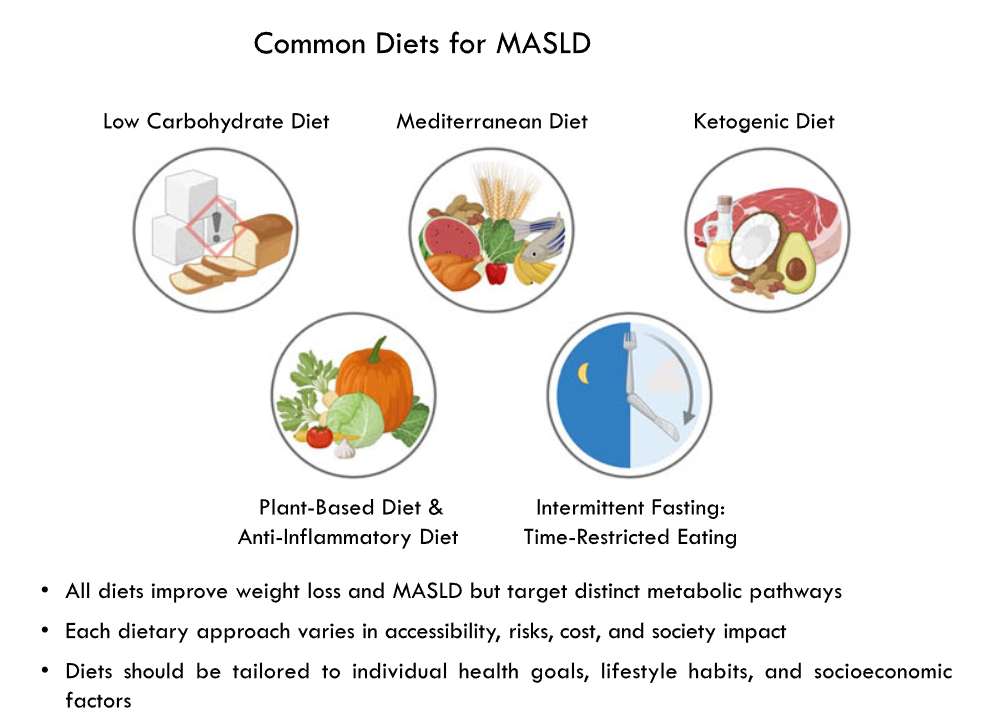
This invited commentary reviews the data for several diets that may improve weight loss and metabolic dysfunction-associated steatotic liver disease (MSALD).
Several points:
“Extremely restricted plant‐based diets may have deficiencies of vitamin D, calcium, and vitamin B12 which are nutrients found in animal products, and can be minimized by vitamin supplementation or increasing consumption of fish, mushrooms, egg yolk, cod liver oil, salmon, herring, and sole fish. VitaminB12 supplementation is recommended in plant‐based diets because this vitamin is primarily found in animal products”
Table 1 compares the structure of these diets and their advantages/drawbacks
“Low to moderate weight loss can be seen in the anti-inflammatory diet, plant-based diets, or Mediterranean diet. These diets are nutritionally complete. However, restrictive plant-based diet carries a risk of micronutrient deficiencies, which can be corrected with appropriate supplementation. These diets are effective in treating MASLD independent of weight loss due to their anti-inflammatory profile.”
“The ketogenic diet, certain carbohydrate-restricted diets, and intermittent fasting can lead to more weight loss but carry a higher risk of malnutrition. Children on these diets must be followed by nutritionists.”
My take: Each of the diets reviewed can help MASLD and obesity. Most patients pursuing dietary therapy would benefit from working with a nutritionist.
Related news: TEVA Press release, August 28, 2025: Generic liraglutide (need for daily injections) is now available.
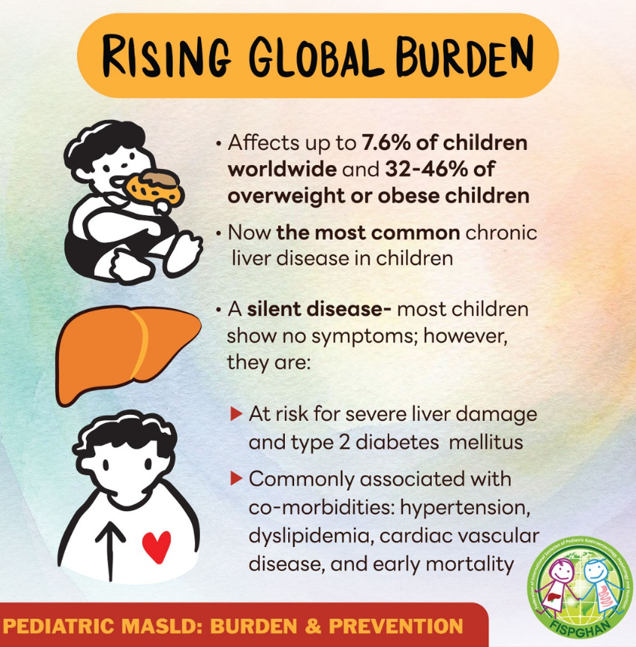
Also, related patient advice from Federation of International Societies for Pediatric Gastroenterology, Hepatology, and Nutrition (FISPGAN) –outlines risk factors and prevention tips for metabolic dysfunction-associated steatotic liver disease (MASLD):
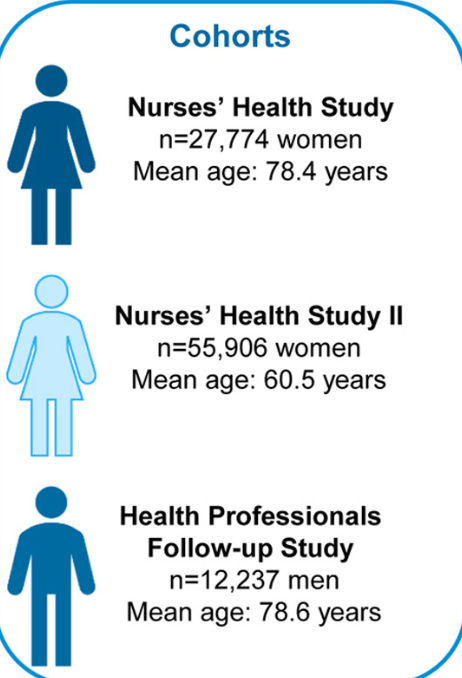
Methods: In three large cohorts, the Nurses’ Health Study (NHS), NHSII, and the Health Professional Follow-up Study (HPFS) (combined >95,000 participants), the authors identified chronic constipation based on repeatedly-measured self-reported constipation symptoms for ≥12 weeks in the past year.
Key Findings:
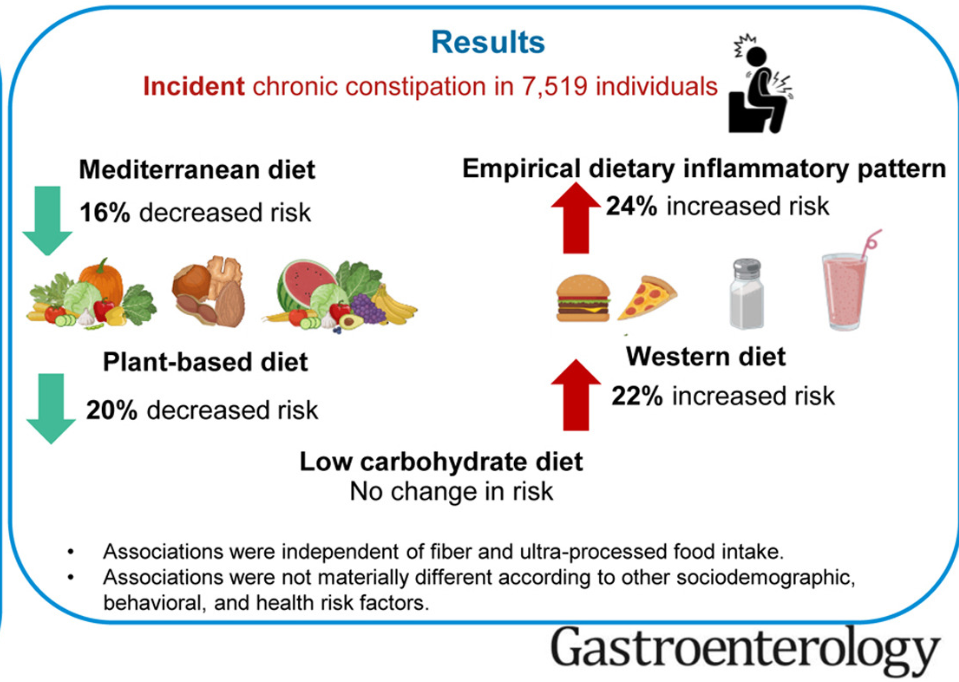
The top quintiles of alternate Mediterranean diet (aMED) and plant-based dietary index (PDI) were associated with 16% (9-22%) and 20% (14-27%) reduced risk for constipation. Vegetable and nut intake, which are enriched in aMED and PDI, were associated with decreased constipation risks.
A Western diet in the top quintile was associated with a 22% (11-33%) increased risk for constipation
My take: The results from this study are not surprising, but nice to see more data on the effects of diet on constipation. While this data focused on adults, it is clear that dietary patterns have a big role in the frequency of constipation in children too.
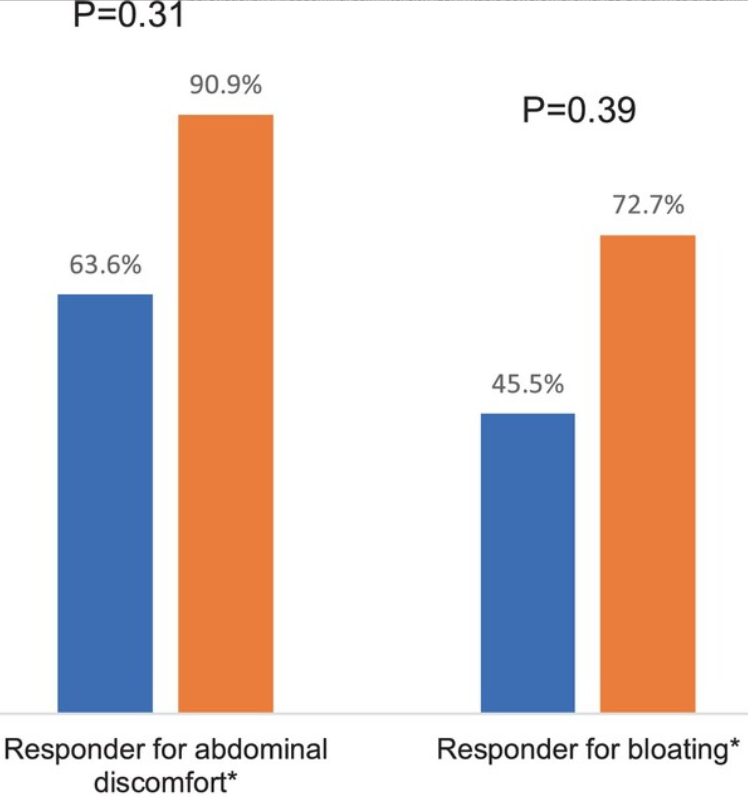
Methods: Patients were randomized controlled trial (RCT), adult patients with diarrhea-predominant IBS (IBS-D) or mixed bowel pattern (IBS-M) were randomized to Mediterranean diet (MD) versus a diet low in fermentable oligo-, di-, monosaccharides, and polyols (LFD) for 4 weeks. 10 patients completed the study in each group. The primary endpoint was the proportion of patients with ≥ 30% decrease in abdominal pain intensity (API) for ≥ 2/4 weeks. Daily variables included abdominal pain intensity (API) and bloating, while IBS symptom severity score (IBS-SSS) and IBS adequate relief (IBS-AR) were scored weekly
Key findings:
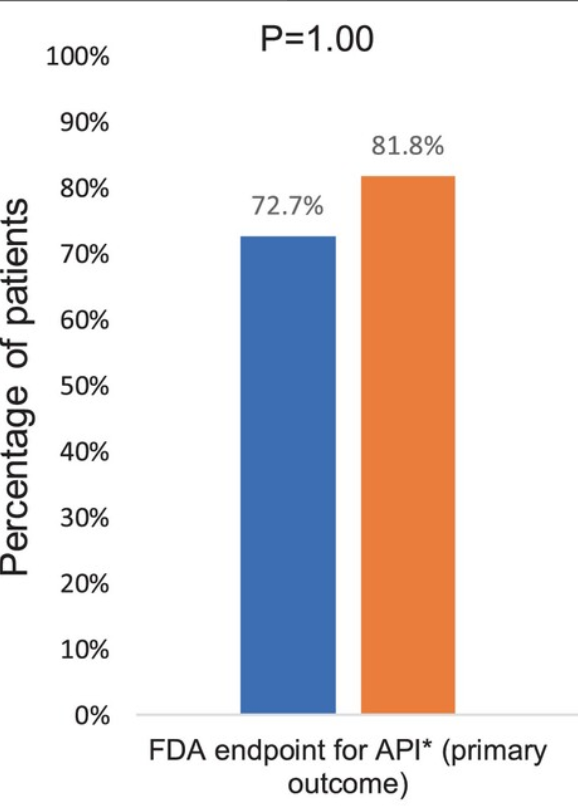
73% percent of the MD group met the primary endpoint compared to 81.8% of the LFD group (p = 1.0)
Although not statistically significant, a numerically higher proportion of the LFD group reported adequate relief and met the responder endpoint for IBS-SSS (50-point reduction) compared to the MD group (54.6% vs. 27.3% for IBS-AR and 81.8% vs. 45.5% for IBS-SSS, p = 0.39 and 0.18, respectively)
The LFD group also had a significantly greater reduction in IBS-SSS score over the 4-week treatment period compared to the MD group (−105.5 vs. −60, p = 0.02)
My take (borrowed from authors): A Mediterannean diet “improves abdominal symptoms in the majority of patients with IBS-D and IBS-M. Larger, adequately powered, real-world studies comparing the efficacy of a MD with LFD and NICE diet are needed to validate these preliminary findings and to help patients and providers to know if a MD should be added to the list of effective, evidence-based diet interventions for patients with IBS.”
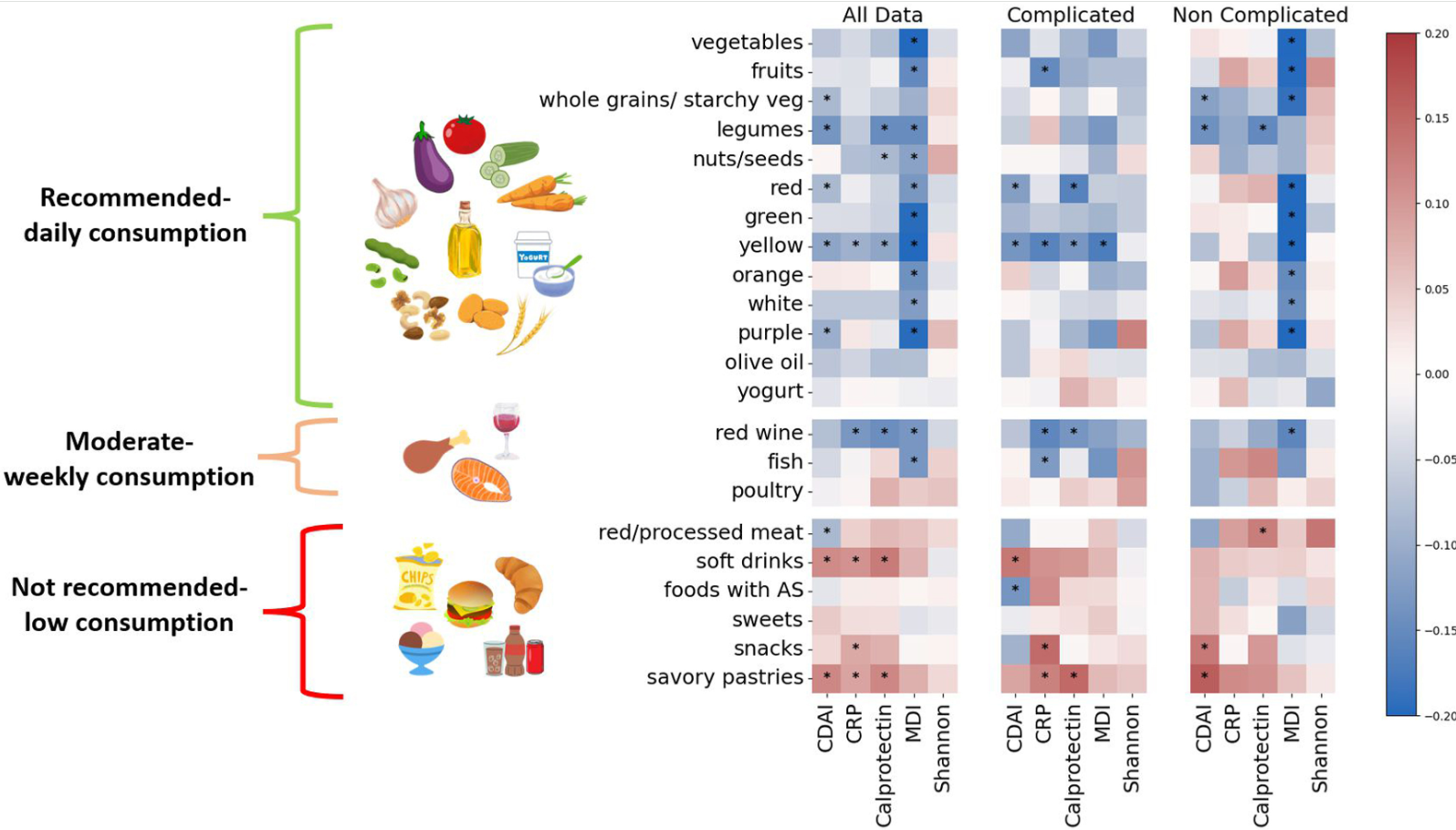
Methods: In this prospective cohort study, consecutive adults (n=271) from 2 large IBD centers in Israel with newly diagnosed CD were recruited and followed prospectively. MED adherence was assessed by repeated food frequency questionnaires (FFQs) using a predefined inflammatory bowel disease Mediterranean diet score (IBDMED score), alongside validated MED adherence screeners. Crohn’s disease activity index (CDAI), C-reactive protein, fecal calprotectin, and microbial composition (16S-ribosomal RNA sequencing) were assessed each visit. Baseline serum and fecal samples were analyzed for targeted quantitative metabolomics.
Demographic/Clinical data indicate 68% received biologics and 40% receiving immunomodulators. 32% received 5-ASA medications (despite lack of proven efficacy)
Key findings:
Adherence to MED was associated with a noncomplicated CD course, and inversely correlated with CDAI, fecal calprotectin, C-reactive protein, and microbial dysbiosis index (all P < .05)
Increasing adherence to MED over time correlated with reduced CDAI and inflammatory markers (P < .05)
Adherence to MED correlated with a beneficial microbial cluster of commensals and short-chain fatty acid producers including Faecalibacterium, and with plant metabolites, vitamin derivatives, and amino acids
Adherence to MED in the cohort group was comparable to the general non-IBD population in Israel
Limitations: This was an observational study rather than an interventional study with a control group. Thus, the results could be influenced by reverse causality
In the associated commentary by Abreu et al, it is noted that in Israel, “MED is more commonplace than in the US and other Western countries…Godny et al found that IBD patients had an average MED adherence score of 7.8, which is similar to that of the general non-IBD population in Israel; in contrast, the average MED adherence score in the US is 4–5.Godny et al’s CD patients consumed an average of 21 g of fiber per day; in a study we just completed, American CD patients consumed less than half that amount.13 Indeed, the baseline diets of American IBD patients are characterized by high amounts of saturated animal fat and almost no fresh fruits and vegetables…Another difference between the Israeli population and the typical American population is body mass index (BMI). The average BMI of patients in this study was 21.9 kg/m2 (interquartile range 20–25.3 kg/m2). This contrasts with the average BMI of the general US population of 30 kg/m2.”
My take: This study shows an association between MED diet and better outcomes/less complications in adults with Crohn’s disease. Eating a good diet is an important part of treatment.
Additional notes on dietary scores: “The IBDMED screener positively scored high consumption of MED-recommended dietary components such as fruits, vegetables, olive oil, legumes, nuts and seeds, and fish. It also positively scored low consumption of MED non-recommended dietary components such as red and processed meat, soft drinks, and sweets. To this we added several dietary features based on previous data associated with microbial composition and function. These included a positive score for plant diversity27 by scoring for different colors in the diet, consumption of fermented foods28 (specifically yogurt), and inclusion of starchy vegetables like potato in the whole grain category to promote diversity in the carbohydrate-rich food group, as well as support butyrate producers as we had previously shown.29 In addition, we aimed to positively score for relatively low UPF intake. To this end, we evaluated the average intake of sweets, snacks, sweet and savory pastries, soft drinks, and foods and drinks containing artificial sweeteners.”
Also, from Kim Beall, Cofounder and Managing Director of Nutritional Therapy for IBD:
“If you haven’t been to the website recently, we have expanded the recipe database to over 1,000 recipes with many filterable aspects and we’ve just released a new nutrition tool, the IBD Nutrition Navigator to facilitate nutrition conversations between providers and patients to find the right nutritional starting point. This is a project led by Dr. Ananthakrishnan and a dedicated team of pediatric and adult medical advisors in a two year long development process. Many have told us this is a useful tool particularly for those less familiar with nutrition in IBD. We’re excited about it’s potential to integrate nutrition in practice, with “an option for every patient”. We appreciate your support in sharing our information, tools, and resources to advance IBD nutrition care.” Here’s the link to their website:
There are 12 “best practice” recommendations. Here are a few of them:
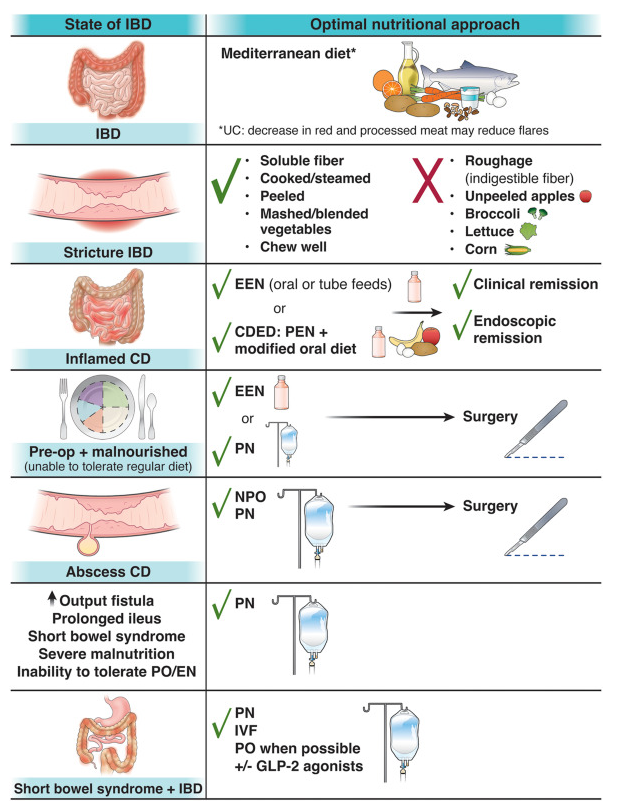
Best Practice Advice 1: Unless there is a contraindication, all patients with IBD should be advised to follow a Mediterranean diet rich in a variety of fresh fruits and vegetables, monounsaturated fats, complex carbohydrates, and lean proteins and low in ultraprocessed foods, added sugar, and salt for their overall health and general well-being. No diet has consistently been found to decrease the rate of flares in adults with IBD. A diet low in red and processed meat may reduce ulcerative colitis flares, but has not been found to reduce relapse in Crohn’s disease.
Best Practice Advice 3: Exclusive enteral nutrition using liquid nutrition formulations is an effective therapy for induction of clinical remission and endoscopic response in Crohn’s disease, with stronger evidence in children than adults. Exclusive enteral nutrition may be considered as a steroid-sparing bridge therapy for patients with Crohn’s disease.
Best Practice Advice 6: In patients with IBD who have an intra-abdominal abscess and/or phlegmonous inflammation that limits ability to achieve optimal nutrition via the digestive tract, short-term parenteral nutrition may be used to provide bowel rest in the preoperative phase to decrease infection and inflammation as a bridge to definitive surgical management and to optimize surgical outcomes.
Best Practice Advice 7: We suggest the use of parenteral nutrition for high-output gastrointestinal fistula, prolonged ileus, short bowel syndrome, and for patients with IBD with severe malnutrition when oral and enteral nutrition has been trialed and failed or when enteral access is not feasible or contraindicated.
Best Practice Advice 10: All patients with IBD should be monitored for vitamin D and iron deficiency. Patients with extensive ileal disease or prior ileal surgery (resection or ileal pouch) should be monitored for vitamin B12 deficiency.
Best Practice Advice 12:Breastfeeding is associated with a lower risk for diagnosis of IBD during childhood. A healthy, balanced, Mediterranean diet rich in a variety of fruits and vegetables and decreased intake of ultraprocessed foods have been associated with a lower risk of developing IBD.
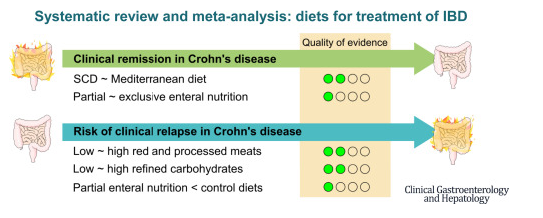
This was a systematic review of prospective controlled trials (n=27) of solid food diets for the induction or maintenance of remission in IBD.
Key findings:
For induction of remission in Crohn’s disease (CD), the Mediterranean diet was similar to the Specific Carbohydrate Diet (low certainty of evidence), and partial enteral nutrition (PEN) was similar to exclusive enteral nutrition (very low certainty of evidence).
PEN reduced risk of relapse (very low certainty of evidence), whereas reduction of red meat or refined carbohydrates did not (low certainty of evidence).
For ulcerative colitis, diets were similar to controls (very low and low certainty of evidence).
My take: Most of the dietary treatments for IBD have low to very low certainty of evidence regarding their effectiveness. Dietary changes are very likely to be helpful but more studies with rigorous endpoints are still needed.
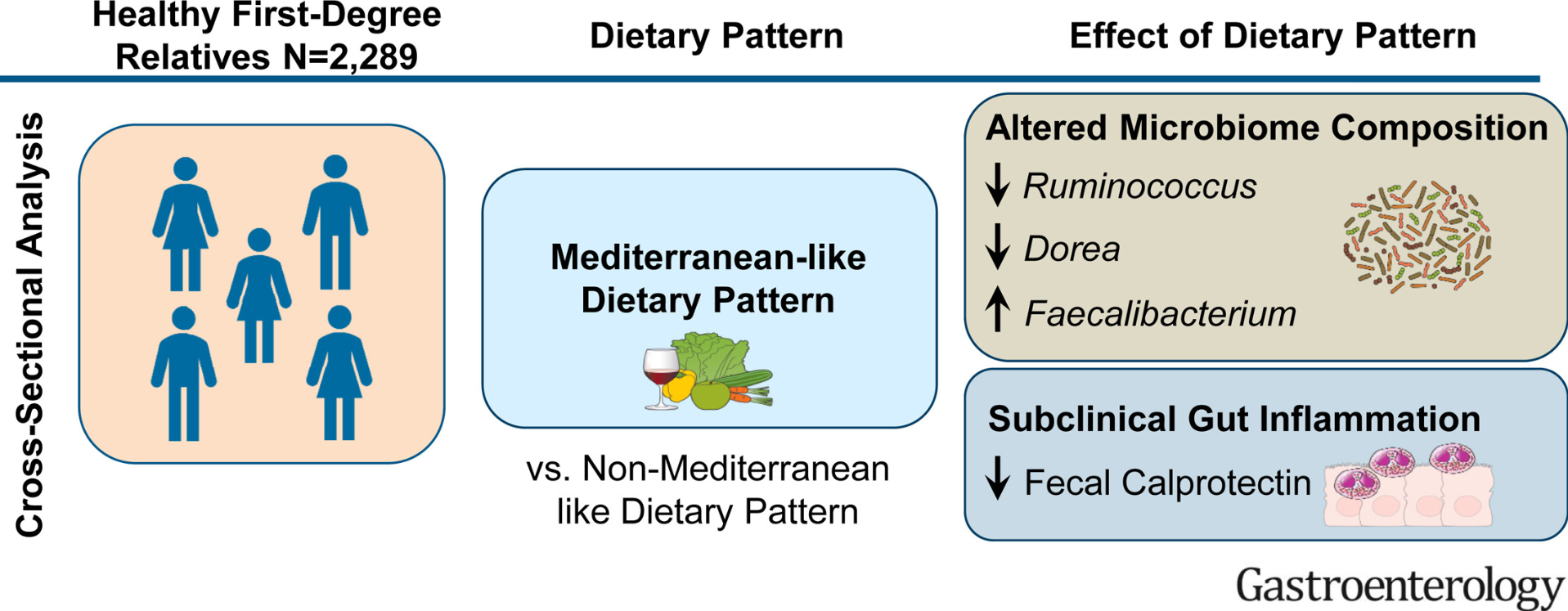
As part of the Genetic, Environmental, Microbial (GEM) Project, the researchers recruited a cohort of 2289 healthy first-degree relatives of patients with Crohn’s disease. Diet was assessed with a food frequency questionnaire. Key finding: A Mediterranean-like dietary pattern is associated with microbiome (increased Ruminococcus, as well as taxa such as Faecalibacterium) and lower intestinal inflammation.
L Zhao et al. Gastroenterol 2022; 163: 699-711. Open Access! Uncovering 1058 Novel Human Enteric DNA Viruses Through Deep Long-Read Third-Generation Sequencing and Their Clinical Impact This study discovered 1058 novel human gut viruses, and these findings can contribute to current viral reference genome, future virome investigation, and colorectal cancer diagnosis. From the editorial: “Previous literature also identified virome signatures associated with certain diseases, such as colorectal cancer14 or inflammatory bowel disease,15 such that a better understanding of the viral dark matter may be used to develop biomarkers to identify individuals at risk or even to influence gut physiology.”
Personal item: If any blog follower has experience using biologics (eg mepolizumab, benralizumab) in a young child (1 yo) with eosinophilic colitis and marked eosinophilia, please send me a personal email: jjhochman@gmail.com.
“Another series of studies from the University of Texas found that four seconds — yes, seconds — of ferocious bicycle pedaling, repeated several times, was enough to raise adults’ strength and endurance, whatever their age or health when they started.”
“As I wrote in July, the familiar goal of 10,000 daily steps, deeply embedded in our activity trackers and collective consciousness, has little scientific validity. It is a myth that grew out of a marketing accident, and a study published this summer further debunked it, finding that people who took between 7,000 and 8,000 steps a day, or a little more than three miles, generally lived longer than those strolling less or accumulating more than 10,000 steps.”
“Exercise also has a disproportionate impact on our odds of enjoying a long, healthy life. According to one of the most inspiring studies this year, overweight people who started working out lowered their risk of premature death by about 30 percent even if they remained overweight, with exercise providing about twice as much benefit as weight loss might…Exercise enhances our brain power, too, according to other, memorable experiments from this year”
“In the study, which I wrote about in May, active people reported a stronger sense of purpose in their lives than inactive people….In effect, the more people felt their lives had meaning, the more they wound up moving, and the more they moved, the more meaningful they found their lives.
For successful aging, recognize one’s issues and adapt accordingly. “Sooner or later, we all must recognize what is no longer possible and find alternatives,” says Jane Brody (Personal Health columnist) –“Inspired by Steven Petrow’s book, “Stupid Things I Won’t Do When I Get Old.”
Learning from ‘Super-Agers’ — “past research has revealed lifestyle factors that contribute to resilience such as obtaining a high level of quality education; holding occupations that deal with complex facts and data; consuming a Mediterranean-style diet; engaging in leisure activities; socializing with other people; and exercising regularly”
The sweet spot for longevity lies around 7,000 steps a day (or 30 minutes of exercise).
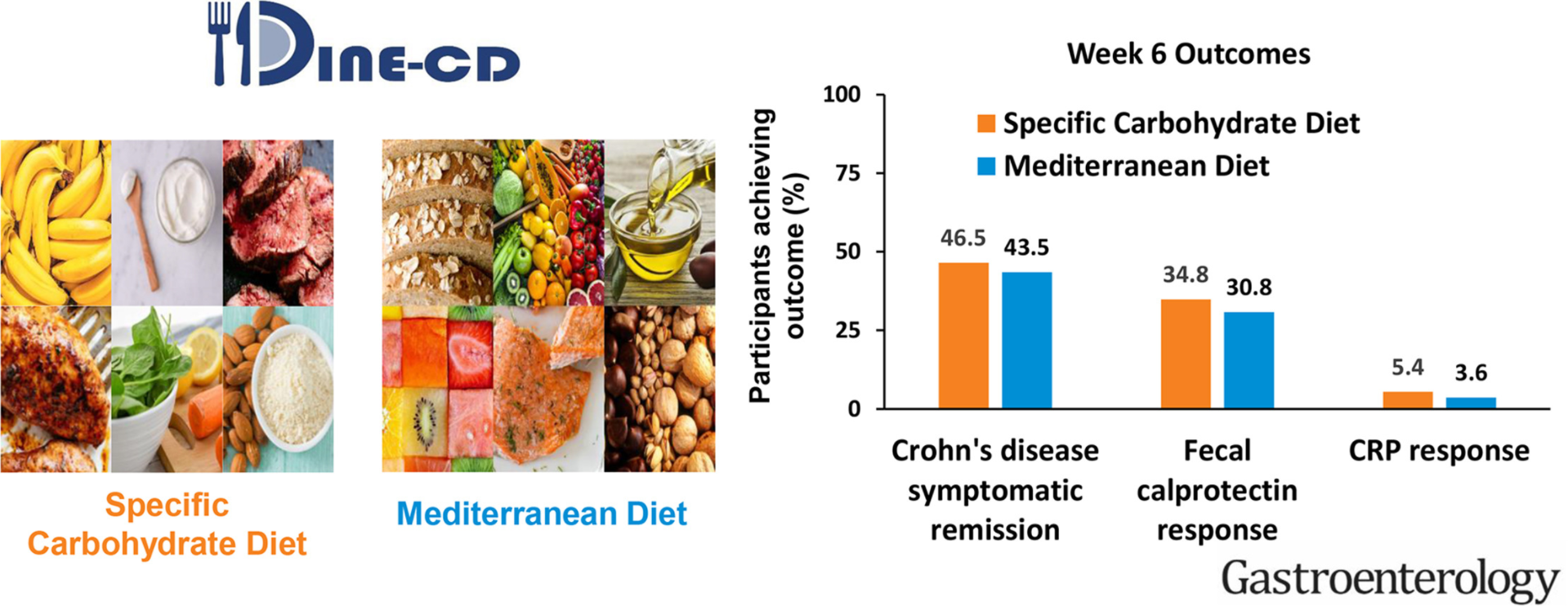
This study compared the effectiveness of the Specific Carbohydrate Diet (SCD) to the Mediterranean Diet (MD) as treatment for Crohn’s disease (CD) with mild to moderate symptoms.
Methods
Adult patients with CD and with mild-moderate symptoms were randomly assigned 1:1 to consume the MD or SCD for 12 weeks. For the first 6-weeks, participants received prepared meals and snacks according to their assigned diet. After 6-weeks, participants were instructed to follow the diet independently. The primary outcome was symptomatic remission at week 6. Key secondary outcomes at week 6 included: fecal calprotectin (FC) response (FC <250 μg/g and reduction by >50% among those with baseline FC >250 μg/g) and C-Reactive Protein (CRP) response (high-sensitivity CRP (hsCRP) <5 mg/L and >50% reduction from baseline among those with hsCRP >5mg/L).
Results
194 patients were randomized, and 191 were included in the efficacy analyses. The percentage of participants who achieved symptomatic remission at week 6 was not superior with SCD (SCD 46.5%, MD 43.5%; P = .77). FC response was achieved in 8/23 participants (34.8%) with SCD and 4/13 participants (30.8%) with MD (P = .83). CRP response was achieved in 2/37 participants (5.4%) with SCD and 1/28 participant (3.6%) with MD (P = .68).
Conclusions
SCD was not superior to MD to achieve symptomatic remission, FC response and CRP response. CRP response was uncommon. Given these results, the greater ease of following the MD, and other health benefits associated with MD, the MD may be preferred to the SCD for most patients with CD with mild to moderate symptoms.