I am a pediatric gastroenterologist at GI Care for Kids (previously called CCDHC) in Atlanta, Georgia. The goal of my blog is to share some of my reading in my field more broadly. In addition, I wanted to provide my voice to a wide range of topics that often have inaccurate or incomplete information.
Before starting this blog in 2011, I would tear out articles from journals and/or keep notes in a palm pilot. This blog helps provide an updated source of information that is easy to access and search, along with links to useful multimedia sources.
I was born and raised in Chattanooga. After graduating from the University of Virginia, I attended Baylor College of Medicine. I completed residency and fellowship training at the University of Cincinnati at the Children’s Hospital Medical Center. I received funding from the National Institutes of Health for molecular biology research of the gastrointestinal tract.
During my fellowship, I had the opportunity to work with some of the most amazing pediatric gastroenterologists and mentors. Some of these individuals included Mitchell Cohen, William Balistreri, James Heubi, Jorge Bezerra, Colin Rudolph, John Bucuvalas, and Michael Farrell. I am grateful for their teaching and their friendship. During my training with their help, I received a nationwide award for the best research by a GI fellow.
I have authored numerous publications/presentations including original research, case reports, review articles, and textbook chapters on various pediatric gastrointestinal problems. In addition, I have been recognized by Atlanta Magazine as a "Top Doctor" in my field multiple times.
Currently, I am the vice chair of the section of nutrition for the Georgia Chapter of the American Academy of Pediatrics. In addition, I am an adjunct Associate Clinical Professor of Pediatrics at Emory University School of Medicine. Other society memberships have included the North American Society for Pediatric Gastroenterology Hepatology and Nutrition (NASPGHAN), American Academy of Pediatrics, the Food Allergy Network, the American Gastroenterology Association, the American Association for the Study of Liver Diseases, and the Crohn’s and Colitis Foundation.
As part of a national pediatric GI organization called NASPGHAN (and its affiliated website GIKids), I have helped develop educational materials on a wide-range of gastrointestinal and liver diseases which are used across the country. Also, I have been an invited speaker for national campaigns to improve the evaluation and treatment of gastroesophageal reflux disease, celiac disease, eosinophilic esophagitis, hepatitis C, and inflammatory bowel disease (IBD). Some information on these topics has been posted at my work website, www.gicareforkids.com, which has links to multiple other useful resources.
I am fortunate to work at GI Care For Kids. Our group has 17 terrific physicians with a wide range of subspecialization, including liver diseases, feeding disorders, eosinophilic diseases, inflammatory bowel disease, cystic fibrosis, DiGeorge/22q, celiac disease, and motility disorders. Many of our physicians are recognized nationally for their achievements. Our group of physicians have worked closely together for many years. None of the physicians in our group have ever left to join other groups. I have also worked with the same nurse (Bernadette) since I moved to Atlanta in 1997.
For many families, more practical matters about our office include the following:
– 14 office/satellite locations
– physicians who speak Spanish
– cutting edge research
– on-site nutritionists
– on-site psychology support for abdominal pain and feeding disorders
– participation in ImproveCareNow to better the outcomes for children with inflammatory bowel disease
– office endoscopy suite (lower costs and easier scheduling)
– office infusion center (lower costs and easier for families)
– easy access to nursing advice (each physician has at least one nurse)
I am married and have two sons (both adults). I like to read, walk/hike, bike, swim, and play tennis with my free time.
I do not have any financial relationships with pharmaceutical companies or other financial relationships to disclose. I have helped enroll patients in industry-sponsored research studies.
Followup on previous blog post (Mary Suhr: Coding Update 2025) -there is a new CPT code for the PENFS procedure in 2026: 64567. This procedure has FDA approval for children/adolescents (8-21 years) with functional abdominal pain associated with irritable bowel syndrome; in addition, it has an indication for functional dyspepsia.
While it may seem like a disease from the past, this airborne illness kills more people than any other infectious disease worldwide, roughly 1.2 million a year. That number could increase dramatically because of the Trump administration’s cuts to foreign assistance, according to a new study…
As many as 10 million additional people could get TB, and 2.2 million could die by 2030 in high-burden countries under the worst-case funding scenario over the next five years, researchers report in the journal PLOS Global Public Health.
My take: I recently finished, Everything is Tuberculosis by John Green, which is a good read. So this article caught my attention. Even before the funding cuts, more effort was needed to stop the scourge of TB. Currently TB kills more than a million people per year; in some historic periods, it has killed as many as one in seven people.
Thanks to Anna Kelly for recommending the book to me.
Mary Suhr, a coding expert, provided our group with an excellent update on coding and the changes needed in documentation. I have taken some notes and shared some of her slides. There may be inadvertent omissions and mistakes in my notes.
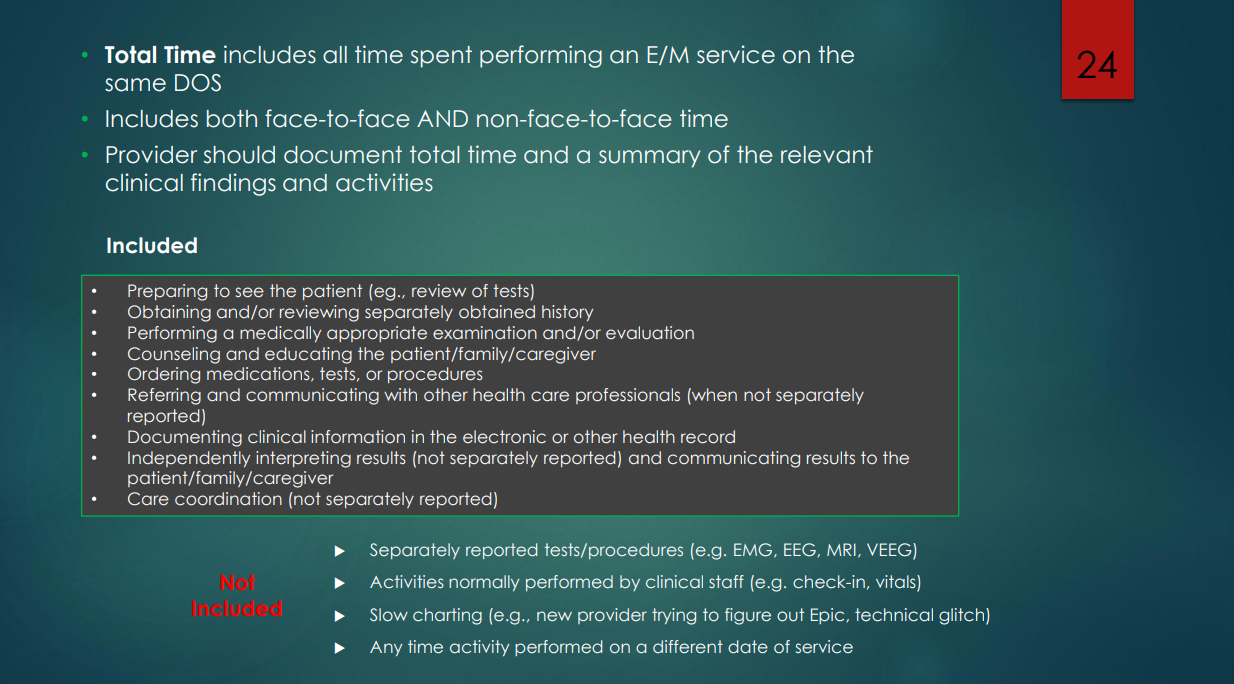
In 2025, billing/coding relies entirely on medical decision-making OR time codes. While documenting a comprehensive history and an exam are important for patient care and good practice, they are not important in billing/coding.
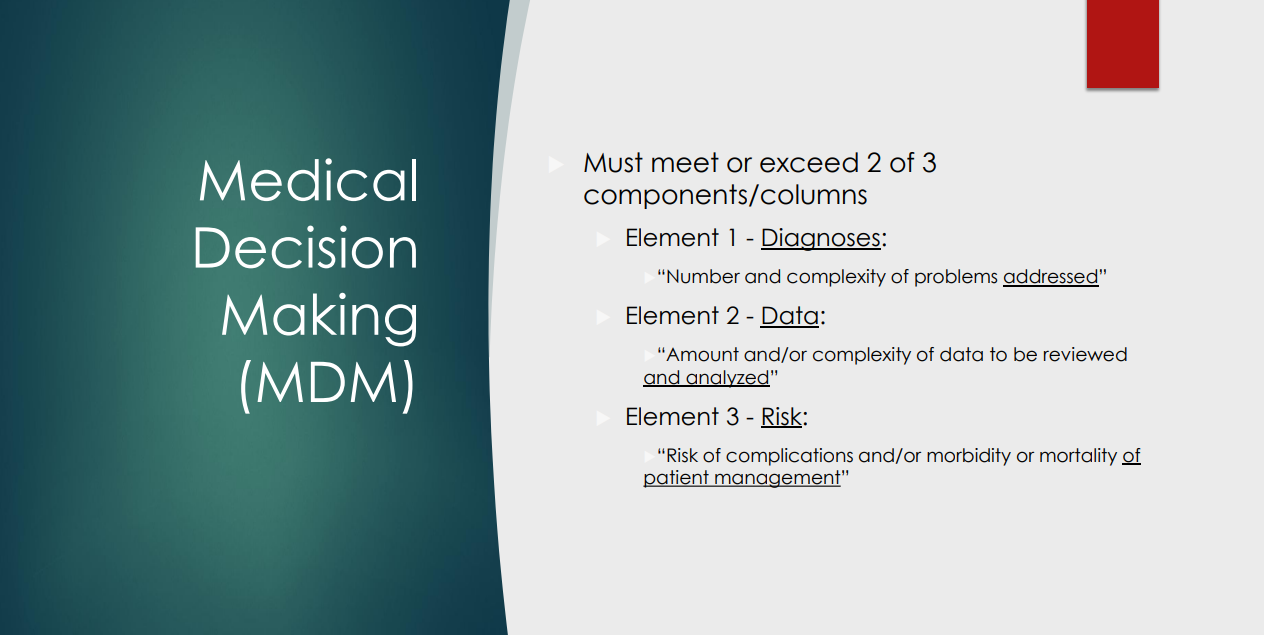
Medical decision-making (MDM) consists of three areas: diagnosis, review of data, and risks of treatment. Data includes points for each lab reviewed/ordered and each radiology test. If you order/review CBC/d, CRP, and CMP, this would be up to 3 points in this category.
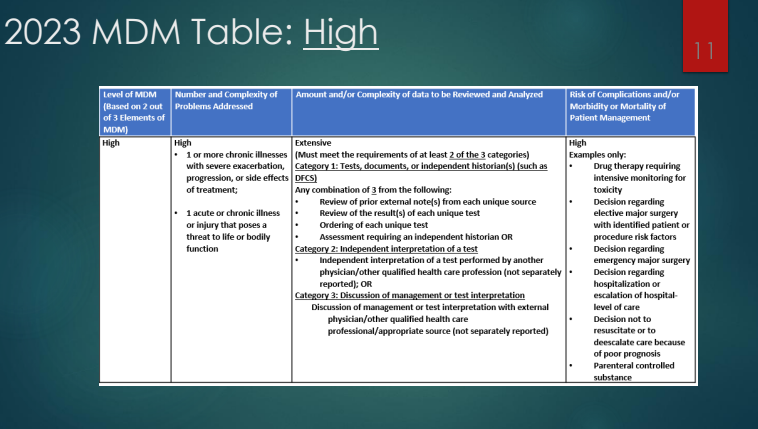
With the changes in requirements in coding, the RVUs were increased for both outpatient and inpatient codes. This reflects the increased difficulty in selecting some codes. For example, the change in requirements, some 99214 codes several years ago will now qualify for 99213 codes. It is much more difficult to use a 99215 code based on medical decision-making and the time spent is up to 40 minutes to use this code
Followup visits who are not doing well generally would NOT be a low level visit if documented appropriately
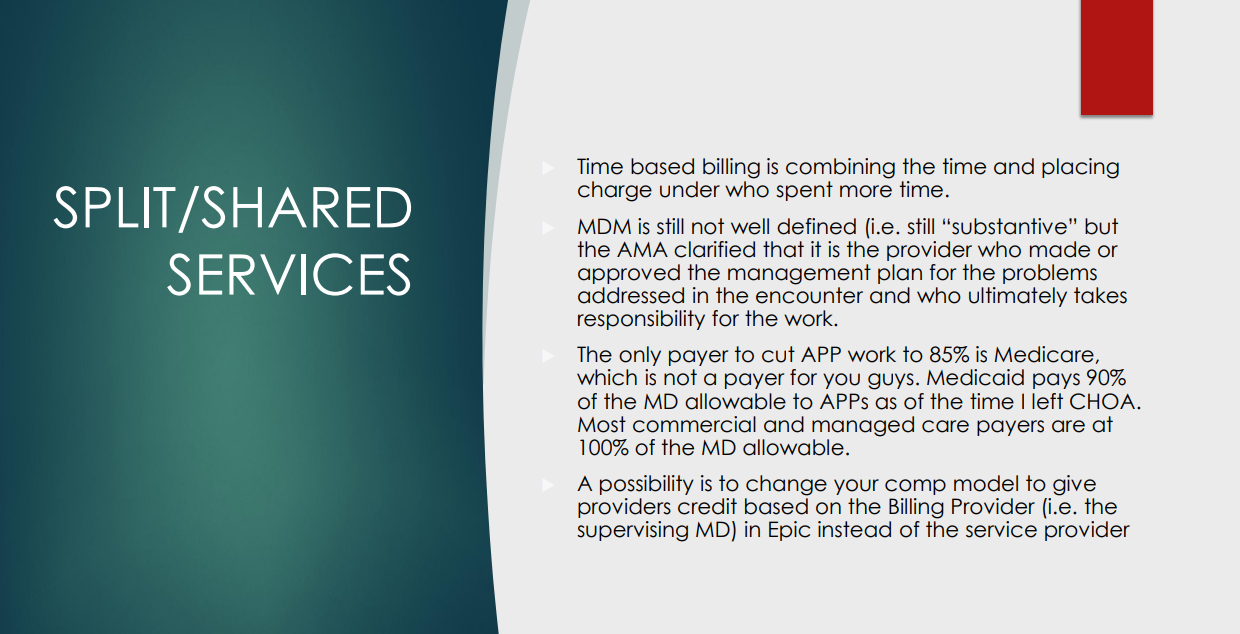
Coding for F/u visits See slide below regarding split/shared services below.If APP spends the majority of the time, then the time codes can be billed by the APP or the MD can bill based on medical decision-making (but not time code).
Discontinuing a prescription medication can be counted as prescription drug management if documentation explains the potential benefits/risks of this
Newer codes that may be useful:
G2211 –>long-term longitudinal care code
99451 –>interprofessional consultation (if patient consented). If an ED physician calls for consultation, documentation could allow for this code as long as the patient is not seen before or after within 7 days
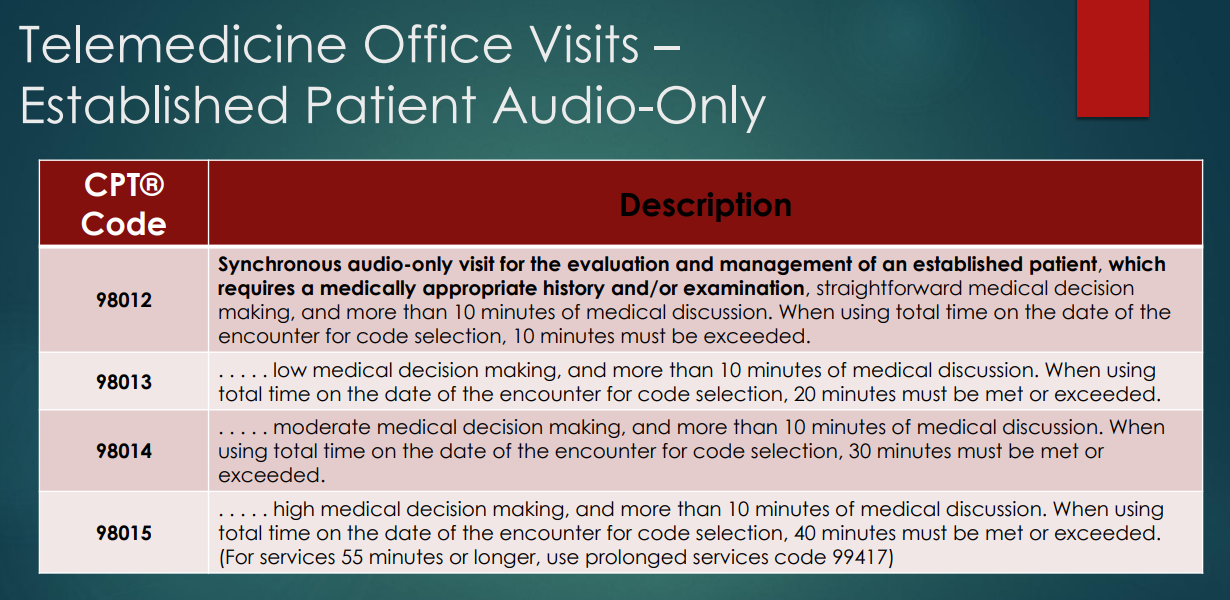
98016 –>audio (telephone) consult code for established patients. This could be used to check in to see if the patient needs an office visit
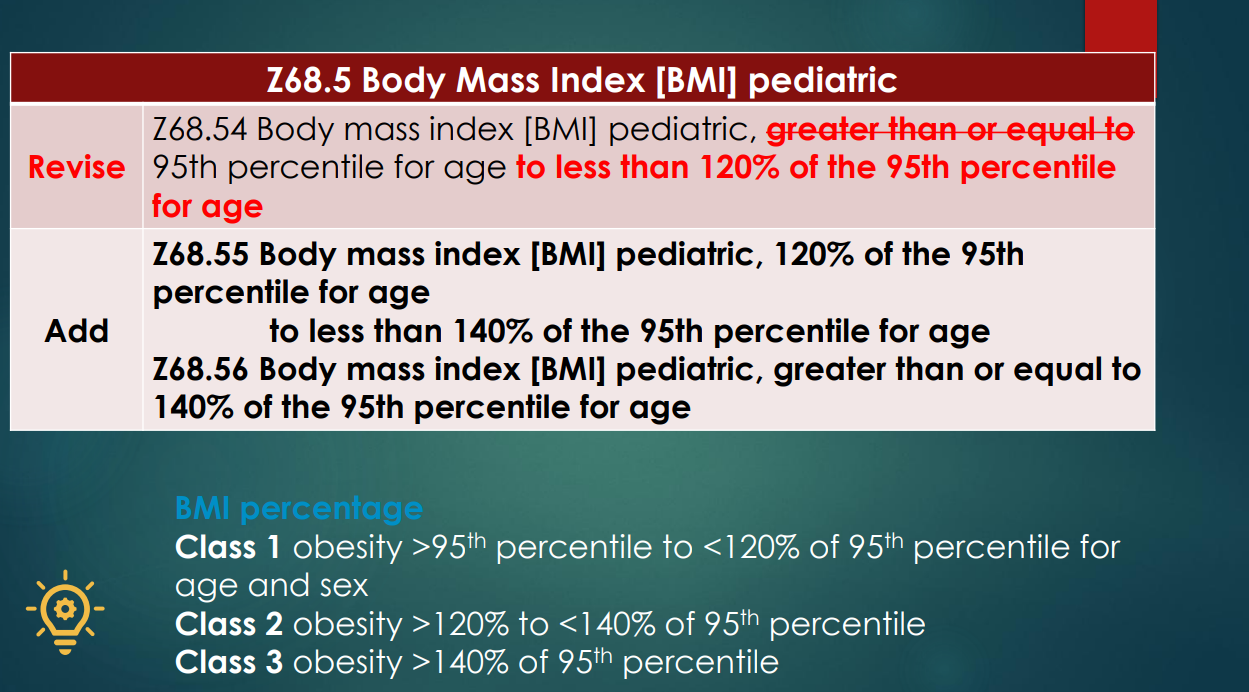
New ICD-10 codes for IBD with fistulas, BMI codes and eating disorders
If a patient is seen in ED and leaves ED, recommended to use ED codes, not office-based outpatient codes
For inpatients, HAL management is generally a high risk medication/treatment for coding-billing purposes
Document defensively. Increasingly, insurance companies are trying to downcode visits. Recommend resisting this and document why the initial codes were selected
Except for Medicaid, can use modifier 25 and bill if patient seen in clinic by one provider and in the hospital by another provider, if each was involved in patient care
This article recommends that physicians consider a proactive role in explaining the prior authorization process. Here is his suggested handout:
We want to make sure you understand something called “prior authorization.”
Often, insurance companies require us to ask their permission for coverage before prescribing a drug or doing a test or procedure. They say they do this to make sure that we are suggesting medically appropriate, cost-effective care — on behalf of you or your employer. In fact, this is always our goal, but they don’t always think we’re accomplishing it.
To try to get this authorization ahead of time, we document our logic in the format they require, and they may reject it. Often we find out about rejections well before any surgery, but sometimes we don’t.
The doctors here often don’t understand why insurers reject our requests for permission.
The prior authorization process can be as baffling to us as it may be to you, and we find it intensely frustrating. Please keep in mind that we are at the mercy of dozens of insurance companies, and their rules and requirements can change constantly. Your doctor may not be able to predict the odds of a prior authorization rejection, and musing over the possibility before it happens probably isn’t a productive use of our time together in the exam room.
We do have billing specialists who handle prior authorization requests for our doctors.
If you have any concerns once you know what we’re recommending, reach out to our billing specialist or the department that helps with this. They too may not be able to tell you much ahead of time, but they will play a role in helping us with any appeal that is necessary if our request for prior authorization fails in full or in part.
Watch for all communications — from us but especially from your insurance company.
Insurance companies like paper mail. Check yours every day, in case they issue denials that way. Download your insurance company’s app and sign up for push notifications for any changes, especially if they offer alerts specifically for changes in prior authorization. Opt in to email notifications, and check your spam.
You might hear from the insurance company before we do.
We are partners here, and you have a role.
We think we are pretty good at navigating this deeplysuboptimal system, but we can’t do it without you. Please, become intimately familiar with your insurance plan and what it covers — whether prior authorization is required or not.
Engage a human resources specialist at your employer, if you have one, to help communicate with the insurance company during the prior authorization process if you think you might need help. Call the insurer on your own to ask whether your medicine or procedures require permission and whether the insurance company is missing information it needs.
Patients can sometimes get better information faster than we can, if only because we may be trying to help hundreds of patients at once.
What happens if our prior authorization request is rejected?
There is an appeal process, which may differ by insurer. Contact a billing specialist with whatever information you have from your insurance company, though we may hear about it before you do and start the process on our own.
Sometimes, the problem is a relatively simple one, resulting from confusion over the byzantine process of submitting medical codes, or some similar snafu. But often, a doctor will have to do what’s known as a peer review with someone from the insurance company. We find this burdensome, since the “peer” on the line with us may not have the same level of expertise as we do. That prolongs the call, adds to our overall operating expenses and keeps us from spending more time with you, the patient.
We’ll give any appeal our best shot, but it may take time to schedule any peer review.
Please don’t worry.
We dislike having to give you a document like this that might produce anxiety. Still, it’s better that you be aware of how things might go than be desperately trying to reach us or learn about the prior authorization process after getting a mysterious and indecipherable rejection letter in the mail.
If things don’t go our way at first, we will have your back and argue fiercely to get you coverage for the care you need.
Still, there is only so much we can do to make this easier.
Our industry has a structural problem. We can provide you information and over-communicate, but the incentive systems are what they are.
Insurance companies may sometimes deny permission for care in order to make more money. Employers (and individuals) don’t want premiums to rise. Some patients demand that we throw everything we doctors have at every health condition. Regulators are in the middle of all of it, ordering up paperwork. And doctors are not infallible.
We wish we could fix all of that. But for now, we can be plain-spoken with you about how prior authorization works and try to make the system that we have just a bit more tolerable.
Methods: A single-center, retrospective chart review was conducted to identify pediatric patients (n=12) with T21 who underwent ERCP.
Patient characteristics:
Six patients (50%) had a history of duodenal atresia with subsequent surgical repair during the neonatal period
Four patients (33.3%) had chronic or acute recurrent pancreatitis, and two patients (16.7%) had biliary pancreatitis
Five patients (41.7%) had a biliary stricture that required stenting
Choledocholithiasis was present in 7 of the 12 patients (58.3%)
Key findings:
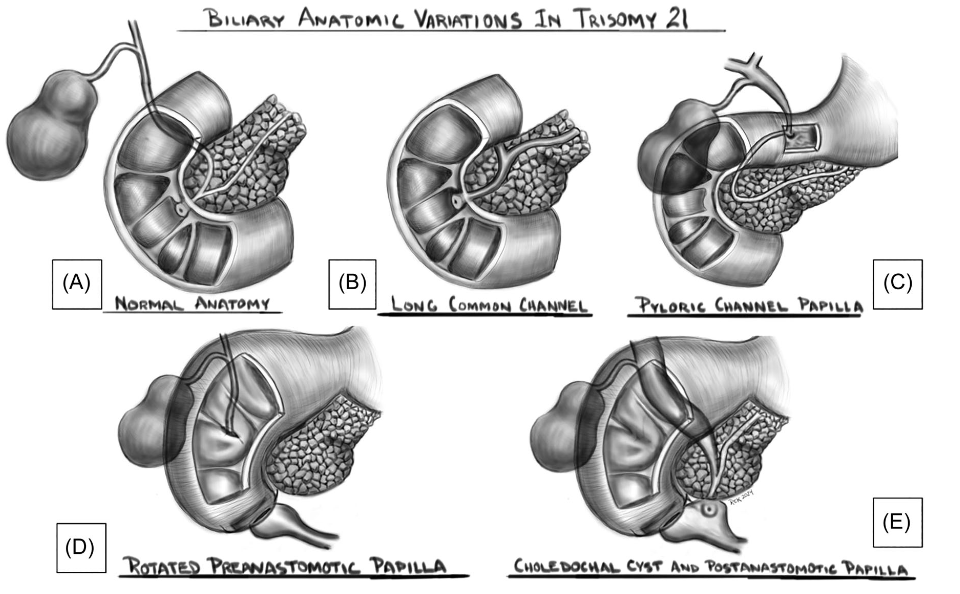
Eight patients (66.7%) were found to have an abnormal location of the major papilla. This included three patients’ papillae which were in the blind duodenal pouch created after duodenal atresia surgery (Figure 1B) and two patients had their papilla in the proximal duodenum/bulb (Figure 1D)
Two patients (16.7%) had unsuccessful ERCP either due to difficult cannulation or inability to find the major papilla
Figure 1: Biliary anatomic variations in Trisomy 21. Shown are drawings that represent variations of the location of the major papilla.(A) Normal; (B) normal location but with a long common channel; (C) pylorus; (D) postsurgical pre‐anastomotic location; and (E) postanastomotic location with choledochal cyst. Illustrations by Dr. Robert E. Kramer.
My take: In patients with trisomy 21, ERCP may be quite challenging due to anatomic variations and stricturing. In some patients in this cohort, a front-viewing scope was helpful.
The authors of this article have a sanguine interpretation of the health care landscape. Here are some excerpts:
The health care industry is exceptional in the United States: it relies on private businesses operating in markets to fulfill a fundamental human need. Because of health care’s essential nature, many observers have viewed the growing influence of large companies in the industry, known as “corporatization,” as odious, akin to privatization of fire and police departments. The corporatization of health care often evokes images of rapacious companies that prioritize profits over patients, since corporations operate according to the logic of business, emphasizing efficiency and financial returns, whereas medical institutions have traditionally operated as professional or charitable enterprises…
Evaluating corporatization requires understanding why it occurs, when it can succeed, and why it can go wrong.
Corporatization represents a deal between organizations and investors. New technologies, upgraded facilities, research and development, and competitive salaries are expensive but are necessary to meet the expectations of patients, who value improvements in health more than improvements in other goods. Investors supply the capital needed to support these enhancements and, in exchange, expect a financial return on their investment….Corporatization unlocks capital in return for growth that prioritizes profits, and investors may take an ownership stake in an organization or adjust management incentives to generate the necessary profits.
But is this deal a good one?…agreements are voluntary and therefore presumably benefit the investors and medical organizations involved. But the key question for society and for policymakers is whether corporatization benefits groups that are not party to such deals: patients and payers…
But for several reasons, health care is exceptional among U.S. markets in that profits and value often don’t align.
First, patients may not be able to accurately assess the quality of medical care, so firms can make money by cutting corners, with little fear of affecting demand. Second, firms may engage in corporatization simply to build market power, which drives up prices. Third, many medical products and services are fundamentally unprofitable because people who could benefit from them cannot afford them…
Corporatization’s effects on nursing home care appear to be largely negative. After being acquired by a private equity firm, nursing homes tend to avoid sicker residents, deliver lower-quality care, and have higher resident mortality2 …
The biopharmaceutical industry is an example of a sector that probably couldn’t exist without investors, since enormous amounts of funding are needed to conduct expensive clinical trials with high failure rates…
Corporatization isn’t the only tool medical firms can use to raise capital. One alternative is government funding, including subsidized loans or tax credits. But relying on public financing has downsides. Governments struggle to identify what patients want, owing to bureaucratic hurdles, a lack of incentives, and budgetary constraints. They are also subject to shifting political climates, making them unreliable funders for large or long-term investments that require steady outlays…
What steps can be taken to unlock the benefits of corporatization while limiting its harms? The guiding objective should be better aligning profits (which drive corporate decision making) with value for patients…
A second approach involves empowering regulators to enforce antitrust rules aimed at limiting market power that wasn’t sanctioned — or regulating prices when those efforts fail. But regulators already have these goals and struggle to achieve them because of tight budgets and bureaucratic limits…
Corporatization will always involve trade-offs because there is no simple or universal “fix” to align profits with value for patients. In each area of medicine, regulators will need to decide whether the deal inherent to corporatization is a worthwhile one — and whether the alternatives are any better.
My take: It is refreshing to see a different viewpoint regarding the profit-driven U.S. health care system. While this is not the system most observers would have created, it is what we have and the currently available alternatives could be worse.
It seems that many of our plants at our home are sensitive too. The ones that survive seem to attract deer. This Bonsai plant was estimated to be more than 400 years old
This study had a clever design: the authors examined the liver findings from overweight/obese children (n=168) who underwent renal ultrasounds to help determine the frequency of hepatic steatosis. Quantification of the hepatorenal index (HRI) by ultrasound has been shown to provide moderate diagnostic performance for detecting hepatic steatosis in children. (Ref: Frankland MP et al. Diagnostic performance of ultrasound hepatorenal index for the diagnosis of hepatic steatosis in children. Pediatr Radiol. 2022; 52(7): 1306-1313)
This design helped avoid a selection bias present in most studies which have examined ultrasonography in children with elevated liver enzymes. The authors did try to correlate the imaging findings with blood tests. Serum laboratory data were available for 50 patients at a mean interval of 115 days (0–366) from the ultrasound examination.
Key findings:
91 (54%) patients had an abnormally elevated HRI (>1.75). An abnormally elevated HRI was present in 58% (50/86) of patients with overweight and 50% (41/82) of patients with obesity
Of the 12 patients with abnormal ALT, 5 (42%) had an abnormal ultrasound HRI and 7 (58%) had a normal ultrasound HRI
Discussion points:
“MASLD can occur at a very young age and should be considered in at-risk patients. Importantly, only 21% (5/24) of the patients with imaging evidence of steatosis and available labs had elevated ALT and 58% (7/12) of patients with an elevated ALT did not have imaging evidence of steatosis, suggesting that ALT may not be a useful biomarker for MASLD screening at this age.”
My take: Hepatic steatosis is likely present in about half of children with early onset overweight/obesity. ALT values are often normal in this cohort.
Methods: In this single-center, observational study, the authors deployed an anonymized survey of outcomes that was completed by 107 parents of children with BA who were younger than age 12 years. A detailed assessment of general neurodevelopment (Mullens Scale of Early Learning and Vineland Adaptive Behavior Scale) was carried out in 50 infants younger than 5 years old, and emerging autistic traits (Autism Diagnostic Observation Schedule) were assessed in those eligible. There were 93 matched controls.
Key findings:
Neurodevelopmental concerns were raised by 37% of parents
47% of children required support from at least 1 service (such as speech and language therapy physiotherapy, play therapy, or seen a clinical psychologist), and a further 42% (n = 45) had used more than 1 service. The most accessed service was speech and language therapy (20%, n = 10)
A clinical or research diagnosis of autism was made in 30% of 35 children >2 years old
Early surgical intervention and faster clearance of jaundice after surgery was associated with better general neurodevelopmental outcomes (F = 2.428, P = .042) but not with the presence of emerging autistic traits
My take: High levels of neurodevelopmental difficulties occur in children with BA.
I am not an expert on autism. However, I am concerned about the administration’s recent recommendations regarding acetaminophen and autism. Even scientists who have suggested a possible link have NOT recommended stopping the use of acetaminophen during pregnancy.
It is well-recognized that autism is related to multiple factors, both genetic and potential environmental factors. The use of acetaminophen, even if linked to autism, could represent an epiphenomenon in which a primary disorder (like a fever or infection) is responsible for subsequent neurodevelopmental problems rather than the medicine itself. While there has been growing concern about the increasing frequency of autism, much of this relates to changes in the definition of autism over various periods.
I recommend the following recent sources of information on this topic:
Editorial Board Wall Street Journal, 9/23/25: Trump, Tylenol and the Plaintiffs Bar “The acetaminophen link to autism is based on weak evidence pushed by RFK Jr. and his legal allies.”
“Today’s announcement by HHS is not backed by the full body of scientific evidence and dangerously simplifies the many and complex causes of neurologic challenges in children. It is highly unsettling that our federal health agencies are willing to make an announcement that will affect the health and well-being of millions of people without the backing of reliable data.
“In more than two decades of research on the use of acetaminophen in pregnancy, not a single reputable study has successfully concluded that the use of acetaminophen in any trimester of pregnancy causes neurodevelopmental disorders in children. In fact, the two highest-quality studies on this subject—one of which was published in JAMA last year—found no significant associations between use of acetaminophen during pregnancy and children’s risk of autism, ADHD, or intellectual disability.
“Acetaminophen is one of the few options available to pregnant patients to treat pain and fever, which can be harmful to pregnant people when left untreated. Maternal fever, headaches as an early sign of preeclampsia, and pain are all managed with the therapeutic use of acetaminophen, making acetaminophen essential to the people who need it. The conditions people use acetaminophen to treat during pregnancy are far more dangerous than any theoretical risks and can create severe morbidity and mortality for the pregnant person and the fetus.”
From KFF News:
In August, Bauer and her colleagues published an analysis of 46 previous studies on Tylenol, autism, and attention-deficit/hyperactivity disorder. Many found no link between the drug and the conditions, while some suggested Tylenol might occasionally exacerbate other potential causes of autism, such as genetics.
Bauer, an epidemiologist at the University of Massachusetts-Lowell, and her team called for more judicious use of the drug until the science is settled.
Autism experts at the Centers for Disease Control and Prevention were neither consulted for the White House’s long-awaited autism announcement nor asked to review a draft of the findings and recommendations…
If prenatal Tylenol has any association, which it may not, it would help account for only a fraction of cases, she said. Further, research has not deeply examined Tylenol risks in young children, and manyrigorous studies refute a link between vaccines and autism.
Bauer worries such statements will cut both ways: People may put themselves at risk to avoid vaccines and Tylenol, the only safe painkiller for use during pregnancy. And she frets that scientists might outright reject her team’s measured concerns about Tylenol in a backlash against misleading remarks from Trump and other members of his “Make America Healthy Again” movement….
Helen Tager-Flusberg, director of the Center for Autism Research Excellence at Boston University, called Trump’s comments dangerous. Fevers can harm the mother and the developing fetus, she said, adding that fevers are more strongly associated with autism than Tylenol…
Several medical and scientificassociations have called for Kennedy’s removal or resignation. Many scientists are skeptical of what he says because much of it has been misleading or wrong. For example, he’s said HIV isn’t the only cause of AIDS (it is), that antidepressant drugs cause mass shootings (they don’t), that older adults don’t have severe autism (some do), that the measles vaccine causes brain swelling (it doesn’t), that covid vaccines were the deadliest vaccines ever made (they aren’t), that vaccines aren’t safety-tested (they are), and that vaccines contribute to autism (they don’t).
From the Wall Street Journal:
Washington Post Editorial:
From TIME article: “Despite what we are now hearing from the most powerful health offices in the nation, the science on acetaminophen and autism remains unsettled. What is not unsettled is the damage done when politics masquerades as medicine. Every false certainty erodes the trust that holds the fragile bridge between patients and their doctors. Break that trust, and no study, no drug, no vaccine will be enough to save lives when the next real crisis comes. When politicians play doctor, it’s families who will pay the price.”
My take: Thinking about the damage from this press conference, I was reminded of a scene from the movie “Doubt.” In the movie Doubt, Father Flynn (played by Philip Seymour Hoffman) tells a parable about an old priest instructing a woman who has been gossiping to take a pillow, cut it open on her roof, and then return to gather up all the feathers. When she tells him it can’t be done because “the wind took them all over,” the priest responds: “And that… is gossip!”
The spreading of damaging rumors and lies, which is being done by leaders of this country, is impossible to contain or undo once released, and its impact is far-reaching and destructive.
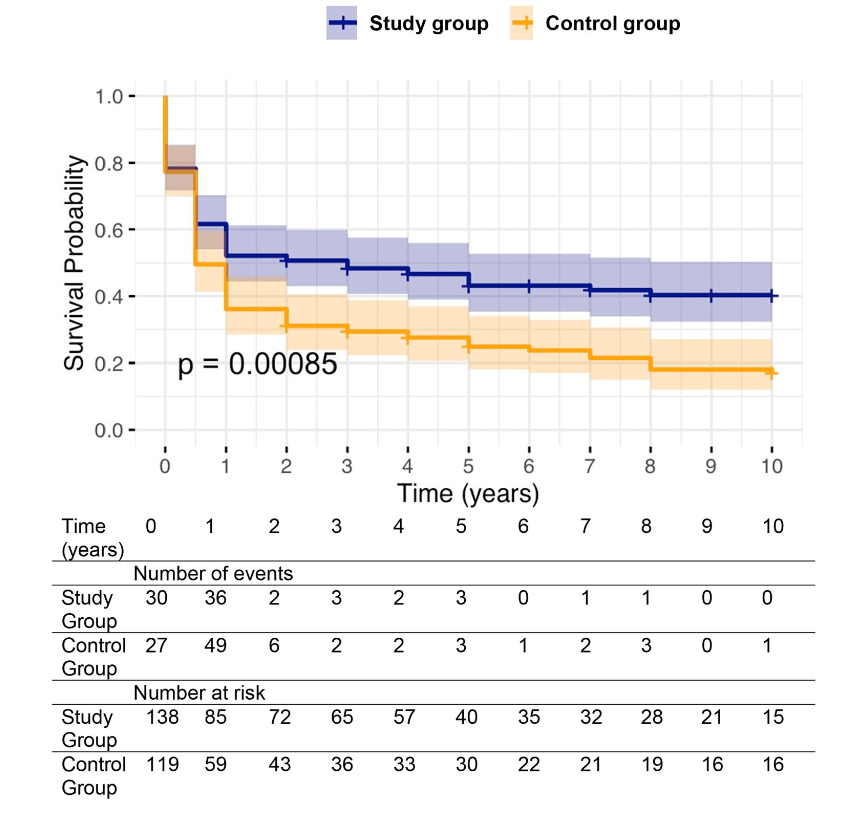
Background: After the START trial in 2014, it seemed that enthusiasm for post-operative steroids for biliary atresia had waned. The START study did not find that steroids improved outcomes after Kasai hepatoportoenterostomy (HPE). Subsequently, though, there have been observational reports of using steroids in a customized fashion to improve outcomes. Langreen et al add to this literature by examining their use of rectal budesonide (2 mg) for 3 months in a retrospective cohort (n=142) with a historical control (n=137). Jaundice-free native liver survival (jfNLS) was assessed at 6 months, 2 years, 5 years, and 10 years post-Kasai.
Key findings:
Improvements were noted in jfNLS at 6 months (53% vs. 39%) , 2 years (45% vs. 22%), 5 years (40% vs. 23%) and 10 years (32% vs. 13%)
These benefits were exclusive to patients with nonsyndromic BA
No serious adverse effects were identified with budesonide
Rationale for rectal budesonide: The authors note that “a single dose of budesonide foam contains about 2 mg of budesonide, equivalent to 25 mg of prednisolone or 20 mg of methylprednisolone…In our series, no serious steroid associated adverse effects were recorded, possibly due to the first pass after rectal administration.”
Limitations: “The retrospective nature of our data analysis allows for variability in the follow‐up protocols, potential biases (historical control group, change of surgeons) and confounding factors cannot be entirely ruled out.”
Kaplan–Meier curve comparing native liver survival between the study and control groups over a 10‐year follow‐up.. Study group—blue. Control group—orange.
My take: The START study with 140 participants was well-designed and did not find a benefit with systemic steroids. However small differences in outcomes can be difficult to identify. Rectal budesonide may improve outcomes. A randomized, double-blind, placebo-controlled trial would be more definitive.
LT is resource-intensive and costly, with expenditures rising dramatically in recent years. Factors contributing to this increase in cost include expanded transplant criteria (higher risk recipients), utilization of marginal organs, and broader organ distribution, resulting in significant logistical expenses
Advanced technologies like organ perfusion devices, while promising better outcomes, further inflate costs due to their high price and market monopolization
Despite rising costs, reimbursement has remained largely stagnant, putting financial strain on transplant programs, and threatening their sustainability. “In fact, there has been an observed decline (−32%) in adjusted reimbursement of LT by Medicare over the past decade.62“
“According to the latest annual SRTR report, patients aged 65 or older undergoing LT accounted for 21.9% of transplants in 2022, up from 14.6% a decade prior.18 One study looking at the cost burden of hospitalizations associated with liver transplants from 2016 to 2019 found mean costs increasing by nearly $10,000 per hospitalization in the group aged >65 over the study period”
“Increasing numbers of patients are being transplanted for steatotic liver disease… LT associated with metabolic dysfunction–associated steatotic liver disease has been demonstrated to be associated with higher costs, largely attributable to longer posttransplant lengths of stay.21–23 Similarly, LT associated with AH/ALD is very expensive—at 1 transplant program, net revenue from LT admission to 90 days after LT was −5.0% for AH compared to +1.4% for acute-on-chronic liver failure.24“
Organ distribution:
“In 2019, the OPTN implemented further changes in liver allocation from a regional-based system to an acuity circle model. This model was intended to create a more equitable allocation system and to reduce waitlist mortality for patients across the United States…This has been associated with a 77% increase in fly-out costs, amounting to an increase in $47,010,190 across all LT centers by recent estimates.4“
“1 study found that the cost for private jets ranged from $6850 to $27,350 depending on the distance traveled.29 In this same study, commercial flights, as opposed to private jets, were found to be safe and only around 10% of the cost.”
Perfusion devices:
“The FDA’s approval of organ perfusion and preservation devices has ushered in a new era in organ transplantation, enabling medical teams to extend the geographical reach for organ procurement. These devices enhance the utilization of organs that may have previously been discarded… It has been suggested that the average cost of using normothermic regional perfusion for DCD organs is around $10,000 per donor, compared to the $40,000–$80,000 per donor for use of NMP [normothermic machine perfusion].”
My take: Transplant centers are getting squeezed financially. In addition, ~25% of liver transplant patients experience a high financial burden. Pretty soon, along with checking organs for suitability, it may be necessary to assess liver transplant centers for viability.