About gutsandgrowth
I am a pediatric gastroenterologist at GI Care for Kids (previously called CCDHC) in Atlanta, Georgia. The goal of my blog is to share some of my reading in my field more broadly. In addition, I wanted to provide my voice to a wide range of topics that often have inaccurate or incomplete information.
Before starting this blog in 2011, I would tear out articles from journals and/or keep notes in a palm pilot. This blog helps provide an updated source of information that is easy to access and search, along with links to useful multimedia sources.
I was born and raised in Chattanooga. After graduating from the University of Virginia, I attended Baylor College of Medicine. I completed residency and fellowship training at the University of Cincinnati at the Children’s Hospital Medical Center. I received funding from the National Institutes of Health for molecular biology research of the gastrointestinal tract.
During my fellowship, I had the opportunity to work with some of the most amazing pediatric gastroenterologists and mentors. Some of these individuals included Mitchell Cohen, William Balistreri, James Heubi, Jorge Bezerra, Colin Rudolph, John Bucuvalas, and Michael Farrell. I am grateful for their teaching and their friendship. During my training with their help, I received a nationwide award for the best research by a GI fellow.
I have authored numerous publications/presentations including original research, case reports, review articles, and textbook chapters on various pediatric gastrointestinal problems. In addition, I have been recognized by Atlanta Magazine as a "Top Doctor" in my field multiple times.
Currently, I am the vice chair of the section of nutrition for the Georgia Chapter of the American Academy of Pediatrics. In addition, I am an adjunct Associate Clinical Professor of Pediatrics at Emory University School of Medicine. Other society memberships have included the North American Society for Pediatric Gastroenterology Hepatology and Nutrition (NASPGHAN), American Academy of Pediatrics, the Food Allergy Network, the American Gastroenterology Association, the American Association for the Study of Liver Diseases, and the Crohn’s and Colitis Foundation.
As part of a national pediatric GI organization called NASPGHAN (and its affiliated website GIKids), I have helped develop educational materials on a wide-range of gastrointestinal and liver diseases which are used across the country. Also, I have been an invited speaker for national campaigns to improve the evaluation and treatment of gastroesophageal reflux disease, celiac disease, eosinophilic esophagitis, hepatitis C, and inflammatory bowel disease (IBD). Some information on these topics has been posted at my work website, www.gicareforkids.com, which has links to multiple other useful resources.
I am fortunate to work at GI Care For Kids. Our group has 17 terrific physicians with a wide range of subspecialization, including liver diseases, feeding disorders, eosinophilic diseases, inflammatory bowel disease, cystic fibrosis, DiGeorge/22q, celiac disease, and motility disorders. Many of our physicians are recognized nationally for their achievements. Our group of physicians have worked closely together for many years. None of the physicians in our group have ever left to join other groups. I have also worked with the same nurse (Bernadette) since I moved to Atlanta in 1997.
For many families, more practical matters about our office include the following:
– 14 office/satellite locations
– physicians who speak Spanish
– cutting edge research
– on-site nutritionists
– on-site psychology support for abdominal pain and feeding disorders
– participation in ImproveCareNow to better the outcomes for children with inflammatory bowel disease
– office endoscopy suite (lower costs and easier scheduling)
– office infusion center (lower costs and easier for families)
– easy access to nursing advice (each physician has at least one nurse)
I am married and have two sons (both adults). I like to read, walk/hike, bike, swim, and play tennis with my free time.
I do not have any financial relationships with pharmaceutical companies or other financial relationships to disclose. I have helped enroll patients in industry-sponsored research studies.
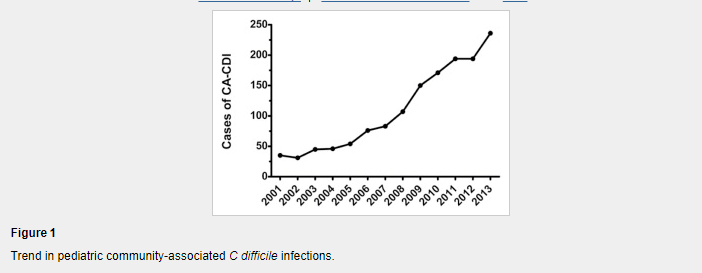
From J Pediatr -full text: Risk Factors for Community-Associated Clostridium difficile Infection in Children (DJ Adams J Pediatr 2017; 186: 105-9)
Methods: We performed a case-control study using billing records from the US military health system database
Results (from abstract):
A total of 1331 children with CA-CDI were identified and 3993 controls were matched successfully. Recent exposure to fluoroquinolones, clindamycin (OR 73.00; 95% CI 13.85-384.68), third-generation cephalosporins (OR 16.32; 95% CI 9.11-29.26), proton pump inhibitors (OR 8.17; 95% CI 2.35-28.38), and to multiple classes of antibiotics, each was associated strongly the subsequent diagnosis of CA-CDI. Recent exposure to outpatient healthcare clinics (OR 1.35; 95% CI 1.31-1.39) or to a family member with CDI also was associated with CA-CDI.
Table 2 lists other medications and their risks; for example, corticosteroids had adjusted OR of 1.22 and H2-receptor antagonists had adjusted OR of 3.33. The OR of fluoroquinolone could not be calculated as 51 cases were exposed compared with 0 controls
In their discussion, the authors note the following:
Our study supports the occurrence of CDI among a population of children who were never hospitalized previously and provides a broad characterization of the medication and epidemiologic exposures associated with pediatric CA-CDI cases. Recent exposure to fluoroquinolones, clindamycin, third-generation cephalosporins, and to multiple classes of antibiotics was associated strongly with the subsequent diagnosis of CA-CDI in children; however, a sizeable minority had no preceding antibiotic exposure.
My take: This large study shows that CDI is more frequent after antibiotic usage and after usage of acid suppression (particularly with proton pump inhibitor) therapy.
Related blog posts:

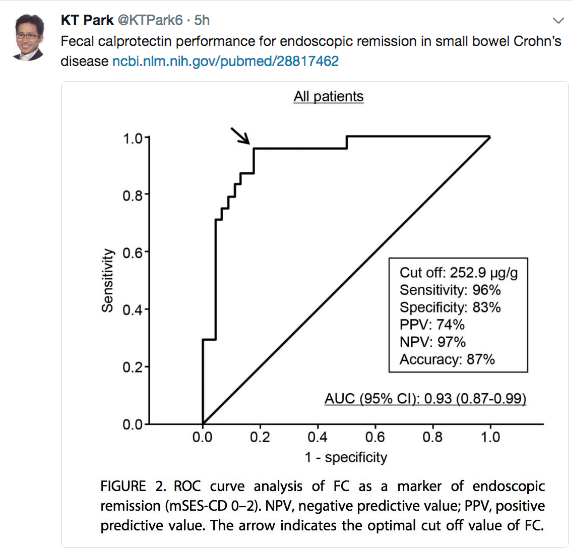
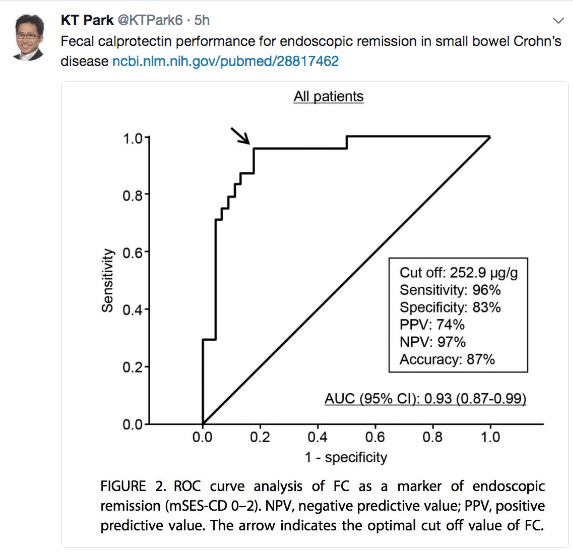
Thanks to KT Park’s Twitter feed for this reference: GA Holtman et al. JAMA Pediatr. Published online August 14, 2017. doi:10.1001/jamapediatrics.2017.1736
An excerpt from abstract:
Results Of the 16 eligible studies, authors of 8 studies (n = 1120 patients) provided their data sets. All blood markers and fecal calprotectin individually significantly improved the discrimination between pediatric patients with and those without IBD, when added to evaluation of symptoms. The best marker—fecal calprotectin—improved the area under the curve of symptoms by 0.26 (95% CI, 0.21-0.31). The second best marker—erythrocyte sedimentation rate—improved the area under the curve of symptoms by 0.16 (95% CI, 0.11-0.21). When fecal calprotectin was added to the model, the proportion of patients without IBD correctly classified as low risk of IBD increased from 33% to 91%. The proportion of patients with IBD incorrectly classified as low risk of IBD decreased from 16% to 9%. The proportion of the total number of patients assigned to the intermediate-risk category decreased from 55% to 6%.
Conclusions and Relevance In a hospital setting, fecal calprotectin added the most diagnostic value to symptoms compared with blood markers. Adding fecal calprotectin to the diagnostic workup of pediatric patients with symptoms suggestive of IBD considerably decreased the number of patients in the group in whom challenges in clinical decision making are most prevalent.
From: Inflamm Bowel Dis. 2017 Aug 16. doi: 10.1097/MIB.0000000000001202. [Epub ahead of print]
From a recent Gastroenterology & Hepatology –Full Link:
Thanks to John Pohl’s twitter feed for this link that provides recommendations for Adults with IBD.
An excerpt:
G&H What specific resources for vaccinations are available to help gastroenterologists?
FF It is helpful for providers to keep a copy of the Crohn’s and Colitis Foundation’s health maintenance recommendations posted in their office. This 1-page checklist (available at http://www.crohnscolitisfoundation.org/science-and-professionals/programs-materials/ccfa-health-maintenance.pdf) includes all recommended vaccines and also comments on other important health maintenance items, such as screening for cervical and skin cancer, depression, and osteoporosis. In addition, Cornerstones Health has a vaccination checklist (available at http://www.cornerstoneshealth.org/wp-content/uploads/2017/06/Monitoring-and-Prevention-3.10.2017.pdf) that can be downloaded, printed, and placed in each examination room to reinforce the importance of vaccination. Primary care providers as well as gastroenterologists can use these checklists as reminders in their busy practices.
Related blog post:
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.

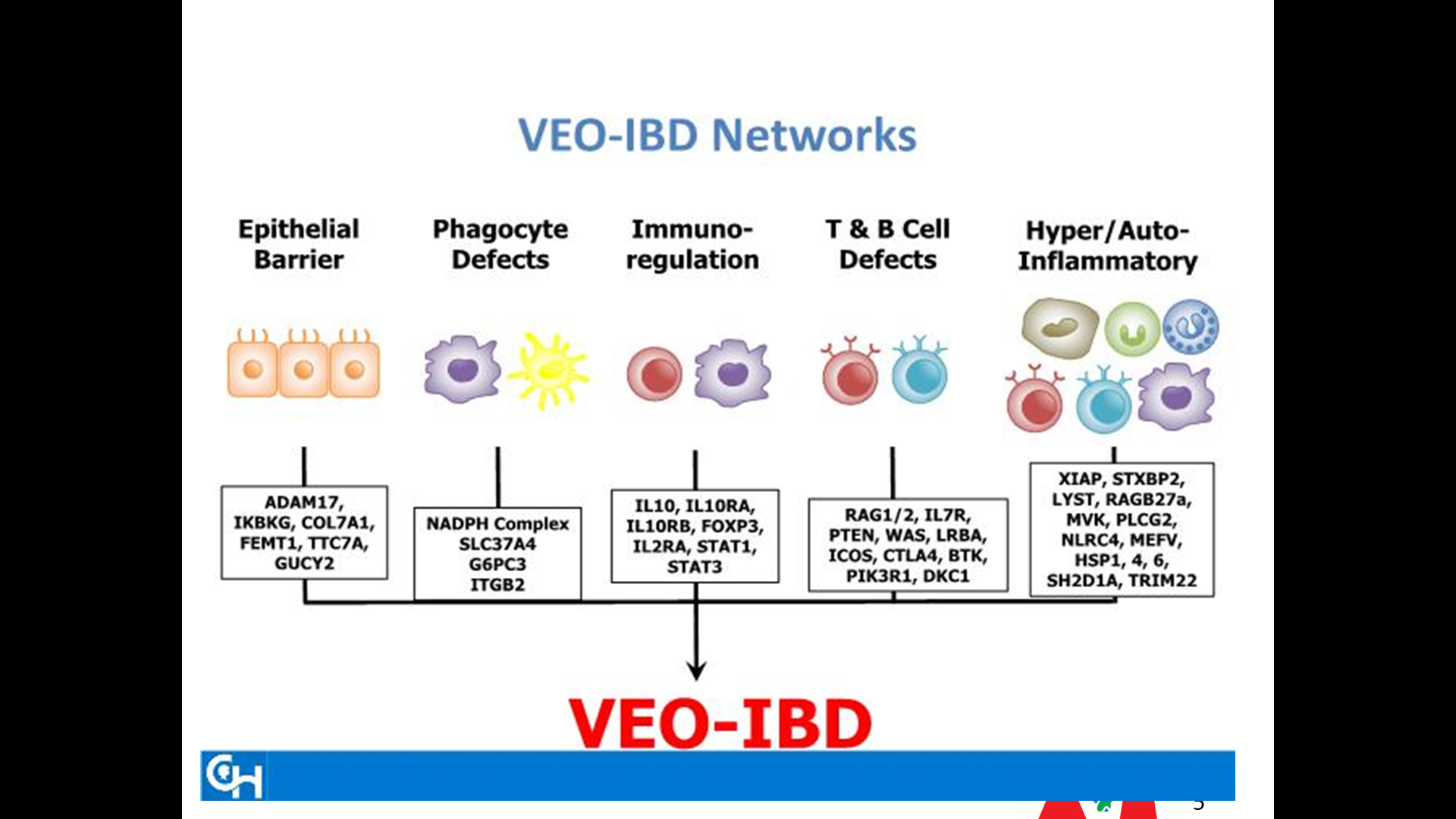
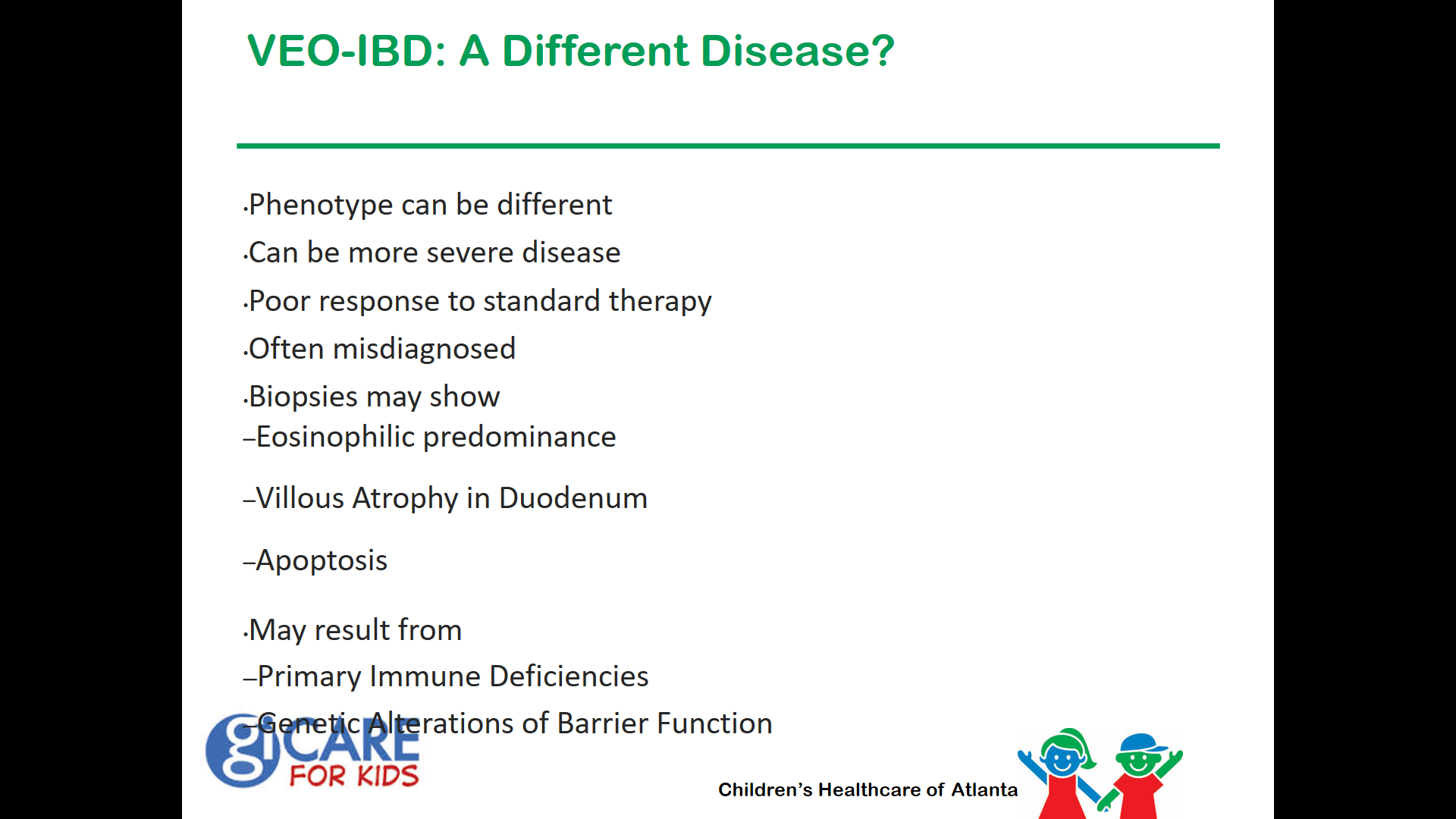
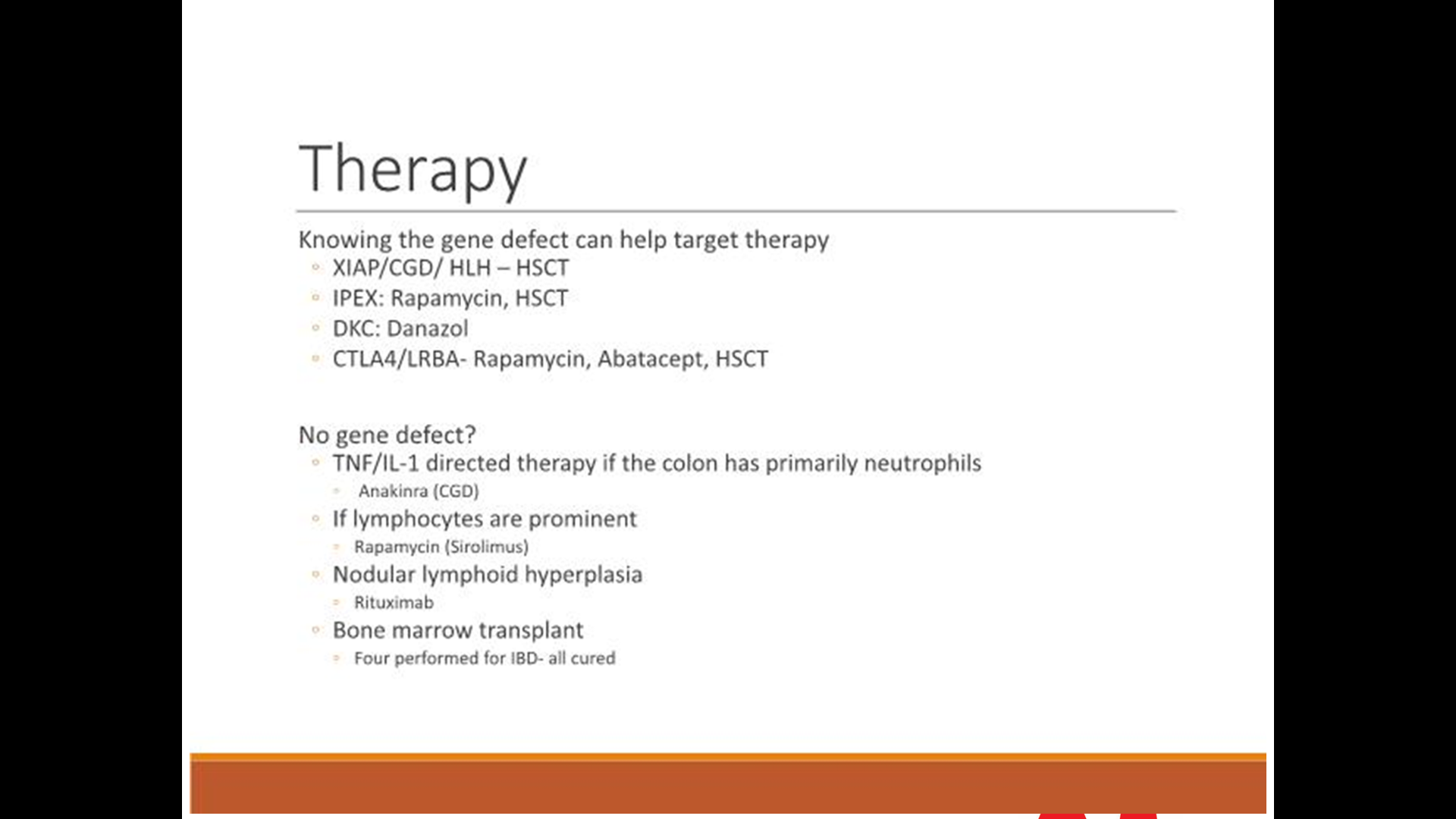
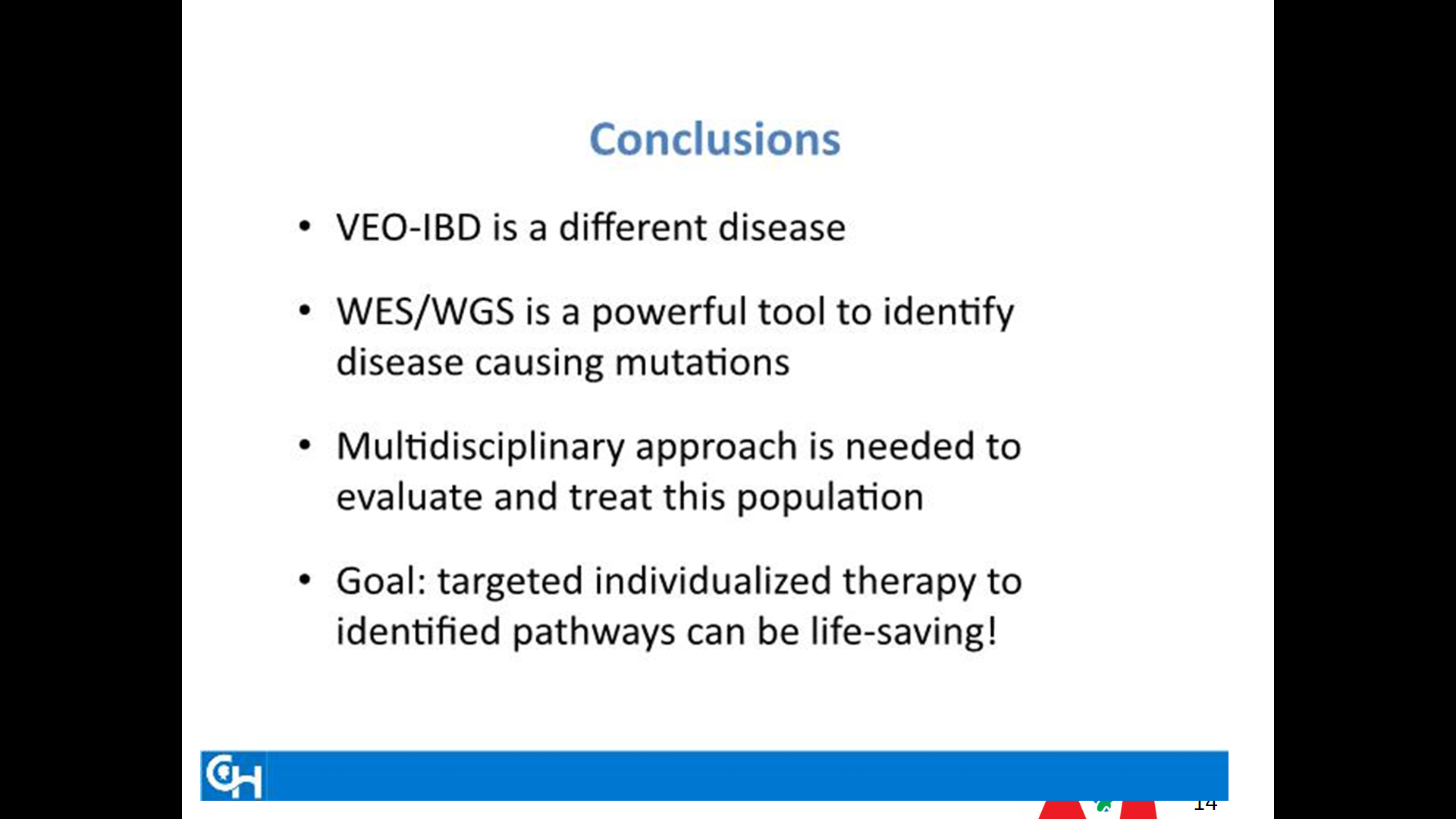
Our recent ImproveCareNow group meeting focused on very early onset IBD. Much of the information has been covered on previous posts, including Patterns and Puzzles with very early onset IBD.
Some of the slides -which at the time of presentation were attributed in part to a recent conference in Philadelphia.






A recent AGA perspectives issue provides two viewpoints on when to start/resume anti-TNF therapy after Crohn’s disease surgery:
Dr. Bressler states that he considers anti-TNF therapy for patients with ongoing immune dysfunction after surgery who are at high risk for recurrence. Attributes of high risk disease include the following:
- younger age (<30 years)
- smoker
- two or more surgeries for penetrating disease.
His commentary indicates that a “‘wait and see’ approach is appropriate for most patients. He frequently will measure a calprotectin three months postoperatively and every three months and perform a colonoscopy typically 6-9 months postoperatively. Those with endoscopic recurrence will be placed on anti-TNF therapy.
Dr. Requiero states:
- The most effective way to prevent recurrence is to initiate an anti-TNF within four weeks of surgery. It has been my practice that patients at high risk for postoperative Crohn’s disease recurrence initiate anti-TNF shortly after they are discharged from the hospital.
- If a patient had been on an anti-TNF prior to the surgery, I will usually resume the same anti-TNF after the surgery. In these patients, I do not give a re-induction course unless they had not received the anti-TNF for more than three months prior to surgery.
- Concomitant therapy: “In the majority of patients, I treat with an anti-TNF, I will use a concomitant immunomodulator…One year after surgery, if there is no disease recurrence, I will decrease and often stop the immunomodulator. With the advent of therapeutic drug monitoring, I have a number of postoperative anti-TNF patients on monotherapy without an immunomodulator.
- [In] patients at moderate risk for postoperative recurrence… I perform an ileocolonoscopy six months postoperatively and, if there is evidence of endoscopic recurrence, I add an anti-TNF agent. After finding a high rate of recurrence in these patients, I am beginning to shift my practice to initiating anti-TNFs in this moderate-risk group as well.
My take: I tend to favor Dr. Reguieiro’s approach in my patient population.
Related blog posts:
August 21, 2017 eclipse (2 days ago) caused unusual shadows:

This shadowing was minutes after the peak eclipse with narrow crescents

This shadowing was a few minutes later and with broader crescents
“Little belly-achers grow up to be big belly-achers and big belly-achers beget little belly-achers” –John Apley
John Apley’s monographThe Child with Abdominal Pains indicates that children with recurrent abdominal pain often grow up to be adults with abdominal pains. A recent study indicates the same type of phenomenon with picky eaters.
A summary of this study in Research Digest: The first study to see if fussy-eating children grow into fussy-eating adults (Thanks to Bonney Reed-Knight for this link.)
An excerpt:
60 per cent of fussy eating children in the study were also fussy eaters at age 23, but fussy eating young adults were no more likely to report signs of eating disorder than their non-fussy peers.
The researchers led by Meredith Van Tine at Stanford University School of Medicine managed to catch up with 61 individuals, now aged 23, who’d participated as children in a long-running study in which their eating habits had been scored by their parents at ages 2, 7, 9.5 and 11, including any signs of fussy eating (being a “selective eater”, having strong likes and dislikes, and only eating a limited variety of foods etc). The participants were now asked to rate themselves on whether they were selective or fussy eaters, and they answered questions about whether they engaged in behaviours related to eating disorders.
Related blog posts:

A personal pet peeve is having to explain to so many parents that their child is not constipated. The typical scenario is that their child went to the ER for abdominal pain and had an abdominal radiograph (AXR); then, the parents are informed that their child is constipated based on ‘fecal loading’ noted on the AXR. In this scenario, it is common for the child to have the following:
- regular bowel movements
- lack of a rectal exam
- lack of improvement with laxatives (though some do improve, perhaps due to the fact that symptoms often have regression to the mean)
- often a normal AXR when interpreted by radiologist rather than ED physician (it is normal to have some stool in the colon)
So, I like to see publications that support my viewpoint that this approach is misguided. Two recent studies provide some insight into this topic:
- SB Freedman et al. J Pediatr 2017; 186: 87-94
- CC Ferguson et al. Pediatrics 2017; 140 (1):e20162290 (thanks to Ben Gold for this reference)
Freedman et al performed a retrospective cohort study (children <18 yrs) who were diagnosed with constipation at 23 EDs from 2004-2015. This study used the PHIS database. Key findings:
- 185,439 of 282,225 had AXR at index ED visit
- Revisits to ED occurred in 3.7%
- 0.28% returned with a clinically important alternate diagnosis, most commonly appendicitis (34% in this category)
- Children who had AXR were more likely to have a 3-day revisit with a clinically important alternate diagnosis (0.33% vs. 0.17%)
Recognizing that AXRs are “unnecessary and potentially misleading,” Ferguson et al aimed to decrease AXR utilization in low-acuity patients who were suspected of having constipation. Using quality tools, the authors performed four plan-do-study-act cycles which included holding grand rounds, sharing best practices, metrics reporting, and academic detailing. Key finding:
- Over 12 months, we observed a significant and sustained decrease from a mean rate of 62% to a mean rate of 24% in the utilizaiton of AXRs in the ED for patients suspected of having constipation.
My take: These studies support my view that routine use of AXR in the diagnosis of constipation is a mistake and can be misleading.
Related blog posts:
The enthusiasm for probiotics is generally greater than expected based on the data available to support their use for many indications. This has been discussed several times on this blog (see below). The reasons why probiotics are sometimes not effective can be related to being poorly regulated/lack rigorous production standards; even in conditions in which there is some effectiveness (eg. antibiotic-associated diarrhea [AAD]), the number of persons needed to treat for one person to benefit is fairly high. Furthermore, as a recent study (A Olek et al. J Pediatr 2017; 186: 82-6) shows, even in conditions like AAD in which probiotics have proven efficacy, the effects may be strain-specific and/or dose-related.
Olek et al showed that Lactobacillus planatarum DSM9843 (LP299V) was NOT beneficial compared to placebo in reducing the incidence of loose/watery stools or mean number of stools among 438 children receiving outpatient antibiotic therapy.
Specifics: This was a prospective, double-blind, randomized, placebo-controlled parallel-group study. The treatment group received LP299V during antibiotic therapy and for 1 week afterwards. In addition to monitoring the number of stools, the authors determined the frequency of AAD which they defined according to WHO guidelines (>3 loose/watery stools/24 hours after initiation of antibiotics). In this study, AAD was confined to study duration rather than over 2 months.
- Overall, 44.5% of children developed loose/watery stools among placebo group and 39% among probiotic group
- 4.1% developed AAD among placebo group and 2.8% among LP299V
- LP299V showed no significant beneficial effects in reducing AAD or loose/watery stools
The authors note that LP299V has been effective in studies involving adult hospitalized patients. They question whether healthy children, therefore, may be less likely to benefit from probiotics and whether a higher dose could have been more effective.
My take: “Data from clinical studies on probiotics are conflicting” for many conditions, including antibiotic-associated diarrhea.

Lovers Leap, near Ashville (Appalachian Trail)
Related blog posts:
Our hospital switched to a new rectal suction biopsy device. This ~ 9 minute YouTube video, rbi2 rectal suction, explains how it is assembled and provides pointers on its use –thanks to Steven Liu for this link.

I have no financial stake in this product.