A recent study (SJ Ott et al. Gastroenterol 2017; 152: 799-811) followed 5 patients who were treated with a sterile fecal filtrate (via nasojejunal tube) for recurrent Clostridium difficile infection (CDI) for a minimum of 6 months. This open-label study noted that this fecal filtrate transfer eliminated the symptoms of CDI in all 5 patients.
A summary of this important study is available in the AGA blog:
Here’s an excerpt: What is the Active Ingredient in FMT for CDI?
Stool was collected from 5 donors selected by the patients and fully characterized according to FMT standards. The stool was then sterile filtered to remove small particles and bacteria, and the filtrate was transferred to patients in a single administration via nasojejunal tube.
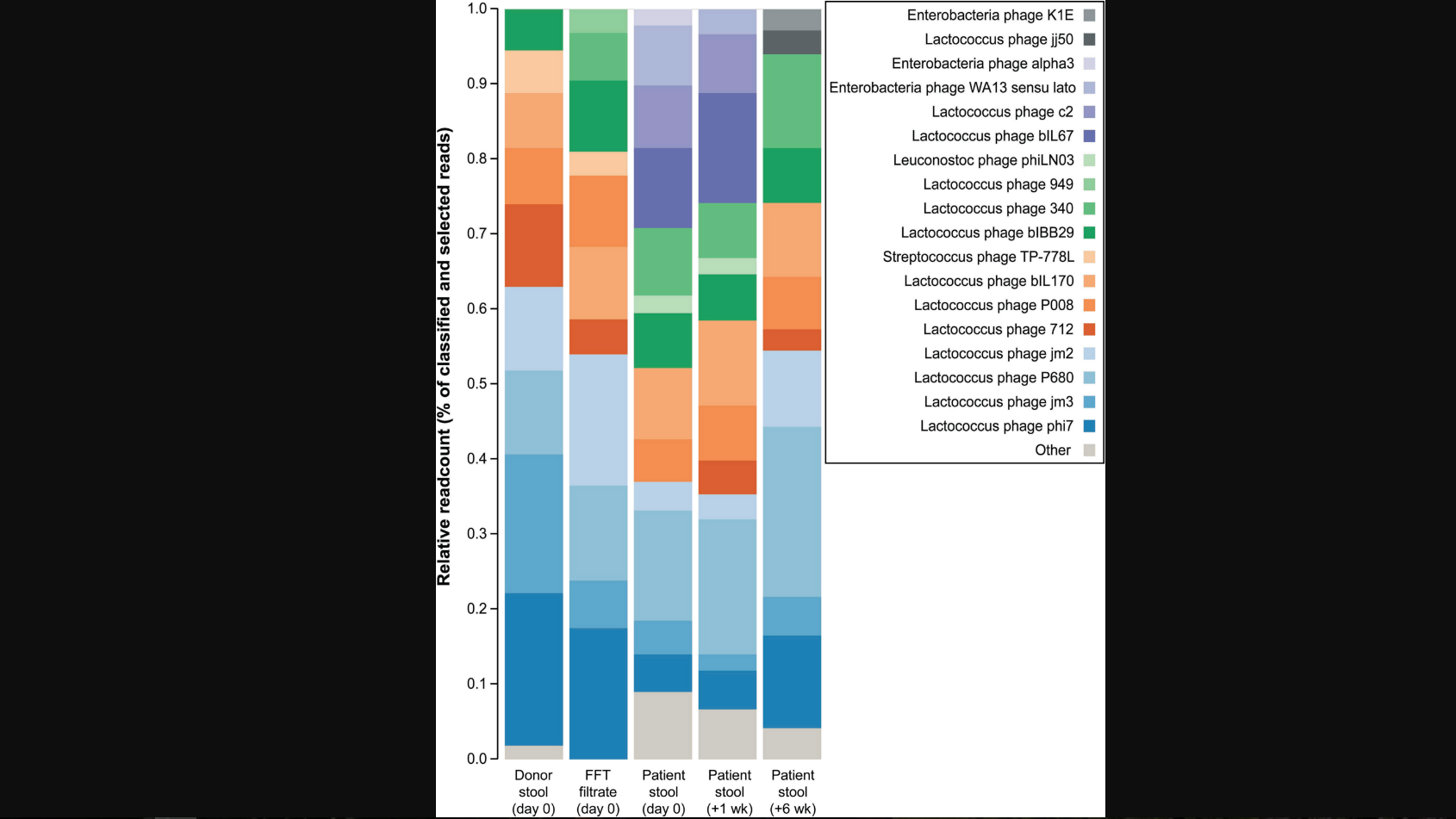
Fecal samples were collected from patients before and at 1 week and 6 weeks after FFT. Microbiome, virome, and proteome profiles of donors and patients were compared….
They identified about 300 different proteins in each of the filtrates they analyzed—most proteins were of human origin, but the filtrates also contained 20–60 bacterial and fungal proteins. The major human proteins in the filtrate proteome were human enzymes such as intestinal-type alkaline phosphatase, chymotrypsin-like elastases, and α amylases. Bacterial proteins included metabolic enzymes and redox proteins without obvious microbiome-modifying properties, such as glyceraldehyde-3-phosphate dehydrogenase, phosphoenolpyruvate carboxykinase, glutaredoxin-1, or thioredoxin-1…
Ott et al propose that the active component of FMT therapy might not be living bacteria, but bacterial components, antimicrobial compounds of bacterial origin (bacteriocins), or bacteriophages that contribute to a healthy intestinal microenvironment. These could be common to all successful FMT therapies and even rather unspecific regarding the bacterial strain(s) used for therapies. They propose that bacteriophages affect community dynamics of gut microbiota to resolve dysbiosis.
My take: This is a provocative study that challenges us to rethink how FMT works. Ultimately, treating CDI needs to be more precise.
Related blog posts: