This satire is particularly amusing for those who have watched “The Pitt.” Unfortunately, many of the health care policy changes under this administration will cause harm here and throughout the world for decades.
“Direct-to-consumer gut microbiome tests produced markedly different results — even when analyzing the same stool sample, researchers found.
Identical fecal samples sent via 21 home-testing kits to seven anonymized direct-to-consumer testing companies yielded a wide variation in reported bacterial abundance and in the health assessments generated from those data, reported Stephanie L. Servetas, PhD, of the National Institute of Standards and Technology (NIST) in Gaithersburg, Maryland, and colleagues in Communications Biology.
In some cases, there was not even agreement among kits produced by the same company…
When researchers compared 18 commonly reported microbial genera across companies, no single provider aligned with the consensus profile for all 18. Across the full dataset, 1,208 unique taxa were reported, but only three genera appeared in every company’s results…
The authors said the discrepancies likely stem from differences in sample processing, sequencing methods, bioinformatics pipelines, reference databases, reporting thresholds, and quality control standards…
“These tests have become popular, partly because people, I think, are increasingly interested in health and wellness, and partly because the gut microbiome has been linked — at least in the public imagination — to the idea that you can improve a whole range of conditions through diet and lifestyle changes,” said co-author Diane Hoffmann, MS, JD, of the University of Maryland in Baltimore.
“There’s been a lot of hype around that, but the hype doesn’t really match the evidence. These tests often have limited evidence behind them, especially when it comes to informing clinical decisions or even basic dietary recommendations,” she added. “So the marketing can be questionable, and consumers can end up misinterpreting or over-trusting results that aren’t very reliable.”
Related article from Houston Methodist Hospital (2024): Should You Do a Gut Microbiome Test?Key point: “While these tests seem to be effective in mapping the gut microbiome, there is currently no benchmark for what a ‘normal’ gut microbiome looks like. So the question becomes what to do with the results…microbiomes are highly variable — even normal, healthy ones. This makes it incredibly challenging to define the patterns or signatures that suggest a microbiome has become imbalanced. Plus, the at-home steps for correcting microbiome imbalance aren’t established either.”
My take: It is uncomfortable informing families that these gut microbiome tests have little clinical value because there is not a proper way to interpret the results. In addition, this study shows that the tests from one place to another produce wildly different results.
While one’s microbiome is important, we still don’t understand what exactly is a normal microbiome.
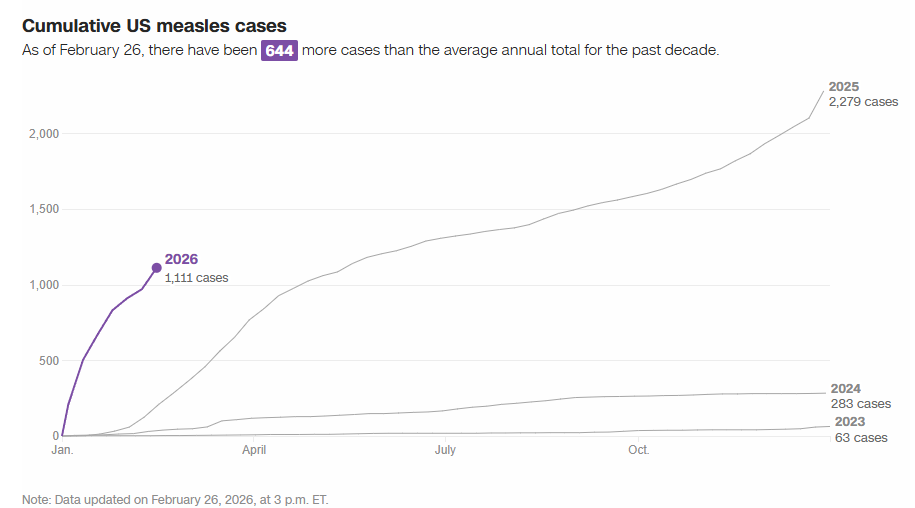
“According to the CDC, out of every 1,000 children who are infected with measles, one may develop encephalitis, which is a dangerous swelling of the brain. Up to 3 out of every 1,000 infected children will die.
The US is on track for another record-breaking year for measles: The number of measles cases reported in the first eight weeks of the year — 1,136 as of February 26, according to CDC data — is already six times more than typical for an entire year. A tracker from the Johns Hopkins University Center for Outbreak Response Innovation has tallied an even higher the annual case total than the CDC…
New measles cases have started to slow in South Carolina in recent weeks…[due to] ublic health groundwork that has helped rapidly identify cases and potential exposures and drive quarantine guidance…Improving vaccination coverage has also helped, she said. The state health department administered nearly 17,000 MMR vaccines in January, which was one of the most successful months for vaccination that the state has had in years.
A new study published Monday provided a sobering look at whether A.I. chatbots, which have fast become a major source of health information…
The experiment found that the chatbots were no better than Google — already a flawed source of health information — at guiding users toward the correct diagnoses or helping them determine what they should do next. And the technology posed unique risks, sometimes presenting false information or dramatically changing its advice depending on slight changes in the wording of the questions…
But Adam Mahdi, a professor at the Oxford Internet Institute and senior author of the new Nature Medicine study, suspected that these clean, straightforward medical questions were not a good proxy for how well they worked for real patients…
So he and his colleagues set up an experiment. More than 1,200 British participants, most of whom had no medical training, were given a detailed medical scenario, complete with symptoms, general lifestyle details and medical history. The researchers told the participants to chat with the bot to figure out the appropriate next steps, like whether to call an ambulance or self-treat at home. They tested commercially available chatbots like OpenAI’s ChatGPT and Meta’s Llama.
The researchers found that participants chose the “right” course of action — predetermined by a panel of doctors — less than half of the time…They were no better than the control group, who were told to perform the same task using any research method they would normally use at home, mainly Googling…
Participants didn’t enter enough information or the most relevant symptoms, and the chatbots were left to give advice with an incomplete picture of the problem…By contrast, when researchers entered the full medical scenario directly into the chatbots, they correctly diagnosed the problem 94 percent of the time…
Even when researchers typed in the medical scenario directly, they found that the chatbots struggled to correctly distinguish when a set of symptoms warranted immediate medical attention or non-urgent care.
My take: AI and chatbots can be quite helpful and continue to improve. This study and the summary by NY Times show some of the limitations. Even small changes in wording/prompts can alter the advice from chatbots considerably.
DB Kramer et al. NEJM 2026; 394: 402-407. Promoting Fairness in Screening Programs for Late-Career Practitioners
This is an interesting article regarding screening late-career physicians (LCPs) to assure competency.
An excerpt:
Late-career physicians (LCPs) are an integral part of the U.S. medical workforce. Nearly a quarter of practicing physicians in the United States are over 65 years of age, and they are serving at a time of overall physician scarcity.1,2 Older physicians bring valuable wisdom and expertise to patient care, but many will experience cognitive and physical decline that may affect their clinical skills.3,4 Interest has grown among hospitals in mandatory screening programs that could proactively identify physicians whose ability to deliver safe care may be compromised, before patient harm occurs.5…
Yet physicians also have interests related to being screened that deserve respect, and LCP programs can and should protect these interests by ensuring procedural fairness…
Evidence that LCPs can pose risk to patients has motivated health care institutional leaders to develop mandatory screening programs.5,12 LCP policies may require testing of the aspects of physicians’ cognitive and physical functioning that are relevant to clinical activities; such testing is usually triggered when a physician reaches an age threshold (commonly 70 years) and is tied to renewal of privileges….Among physicians’ objections are that tests have imperfect predictive accuracy and that erroneous results could threaten their reputation and livelihood…
Fair assessment requires that the screening tests and processes employed provide an accurate, impartial assessment of relevant skills. An appeals process should be developed that gives physicians a meaningful opportunity to contest any restrictions on their privileges based on test results. Physicians who participate in LCP programs, like employees in other industries, retain recourse to the Equal Employment Opportunity Commission and the courts to contest wrongful termination, age discrimination, and disability discrimination…
The other key component considered by courts evaluating individual burden is known as least infringement. In the context of LCP programs, such an inquiry would center on whether an adverse action taken on the basis of test results is the least-restrictive option that is commensurate with the goal of protecting patient safety…
Care should be taken not to mistakenly hold LCPs to a higher standard than younger physicians simply by applying greater scrutiny to their practice.26
My take: In theory, screening of late-career physicians makes a lot of sense to protect patient welfare. In practice, it may be difficult to design tests that have adequate sensitivity and specificity with regard to physician capability. This is true for both older and younger physicians.
Danish residents with elevated lipids and CVD risk factors who were taking statins for CVD prevention saw a 16% lower risk per unit time of incident IBD, the researchers found (AS Faye et al. J Intern Med 2025;298[6]:686-696. Statin use for primary prevention of cardiovascular disease reduces the risk of incident IBD: A population-based cohort study)…
The study was a population-based, prospective cohort design drawing on the Danish National Registries. Participants were over 40 years of age and had undergone low-density lipoprotein (LDL) measurement between 2008 and 2022…Each of 110,961 people who picked up statin prescriptions within six months of LDL measurement was matched to five others (n=554,805) not prescribed statins by age, sex, calendar year, and CVD risk factors…
The aHR of developing IBD for statin users versus nonusers was 0.84 (95% CI 0.72-0.97)…The five-year number needed to treat (NNT) with statins was 2,881 to prevent one additional IBD case…
In addition to lipid-lowering properties, statins have anti-inflammatory and immunomodulating actions.
My take: This study suggests that statins have an “off target” beneficial effect in reducing the risk of inflammatory bowel disease. However, it is possible that statin use is not directly beneficial but an epiphenomenon. For example, individuals taking statins may have modified their diet to lower their risk as well.
Background: “Lynch syndrome (LS) is a prevalent hereditary cancer syndrome affecting ~1 in 300 individuals, with an overall lifetime cancer risk as high as 80%. LS is caused by germline mutations in the DNA mismatch repair genes, leading to microsatellite instability (MSI) and accumulation of shared mutations. When these occur in coding regions, they generate frameshift peptides (FSPs). Nous-209 is a neoantigen-directed immunotherapy” against these FSPS. These are “the results from cohort 1 of a phase 1b/2 single-arm trial of Nous-209 for cancer interception in LS carriers (n = 45).”
Key findings:
Neoantigen-specific immune responses were observed after vaccination in 100% of evaluable participants (n = 37), with induction of potent T cell immunity
The immune response was durable and detectable at 1 year in 85% of participants
Both CD8+ and CD4+ T cells were induced, recognizing multiple FSPs
Peptide–human leukocyte antigen predictions allowed the identification of >100 immunogenic FSPs with demonstration of cytotoxic activity in vitro
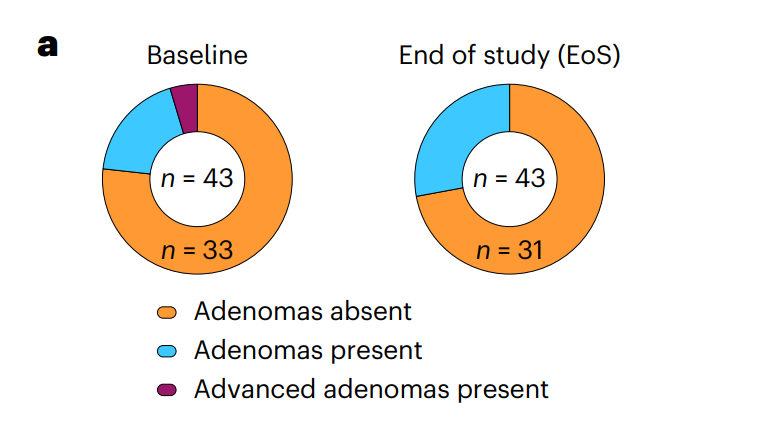
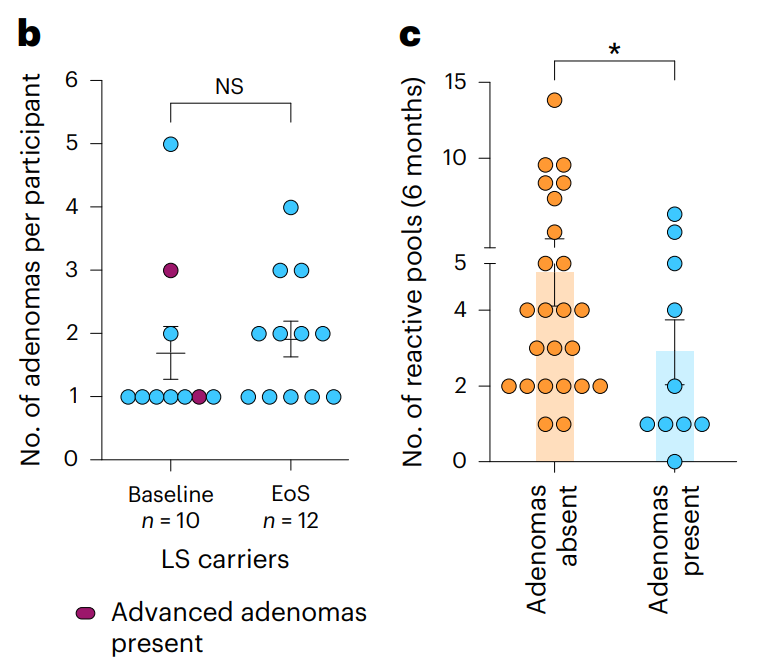
Colorectal neoplasia burden observed at end-of-study colonoscopy inversely correlates with breadth of immune response. a, Number of participants who underwent screening colonoscopy at baseline and end of study (EoS; n = 43) who had no adenomas (adenomas absent), at least one adenoma (adenomas present) and advanced adenomas (advanced adenomas present) detected.b, Number of adenomas per trial participant at baseline and end of study; comparison of baseline versus EoS was performed using a two-tailed Mann–Whitney U-test; NS, not significant. c, Number of reactive pools measured at 6 months (n = 34 evaluable subjects) between the participants with and without adenomas. Data are shown as the mean ± s.e.m.
My take (borrowed in part from authors): “Overall, this clinical trial provides important proof-of-concept data of the safety and the robustness of induced immunogenicity of Nous-209 in LS carriers…and supporting its clinical development as a valuable intervention for cancer immune interception.” Vaccines have a long history in reducing cancer (for Hepatitis B, Cervical Cancer (due to HPV), Anal Cancer, Leukemia (by boosting immunity) and Others). Until recently, this has been by preventing viral infections that increase the risk of cancer. This is a new approach.
Related article: Blood test for colorectal cancer: A Mannucci et al. Gastroenterol 2026; 170: 330-343. An Exosome-Based Liquid Biopsy for the Detection of Early-Onset Colorectal Cancer: The ENCODER Multicenter Study Methods: A panel of 6 cell-free and exosome-based circulating biomarkers were identified through small RNA sequencing from a biomarker discovery cohort (blood test). Key finding: “This study developed and independently tested a blood-based test with 97.3% sensitivity for screening-relevant CRC stages I–III and 61.5% for the noninvasive detection of high-grade dysplasia.”
RM Califf et al. N Engl J Med 2026;394:4-6. A Threat to Evidence-Based Vaccine Policy and Public Health Security at the FDA
This editorial by 12 former FDA commissioners of both Democratic and Republican administrations is sharply critical of recent policy changes at the FDA which threaten the supply of life-saving vaccines.
Here is an excerpt:
“The existing regulatory model builds public trust by encouraging open information exchange and rigorous, transparent scientific debate. Yet a memo sent last week to FDA staff will upend core policies governing vaccine development and updates…
The memo (available at https://www.biocentury.com/article/657740) was written by Vinay Prasad, director of the FDA’s Center for Biologics Evaluation and Research (CBER), who also serves as the agency’s chief scientific officer, chief medical officer, and acting head of CBER’s office of biostatistics, as well as overseeing the division responsible for vaccine review and approval. His memo characterizes the actions of FDA scientists who express concerns about agency processes or decisions to outside parties as “unethical” and “illegal.” It calls for scientific debates to be kept within the agency “until they are ready to be made public,” and instructs staff members who disagree with the new framework to “submit your resignation letters.”..
If enacted, the framework would impede the ability to update vaccines to keep up with the natural evolution of respiratory viruses or changes in the prevalence of bacterial serotypes…
The new framework rejects the agency’s long-standing reliance on “immunobridging” studies for well-understood vaccines with extensive safety data. Using this approach, once a reliable correlation with effectiveness has been established, a vaccine’s ability to stimulate the immune system to produce protective antibodies can serve as a surrogate for its efficacy in helping patients avoid infections and complications from rapidly evolving viruses such as SARS-CoV-2 and influenza. Because these viruses change frequently, repeating large-scale efficacy trials for every new seasonal strain is not feasible within the time needed to update the vaccines…
Abandoning the existing methods won’t “elevate vaccine science,” as the memo asserts. It will subject vaccines to a substantially higher and more subjective approval bar. The proposed measures will slow the replacement of older products with better ones and will create potentially prohibitive expenses for new market entrants…Moreover, insisting on long, expensive outcomes studies for every updated formulation would delay the arrival of better-matched vaccines when new outbreaks emerge or when additional groups of patients could benefit…
The new approach would also evade public transparency, including long-standing statutory and regulatory mechanisms that enable disagreements about benefit–risk balance, clinical trial end points, trial design, and data analysis to be aired in public…
The benefits and risks of many established vaccines are well understood, and imposing the new approval requirements without meaningful new evidence could make it impossible to keep up with evolving infectious threats.
The memo asserts, incorrectly, that “we do not have reliable data” on the benefits of Covid vaccination in children. Reasonable scientists should engage in open debate about how best to shape recommendations for children at lower risk for Covid-19, but substantial evidence shows that vaccination can reduce the risk of severe disease and hospitalization in many children and adolescents…
Americans’ safety depends on a culture in which evidence is reviewed openly and staff can surface concerns, challenge leadership, and engage with external scientists without fear of reprisal.
In a nearby neighborhood, my wife and I went walking and came across a “free art” stand which looked similar to a “free little library” stand. We picked out this small piece (about 5 inches on each side).
Last week, the following article explained why the newest changes, announced yesterday (see link below), to the vaccine schedule recommendations are not a good idea:
“Proponents of the push to align U.S. recommendations with those of so-called peer nations such as Denmark, Japan and Germany — all of which recommend fewer shots than the United States — have billed it as a common-sense corrective. But, as innumerable doctorsandscientists have explained, when it comes to public health, countries with fewer shots on their must-have list are not actually our peers.
In Denmark, to take the administration’s favorite example, prenatal care is free and universal. More than 95 percent of pregnant women are screened for hepatitis B, and those who test positive are promptly treated and duly monitored…
None of this is true in the United States.
Here, nearly a quarter of pregnant women lack adequate prenatal care, and those who face the highest risk of contracting and spreading vaccine-preventable diseases are often the least likely to have access to doctors or pharmacies. When U.S. health officials tried to stamp out hepatitis B through vaccination programs aimed at high-risk groups, they failed miserably. It was not until they carried out a universal, at-birth vaccination policy in 1991 that hepatitis B infections finally plummeted — by about 99 percent.
In fact, if the U.S. public health system has one thing going for it relative to other nations, it’s probably vaccines. As the C.D.C.’s own data indicates, routine childhood vaccination has prevented hundreds of millions of illnesses and tens of millions of hospitalizations here. It has also saved half a trillion dollars in medical costs, a figure that jumps into the multitrillions once you factor in indirect, societal costs like lost productivity and lost wages.
The United States tends to have higher rates of measles vaccination than Europe, and fewer measles cases as a result. Compared with Denmark, we also tend to have lower hospitalization rates for rotavirus (which causes diarrhea and can be fatal in infants and children) and respiratory syncytial virus, or R.S.V. (which is a leading cause of hospitalization among children). The reason for those disparities is not in dispute: We vaccinate routinely against both viruses. Denmark does not…
In the meantime, the Food and Drug Administration is angling to make an even bigger and more enduring impact on Americans’ access to vaccines…top officials at the agency have proposed a roster of new requirements for the shots, including several that critics say would be logistically impossible and could leave us with no F.D.A.-approved Covid or flu vaccines…
We don’t have to wonder what that future will look like. We can glimpse it already in communities across the country where measles and whooping cough are resurgent and where infants and young children have already died from both. We can also see it foretold in the current flu season: This year’s flu vaccine has proved an imperfect match to the currently circulating strains. New shots, based on mRNA technology, would have one day enabled us to avoid this kind of misfire. But the nation’s leaders have imperiled that future with the decisions they made this year…
Mr. Kennedy has brought us to this precipice by aggressively subverting nearly every process and protocol that previously governed our public health institutions. He has granted political appointees enormous sway over agency scientists. He has excluded people with meaningful expertise from his planning and deliberations. And he has fired dissenters all the way up to the C.D.C. director and replaced them with lackeys, sycophants and wellness grifters.”
My take: RFK Jr and this administration has already done great damage to our health care and the toll will be evident for a long time. But, they are not done yet.
Link to yesterday’s announcement: NY Times 1/05/25: Kennedy Scales Back the Number of Vaccines Recommended for Children“Public health experts expressed outrage at the sweeping revisions, saying federal officials did not present evidence to support the changes or incorporate input from vaccine experts…and will endanger the health of children in the United States…The C.D.C.’s new schedule continues to recommend vaccines against some diseases, including measles, polio and whooping cough, for all children. Immunization against six other illnesses — hepatitis A, hepatitis B, meningococcal disease, rotavirus, influenza and respiratory syncytial virus, the leading cause of hospitalization in American infants — will be recommended for only some high-risk groups or after consultation with a health care provider.”
This article focuses on the experience of a transgender patient who recorded unfavorable remarks while under anesthesia.
An excerpt:
On the recording, the health care workers express a variety of opinions about transgender identity more generally….And in the middle of the conversation, one person suggests updating Ms. Capasso’s medical file. “Yeah, it needs to say ‘male,’” the person says.Ms. Capasso said it appeared that hospital staff had in fact changed her electronic medical records, all while she was unconscious…
Ms. Capasso insists that she was not trying to catch the medical staff speaking disrespectfully about her. She said she was motivated by curiosity and a desire to know exactly what the surgeons discovered. It may not be such an unusual impulse.
Dr. Alexander Langerman, a surgeon at Vanderbilt University Medical Center, led a medical conference in 2021 on surgical recordings.
There is often “a really strong desire by patients to know what happened to them in the operating room,” Dr. Langerman said. “And, I think, a valid right to know what happened.”
Surgery was once a relatively public event — operating rooms were called “theaters” for a reason. But infection control and malpractice litigation pulled the operating room out of public view.
“Operating rooms and surgery have become one of the most secretive environments in modern society,” said Dr. Teodor Grantcharov, a Stanford University professor who started a company that uses operating room recordings to improve patient safety and hospital efficiency.
My take: While a patient is under anesthesia, it is best to treat them in the same manner as if they were awake.
“The true test of a man’s character is what he does when no one is watching.”