M Barroso et al. Gastroenterol 2018; 154: 2087-96.
Background: “Western-like diets –mainly characterized by high intake of red and processed meats, refined grains, simple sugars, and saturated fats and low intake of fruits, vegetables, and whole grains– have been associated with low-grade chronic inflammation, which is involved in the etiology of inflammatory conditions.” Ref: Br J Nutr 2015; 114: 999-1012.
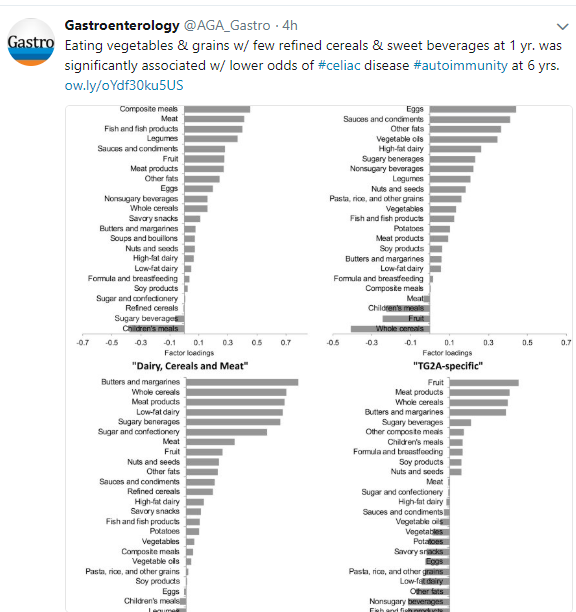
To examine how diet may influence the development of celiac autoimmunity, defined by TG2A positivity, the authors examined a subset of patients (n=1997) from the prospective Generation R study (Netherlands); 27 in this cohort developed celiac autoimmunity (1.4%).
Key finding:
- Higher adherence to a “prudent” diet which had a higher intake of vegetables, vegetable oils, pasta, and grains and low consumption of refined cereals and sweet beverages at 1 year of age was associated with a lower odds of celiac autoimmunity at 6 years of age with an odds ratio of 0.67.
This study is limited by the relatively low number who had celiac autoimmunity and by its use of a food questionnaire.
My take: This study indicates that diet plays a role in the development of celiac along with other disease, but this likely involves a complex mix of components rather than a single toxic agent.
Related blog posts:
- Northern Latitudes -Higher Celiac Disease Rates
- Celiac Disease Epidemic (High rate of celiac disease reported in Denver children)
- Vaccine for Celiac Disease
- Celiac Disease Risk –TEDDY study
- Celiac Disease and Mode of Delivery -Perhaps Not Very Consequential
- Celiac disease and diabetes
- Celiac disease and psychological problems
- How Birth Can Affect Your GI Tract | gutsandgrowth
- How to Protect Children From Celiac Disease
- Why are we seeing so many more cases | gutsandgrowth
- Why is Celiac Disease Becoming More Prevalent?