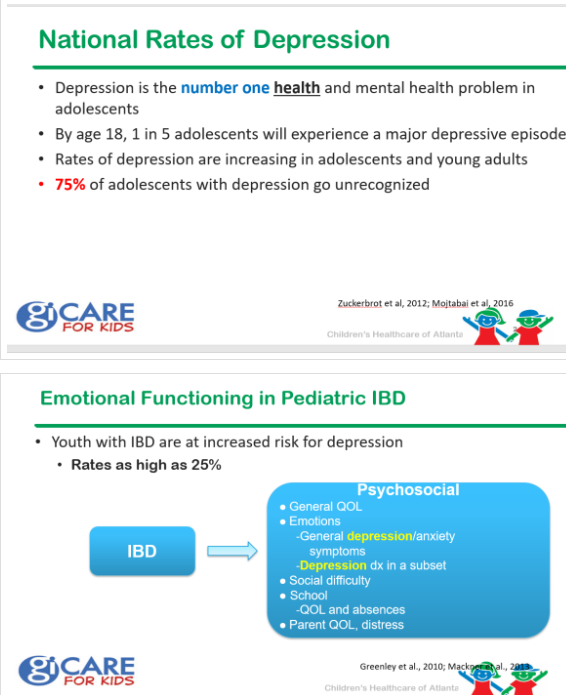
LW Gaines et al. Inflamm Bowel Dis 2020; 26: 423-8. In this study with 3307 adults with Crohn’s disease (CD) and baseline demographics, CD activity and an affective-cognitive index of depression, the authors used structural equation models to determine the likelihood of whether depression triggers CD activity or whether CD activity triggers depression. Key findings: “The hypothesis that an affective-cognitive depression predicts patient-reported exacerbation of CD is 218 times more likely to account for the data than the converse.” (Depression is likely to increase CD activity rather than be due to CD activity).
JJ Ashton et al. Inflamm Bowel Dis 2020; 26: 469-76. Among 256 patients (dx 2013-17) in Southhampton-PIBD database, there were 151 with CD, 95 with UC and 10 IBD-unclassified. Key findings:
- 9% presented with all normal blood tests (tests analyzed if available: CRP, ESR, Albumin, platelets, packed cell volume, wbc, ALT)
- Normal labs were more common with UC compared to CD: 14.4% vs 5.3%
RC Ungaro et al. AP&T; 2020; DOI: 10.1111/apt.15685. (Thanks to Ben Gold for this reference). Systematic review with meta-analysis: efficacy and safety of early biologic treatment in adult and paediatric patients with Crohn’s disease. A total of 18 471 patients were studied, with a median follow-up of 64 weeks (range 10-416). Meta-analysis found that early use of biologics was associated with higher rates of clinical remission (OR 2.10 [95% CI: 1.69-2.60], n = 2763, P < 0.00001), lower relapse rates (OR 0.31 [95% CI: 0.14-0.68], n = 596, P = 0.003) and higher mucosal healing rates (OR 2.37 [95% CI: 1.78-3.16], n = 994, P < 0.00001) compared with late/conventional management. Conclusions: Early biologic treatment is associated with improved clinical outcomes in both adult and paediatric CD patients, not only in prospective clinical trials but also in real-world settings.
RS Boneh et al. Dietary Therapies Induce Rapid Response and Remission in Pediatric Patients With Active Crohn’s Disease Clin Gastroenterol Hepatol (online April 14, 2020, in press) Thanks to KT Park’s Twitter feed for this reference.
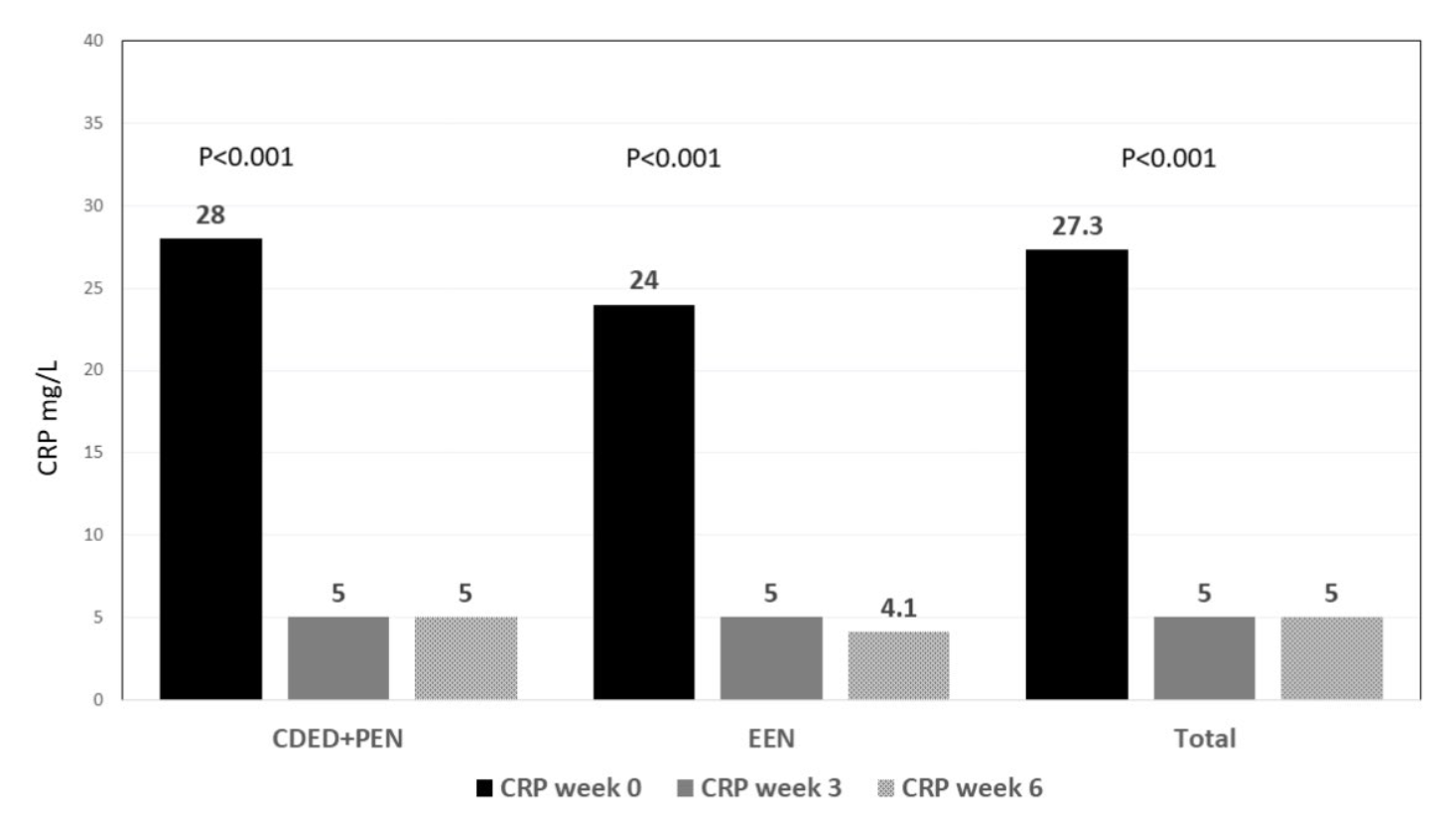
- Methods: We collected data from the multicenter randomized trial of the CD exclusion diet (CDED). We analyzed data from 73 children with mild to moderate CD (mean age, 14.2±2.7 y) randomly assigned to groups given either exclusive enteral nutrition (EEN, n=34) or the CDED with 50% (partial) enteral nutrition (n=39). Patients were examined at baseline and at weeks 3 and 6 of the diet. Remission was defined as CD activity index scores below 10 and response was defined as a decrease in score of 12.5 points or clinical remission. Inflammation was assessed by measurement of C-reactive protein.
- Results: At week 3 of the diet, 82% of patients in the CDED group and 85% of patients in the EEN group had a dietary remission (DiRe). Median serum levels of C-reactive protein had decreased from 24 mg/L at baseline to 5.0 mg/L at week 3 (P<.001). Among the 49 patients in remission at week 6, 46 patients (94%) had a DiRe and 81% were in clinical remission by week 3. In multivariable analysis, remission at week 3 increased odds of remission by week 6 (odds ratio, 6.37; 95% CI, 1.6–25; P=.008) whereas poor compliance reduced odds of remission at week 6 (odds ratio, 0.75; 95% CI, 0.012–0.46; P=.006).
- Conclusions: For pediatric patients with active CD, dietary therapies (CDED and EEN) induce a rapid clinical response (by week 3).
Related blog posts:
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition