Lately, I’ve been shocked and dismayed by the frequent headlines about the number of overdoses and deaths due to narcotics throughout our country. A timely article (RG Frank, HA Pollack. NEJM 2017; 376: 605-7) addresses one aspect of this threat to public health that I was not aware of previously.
- Fentanyl, which is a powerful synthetic opioid, is much cheaper to produce than heroin. In addition, fentanyl can result in death much more quickly as well.
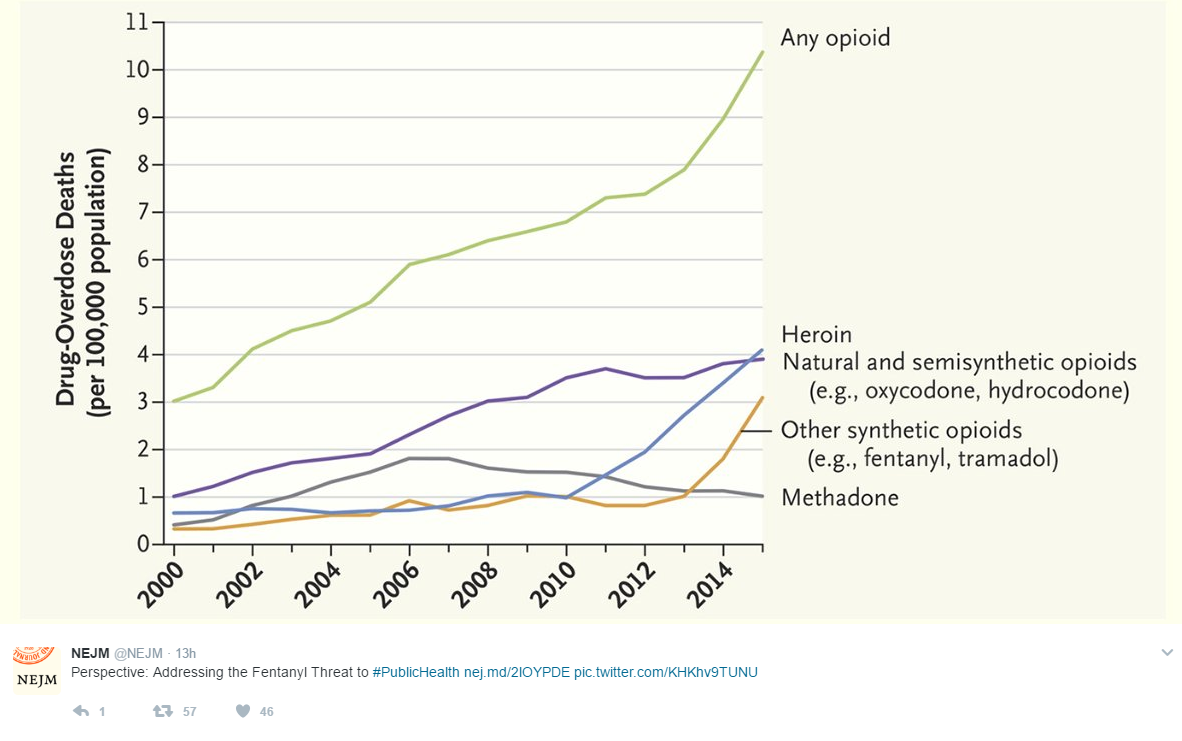
- Presumably due to its lower cost, suppliers ‘cut’ heroin with the drug. As a consequence, fentanyl is increasingly responsible for opioid deaths. The authors estimate that from 2012 to 2014, the number of deaths due to fentanyl doubled to 5544 and that “41% of the roughly 7100 heroin-related deaths during this period involved fentanyl.”
- Fentanyl has been found in multiple counterfeit illicit drugs. For example, in a recent analysis from Canada, “89% of seized counterfeit OxyContin tablets” had fentanyl present.
- Naloxone can reverse fentanyl overdoses but needs to be given more quickly and sometimes multiple doses are needed.
My take: The presence of fentanyl in illicit drugs means that even experimenting once could be fatal.
Related blog posts:
- Trends in Non-medical opioid Use and Heroin Addiction
- CDC Guideline for Prescribing Opioids for Chronic Pain
- Deadly consequences of pain management | gutsandgrowth
- Increased Narcotic Usage in Pediatric Patients with IBD …
- Epidemic of Prescription Drug Overdoses | gutsandgrowth
- Increased Narcotic Usage in Pediatric Patients with IBD