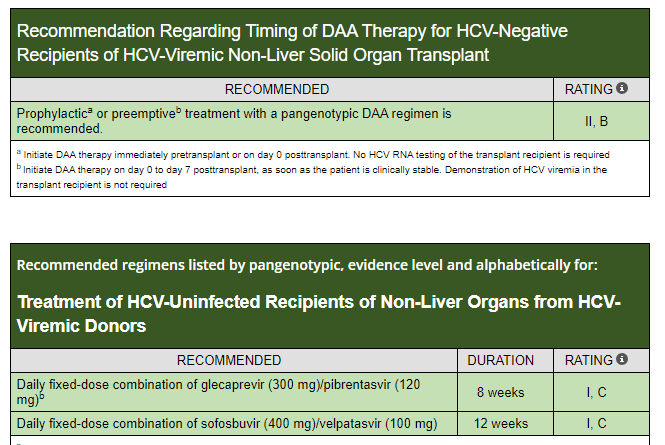
A recent report in Gastroenterology and HepatologyNews (July 2024: Shortened Protocol Can Prevent Infection in Recipients of HCV+ Organs) highlighted the recommended use of 1 week empiric treatment to prevent the development of hepatitis C in transplant recipients of HCV+ organs.
The cost for a one week course of “the Toronto Protocol” which includes glecaprevir-pibrentasvir along with ezetimbe is ~$2800. This is much less than a full course which likely would cost ~$30,000. Ezetimbe, cholesterol-lowering agent, has the ability to prevent HCV from entering cells.
For liver transplant recipients of HCV+ donor, a 12 week course of treatment is recommended
SJ Martinez-Dominguez et al. Inflammatory Bowel Diseases, Volume 30, Issue 8, August 2024, Pages 1274–1283, https://doi.org/10.1093/ibd/izad175 Open Acess! Inflammatory Bowel Disease Is an Independent Risk Factor for Metabolic Dysfunction–Associated Steatotic Liver Disease in Lean Individuals
Methods: This was a cross-sectional, case-control study including 300 lean cases with IBD and 80 lean controls without IBD, matched by sex and age (median age ~45 yrs). All participants underwent a liver ultrasound, transient elastography, and laboratory tests. All patients with current or previous use of systemic steroid in the last 2 years were excluded from the analysis
Key Findings:
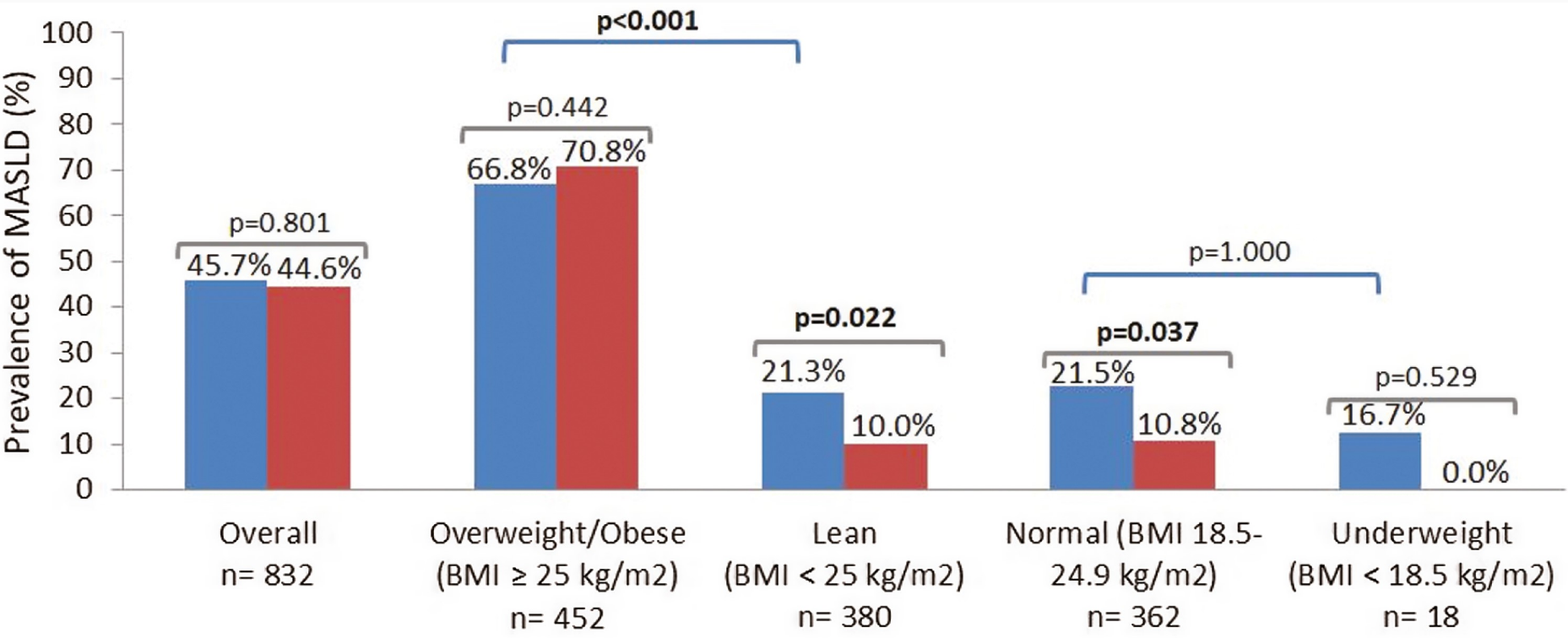
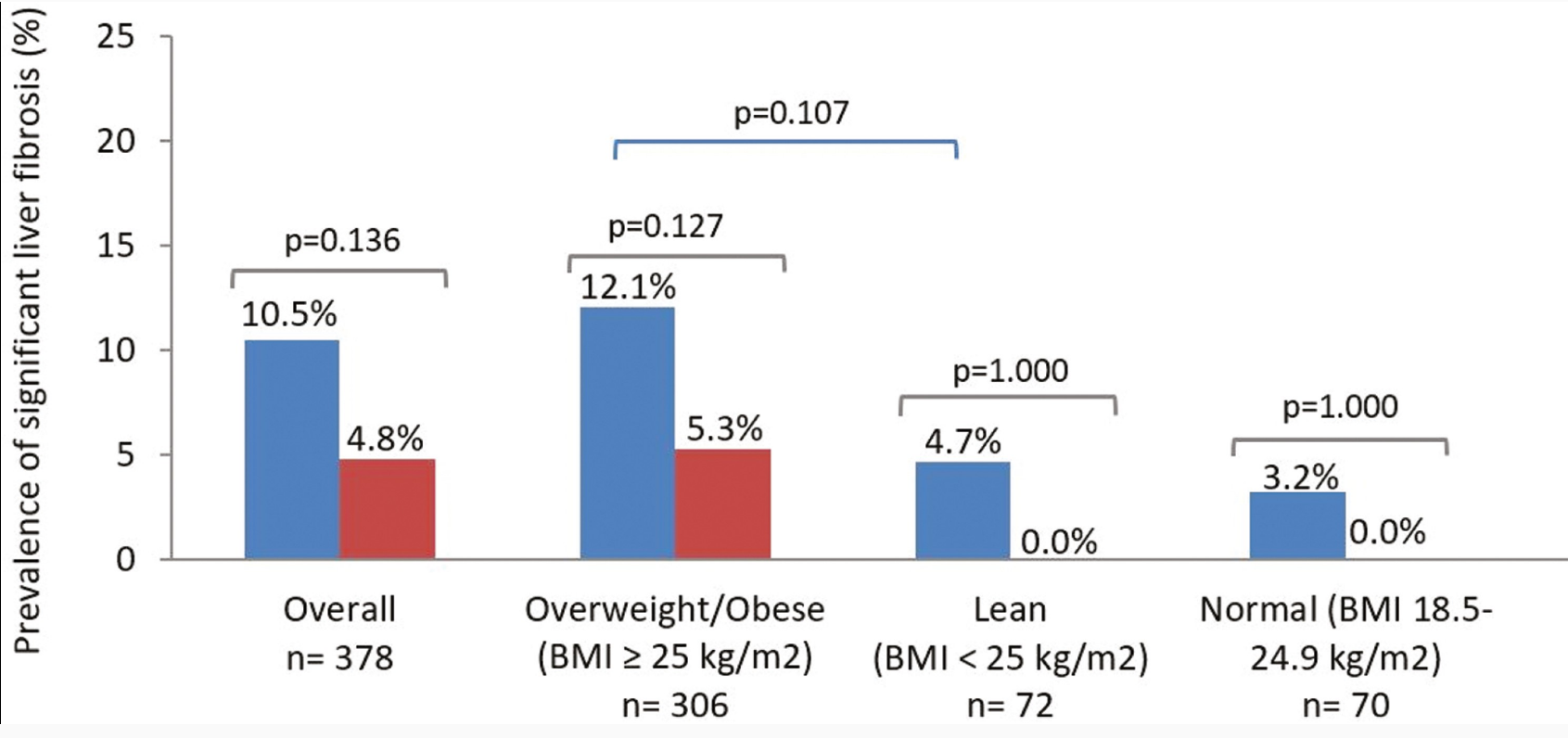
The lean IBD group showed a significantly higher prevalence of MASLD compared with lean non-IBD group (21.3% vs 10%; P = .022), but no differences were observed in the prevalence of significant liver fibrosis (4.7% vs 0.0%; P = 1.000)
No differences were found between the prevalence of MASLD in IBD and non-IBD participants who were overweight/obese (66.8% vs 70.8%; P = .442)
IBD was an independent risk factor for MASLD in lean participants (odds ratio [OR], 2.71) after adjusting for classic metabolic risk factors and prior history of systemic steroid use
Prevalence of metabolic dysfunction–associated steatotic liver disease (MASLD) in cases and controls according to body mass index (BMI) status. Blue bars: cases (inflammatory bowel disease). Red bars: controls (non–inflammatory bowel disease). P values in bold indicate statistical significance (P < .05).
My take: This study suggests that “chronic inflammation could play a role in MASLD development.” Also, this indicates that MASLD could be a reason for elevated LFTs in patients with IBD, even in lean patients.
NE Peters et al. NEJM 2024; 391; 56-59. Normalization of C1 Inhibitor in a Patient with Hereditary Angioedema
“An infant with genetically confirmed hereditary angioedema and low C1 inhibitor levels (but without previous episodes of angioedema) underwent liver transplantation for biliary atresia, an unrelated condition. Liver transplantation led to normalization of the C1 inhibitor level and function. To our knowledge, this represents the first patient to be potentially cured of hereditary angioedema.” This case report shows that liver-directed therapy can reverse hereditary angioedema.
T Asselah et al. NEJM 2024; 391:133-143. Bulevirtide Combined with Pegylated Interferon for Chronic Hepatitis D
Key finding: At 24 weeks after the end of treatment, HDV RNA was undetectable in 17% of the patients in the peginterferon alfa-2a group, in 32% of those in the 2-mg bulevirtide plus peginterferon alfa-2a group, in 46% of those in the 10-mg bulevirtide plus peginterferon alfa-2a group, and in 12% of those in the 10-mg bulevirtide group.
My take: This is a long (48 weeks) and difficult treatment (2 injection meds and lots of peginterferon side effects). However, there is a fairly good response rate.
This link to the article also has links to related AASLD guidelines (eg. management of portal hypertension). Table 2 summarizes the ~34 recommendations which include yearly evaluation with labs, ultrasound at least every 2 years in pediatric patients (age 3 yrs and older) and against routine use of ursodeoxycholic acid.
VG Clark et al. Gastroenterol 2024; (in press). DOI:https://doi.org/10.1053/j.gastro.2024.06.028 Fazirsiran for Adults with Alpha-1 Antitrypsin Deficiency Liver Disease: A Phase 2 Placebo Controlled Trial (SEQUOIA)
Key findings:
At Week 16, least-squares mean percent declines in serum Z-AAT concentration were −61%, −83% and −94% with fazirsiran 25/100/200 mg, respectively, versus placebo (all P< .0001)
Efficacy was sustained through Week 52. At post-dose liver biopsy, fazirsiran reduced median liver Z-AAT concentration by 93% compared with an increase of 26% with placebo
All fazirsiran-treated patients had histological reduction from baseline in hepatic globule burden
Portal inflammation improved in 5/12 and 0/8 patients with baseline score >0 in the fazirsiran and placebo groups, respectively
Histological METAVIR score improved by >1 point in 7/14 and 3/8 patients with fibrosis >F0 at baseline in the fazirsiran and placebo groups, respectively
My take: This is an exciting development for patients with A1AT-associated liver disease. Longer duration data is needed to confirm whether fazirsiran will be a useful therapeutic agent for A1AT deficiency. If effective, selecting patients who benefit from treatment will need to be determined.
9698 participants in NHANES during the 2017-2020 cycle completed a transient elastography examination. After excluding patients less than 18 years, these were the key findings:
37.87% had steatotic liver disease
32.45% had MASLD
2.56% had MetALD
1.17% and ALD
Limitations: database study, lack of liver biopsy, reliance on self-reports of alcohol consumption
Methods: 336,866 adults aged ≥30 years were prospectively enrolled in a health screening program between 1997–2013
Key findings:
122,669 (36.4%) had MASLD. Over a mean follow-up of 15 years, 5562 new cases of cirrhosis and 2273 new cases of HCC were diagnosed.
Hazard ratios for HCC were 8.86 for MASLD with HBV or HCV, compared with non-SLD without HBV or HCV
Hazard ratios for HCC were 8.81 for HBV or HCV with non-SLD (SLD), and 1.52 for MASLD without HBV or HCV
My take: MASLD significantly increased cirrhosis and HCC risks; however the risk of HBV or HCV was much greater. The high prevalence rates of MASLD guarantees a huge need for liver disease management for the foreseeable future.
This meta-analysis consisted of eighty-seven articles involving 60,829 living liver donors.
Key findings:
The overall pooled incidence of complications in LDLT donors was 24.7%
The incidence of minor complications was 17.3%
The incidence of major complications was 5.5%
The overall incidence of donor mortality was 0.06% in 49,027 individuals**.
Psychological complications 7.6% were the most common complications among LDLT donors. This was followed by wound-related complications 5.2%
Table 2 (below) gives an extensive list of potential complications and their incidences in this cohort
**In the discussion, the authors note that “donor mortality is a devastating outcome in LDLT…Our study found that Asian countries reported a lower rate…For example, in Japan, the rate of donor mortality was 0.3 deaths per 1000 donors, while in the United States and Europe, donor mortality rates were 1.7 and 2.3 deaths per 1000 donors, respectively. While this observation may be attributed to greater experience in LDLT in Asian centers, it is also possible that underreporting in Asian centers might play a role. Mortality in donors…may result in the suspension or termination of an LDLT program.”
My take: Even with potential underreporting, this study highlights the very real risks associated with trying to save a life via LDLT.
“At 12 months, liver biopsies showed that a greater proportion of subjects who were treated with Rezdiffra achieved NASH resolution or an improvement in liver scarring as compared with those who received the placebo. A total of 26% to 27% of subjects who received 80 milligrams of Rezdiffra and 24% to 36% of subjects who received 100 milligrams of Rezdiffra experienced NASH resolution and no worsening of liver scarring, compared to 9% to 13% of those who received placebo and counseling on diet and exercise…n addition, a total of 23% of subjects who received 80 milligrams of Rezdiffra and 24% to 28% of subjects who received 100 milligrams of Rezdiffra experienced an improvement in liver scarring and no worsening of NASH, compared to 13% to 15% of those who received placebo, depending on each pathologist’s readings.”
“The most common side effects of Rezdiffra included diarrhea and nausea. Rezdiffra comes with certain warnings and precautions, such as drug-induced liver toxicity and gallbladder-related side effects. Use of Rezdiffra should be avoided in patients with decompensated cirrhosis.”
My take: It is good to finally have an FDA-approved medication for MASH (in adults). My speculation is that medications which achieve persistent weight loss will have a more pronounced effect on liver health and overall health.
Background: Trientine (TRI) and D-penicillamine (PEN) are used to treat copper overload in Wilson disease. Their main mode of action is thought to be through the facilitation of urinary copper excretion. In a recent study, TRI was noninferior to PEN despite lower 24-hour urinary copper excretion than PEN.
Key findings and conclusions:
“TRI inhibits intestinal copper absorption, in addition to its cupriuretic effect. In contrast, PEN has modest effects on the intestinal copper absorption. This may explain why TRI and PEN are equally effective although urinary copper excretion is lower with TRI.”
” TRI (n=8) reduced hepatic 64Cu activity 1 hour after 64Cu dose from 6.17 (4.73) to 1.47 (2.97) standard uptake value, p<0.02, and after 15 hours from 14.24 (3.09) to 6.19 (3.43), p<0.02, indicating strong inhibition of intestinal 64Cu absorption.”
“PEN (n=8) slightly reduced hepatic standard uptake value at 15 hours, from 16.30 (5.63) to 12.17 (1.44), p<0.04.”
“The study questions whether the same therapeutic targets for 24-hour urinary excretion apply to both drugs.”
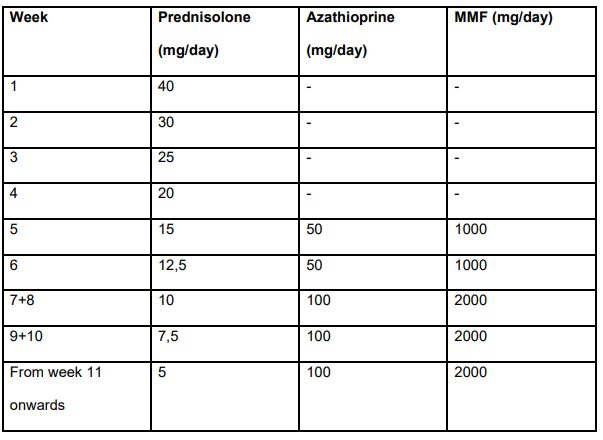
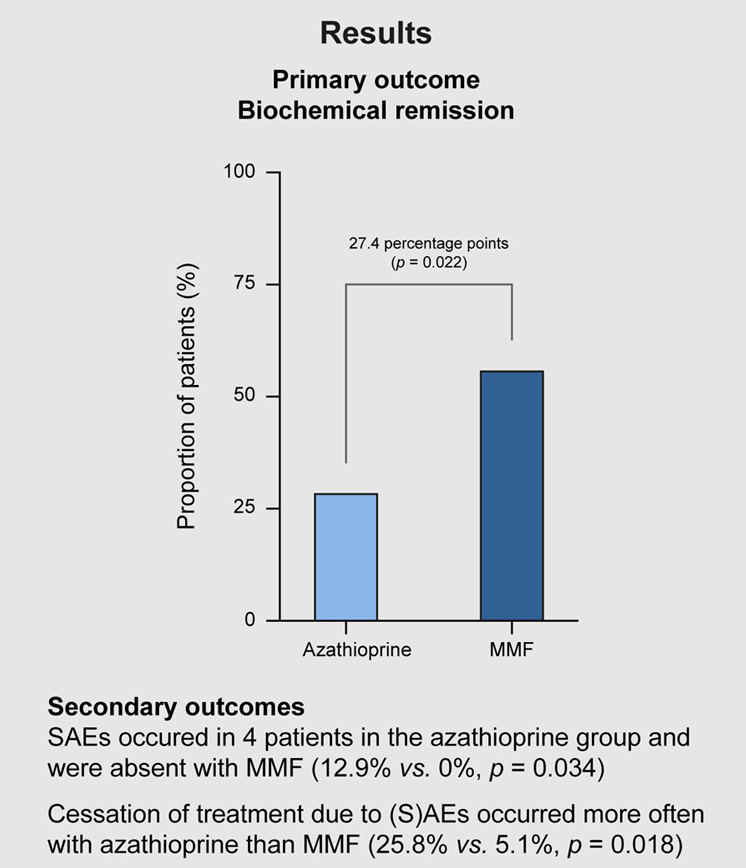
Methods: In this 24-week, prospective, randomised, open-label, multicentre superiority trial, 70 patients (mean age 57.9 years) with treatment-naive AIH received either MMF or azathioprine, both in combination with prednisolone. The primary endpoint was biochemical remission (BR) defined as normalisation of serum levels of alanine aminotransferase and IgG after 24 weeks of treatment.
Treatment dosing in study (Table S2):
Key findings:
56.4% of the MMF group and 29.0% of the azathioprine group achieved BR
No serious adverse events occurred in patients who received MMF (0%) but serious adverse events were reported in four patients who received azathioprine (12.9%) (p = 0.034)
Excerpts from the discussion:
“The evidence for the current standard induction therapy in AIH with azathioprine and prednisolone is limited and stems from the early seventies of the last century.”
“Patients assigned to azathioprine were significantly more prone to discontinuing treatment because of intolerance or SAEs, with nausea and vomiting as the main reasons for cessation of treatment.”
“MMF exhibits high teratogenicity. MMF should not be used during pregnancy and may only be used with strict contraceptive measures in women of childbearing age and men planning to father a child, as its use is absolutely contraindicated during pregnancy.”
“In addition, MMF must be administered twice daily, while azathioprine is given as a single dose daily…relevant for a disease that requires lifelong treatment.”
My take: This study needs to be replicated in the pediatric age group. Though many patients have some frequent side effects with MMF, the overall safety (and possibly effectiveness) appears improved with MMF compared with azathioprine.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Cyanobacteria are commonly found in water bodies and their production of hepatotoxins can contribute to liver damage.
Methods: Across the contiguous United States, regions with high cyanobacteria exposure (CE) counts in water bodies were identified using satellite remote sensing data. The data were geospatially mapped to county boundaries, and disease mortality and incidence rates were analyzed.
Key findings:
There was a highly significant spatial association between CE, liver disease, and liver cancer. In Figure 4, the counties in the top half of CE had higher liver cancer. The mean CE 569.6 in the top half compared with median counts of CE of 319.5 in the bottom half of CE
Counties with CE exceeding the 80Th percentile for >8 or more years had as significantly higher liver cancer age-adjusted incidence rate (mean 9.48) compared with that did so for 5 or fewer years (mean=8.79)
Hot spots of CE and mortality were identified along the Gulf of Mexico, eastern Texas, Louisiana, and Florida, and cold spots across the Appalachians.
Cyanotoxins were detected in 62% of US counties using remote sensing.
My take: This study shows an association between areas with higher CE exposure and increased risk of liver cancer. This could be mediated via contaminated water exposure.