Cyanobacteria are commonly found in water bodies and their production of hepatotoxins can contribute to liver damage.
Methods: Across the contiguous United States, regions with high cyanobacteria exposure (CE) counts in water bodies were identified using satellite remote sensing data. The data were geospatially mapped to county boundaries, and disease mortality and incidence rates were analyzed.
Key findings:
There was a highly significant spatial association between CE, liver disease, and liver cancer. In Figure 4, the counties in the top half of CE had higher liver cancer. The mean CE 569.6 in the top half compared with median counts of CE of 319.5 in the bottom half of CE
Counties with CE exceeding the 80Th percentile for >8 or more years had as significantly higher liver cancer age-adjusted incidence rate (mean 9.48) compared with that did so for 5 or fewer years (mean=8.79)
Hot spots of CE and mortality were identified along the Gulf of Mexico, eastern Texas, Louisiana, and Florida, and cold spots across the Appalachians.
Cyanotoxins were detected in 62% of US counties using remote sensing.
My take: This study shows an association between areas with higher CE exposure and increased risk of liver cancer. This could be mediated via contaminated water exposure.
SA Harrison et al. NEJM 2024; 390: 497-509. A Phase 3, Randomized, Controlled Trial of Resmetirom in NASH with Liver Fibrosis
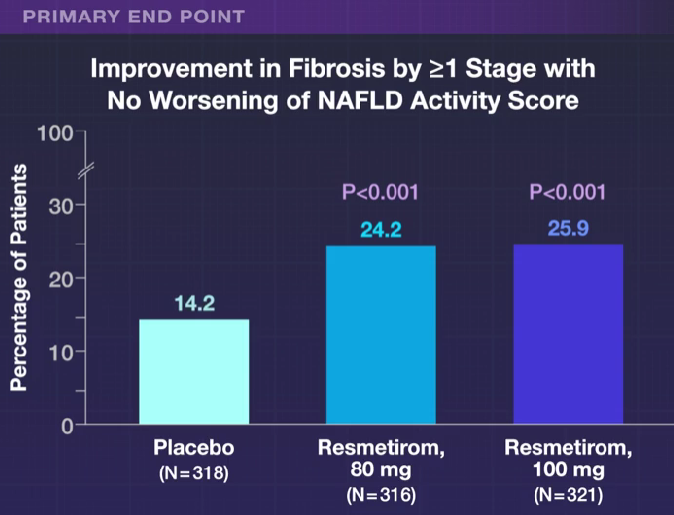
This “MAESTRO-NASH” study enrolled 966 adult patients biopsy-confirmed NASH (now termed MASH) and a fibrosis stage of F1B, F2, or F3. Approximately 60% of each arm had F3 fibrosis. Patients were randomly assigned in a 1:1:1 ratio to receive once-daily d resmetirom at a dose of 80 mg or 100 mg or placebo; Resmetirom is an oral, liver-directed, thyroid hormone receptor beta–selective agonist.
Key findings:
MASH “resolution with no worsening of fibrosis was achieved in 25.9% of the patients in the 80-mg resmetirom group and 29.9% of those in the 100-mg resmetirom group, as compared with 9.7% of those in the placebo group (P<0.001)”
“Fibrosis improvement by at least one stage with no worsening of the NAFLD activity score was achieved in 24.2% of the patients in the 80-mg resmetirom group and 25.9% of those in the 100-mg resmetirom group, as compared with 14.2% of those in the placebo group (P<0.001)”
“Levels of a broad range of atherogenic lipids and lipoproteins, including LDL cholesterol, non-HDL cholesterol, triglycerides, apolipoprotein B, and lipoprotein(a), appeared to be reduced by resmetirom relative to placebo, findings consistent with those of earlier studies.18,19“
Diarrhea and nausea were more frequent in the resmetirom group compared to placebo, though there were no differences in serious adverse effects. Patients in the 100 mg group were more likely to discontinue treatment (~7%) compared to 2% in the other two groups.
“In this trial, achievement of a 30% reduction in hepatic fat (MRI-PDFF) or a 120% increase in the sex hormone–binding globulin level appeared to be associated with biopsy responses.”
In their discussion, the authors note that “Noninvasive testing to identify patients with NASH for treatment and to monitor treatment response will be important in clinical practice in which liver biopsy is infrequently used.”
The associated editorial by Kenneth Cusi (pg 559-561) notes the following:
Resmetirom had neutral effects on body weight and insulin resistance.
“Treatment affected the pituitary–thyroid hormone axis, with prohormone free T4 levels decreasing by approximately 17 to 21% and mean thyrotropin levels also decreasing.” It is unclear if this has any long-term significance (long-term data needed). ”Careful surveillance to detect early endocrine disease that is related to potential thyroid, gonadal, or bone disease appears warranted to avoid any potential risks from long-term treatment.”
When subtracting the placebo effect, he notes that “approximately 2 of 10 patients treated will have NASH resolution and approximately 1 of 10 patients treated will have fibrosis improvement.” Thus, combination therapy may be needed.
My take: This study brings us a step closer to having a medication which can improve MASH as currently there are no FDA-approved medications. My speculation is that medications which achieve persistent weight loss will have a more pronounced effect on liver health and overall health.
Congress has an opportunity to turn this ongoing human tragedy into a public health advancement, by providing support for a five-year project to eliminate hepatitis C in the United States...
Each year, about 15,000 Americans die from hepatitis C, many in their 40s and 50s. Given the safe and effective cure available for the last nine years, the correct number of deaths in 2023 should be zero...
In March, President Biden came out in favor of a five-year program to put the United States on track to eliminate hepatitis C…The plan includes an innovative approach to provide broad access to curative medications, modeled on a successful effort in Louisiana. Under this approach, sometimes known as the “Netflix model,” a drug company or companies agree to provide full access to medications for a population in need in exchange for a set lump sum payment. In the current proposal, the populations who would have access to free hepatitis C drugs are Medicaid enrollees, the uninsured, Native Americans, and those in the prison and jail systems. If structured correctly, many more people can get lifesaving care and the cost per cure drops significantly…the plan also includes training, technical support and resources for primary care offices, federally qualified health centers, drug treatment centers, and jails and prisons…
An expert group has estimated that a national initiative to end hepatitis would save society more than $18 billion in health care costs over the next decade, with $13.3 billion of that savings accruing to the federal government.
My take: The advent of safe and effective hepatitis C medications has helped many. Particularly with the challenge of more infections due to intravenous drug use, it will take a concerted effort to eliminate this infection.
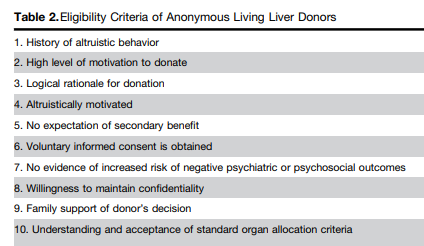
This commentary, from Toronto General Hospital practitioners, discusses the increasing use of anonymous living liver donation (ALLD) in North America and donor altruism which is a term coined and popularized by the French philosopher Auguste Comte in the 1800s. Altruism is the principle and moral practice of concern for the welfare or happiness of others.
Key points:
Living-donor liver transplantation (LDLT) … in Toronto currently makes up 30% of adult and 80% of pediatric liver transplants.
Over the past 4 years, ALLD activity has doubled and now accounts for 15% of our yearly LDLT activity (80–85/year). Similar rates of growth in ALLD have occurred in the USA, whereas it remains rare outside of North America
The Canadian system provides several important advantages for anonymous donors: publicly funded health care that covers the cost of the donor assessment, surgery, and postoperative care; supportive employers and social programs that minimize financial losses; and a provincially funded program (Prelod) that reimburses incidental costs related to travel, accommodation, and meals up to $6000.
Important steps toward supporting living donation have been taken in the USA, such as the development of the National Living Donor Assistance Center as well as the Patient Protection and Affordable Care Act, which makes it illegal for insurance companies to deny health coverage to living donors…
Donors in the USA, however, still face significant obstacles to obtaining life insurance, long term care insurance, and disability insurance. Notably, the National Living Donor Protection act, which aims to rectify this problem (https://www.congress.gov/bill/117th-congress/ house-bill/1255/text) has yet to move through Congress despite pressure from the transplant community
My take: It is definitely a good idea to promote living donors by removing insurance obstacles/discrimination
This article has 50 recommendations for prevention, diagnosis, and treatment of hepatocellular carcinoma. I will focus on prevention/screening in this post as this is most relevant to pediatric practice.
Figure 1
Figure 3 provides data supporting benefits of hepatocellular carcinoma (HCC) surveillance. HCC surveillance has been shown to significantly reduce HCC-related mortality in a randomized controlled trial among patients with chronic HBV infection and in several cohort studies among patients with cirrhosis from any etiology.
Who to screen for HCC:
Key Recommendations on Surveillance:
My take: This guidance recommends ultrasound and AFP monitoring every 6 months in those at high risk of developing HCC. Most pediatric patients would not require surveillance based on this guidance.
HBV Vaccination Prevents Cancer In Taiwan: HCC incidence per 105 person-years was 0.92 in the unvaccinated cohort and 0.23 in the vaccinated birth cohorts.
After inverse probability of treatment weighting (IPTW) (n = 819), the 5-, 10-, and 15-year cumulative HCC incidence was 3%, 4%, and 9% among treated patients (n = 394) versus 3%, 15%, and 19%, among untreated patients (n = 425), respectively (p = 0.02)
It took 5 years of treatment before there was a significant reduction in HCC risk
The protective effect was mainly in males; it was not observed in females and in patients who were HBeAg negative
The author studied patients with “Indeterminate” HBV; that is, patents that did not fit into the following categories:
The above definitions are AASLD definitions for the HBV categories. In their study, the authors’ definitions required immune tolerant to have ALT <1 x ULN, immune active to have ALT >/= ALT 2 x ULN. Inactive patients had no significant fibrosis or inflammation. The authors gauged fibrosis with either histology or a noninvasive measure (eg. FIB-4, or elastography)
My take: In this subgroup with indeterminate-phase chronic hepatitis B, antiviral treatment resulted in a 70% reduction in HCC risk. Previous AASLD guidelines indicated that treatment is mainly beneficial for immune active HBV; this study indicates that adults with indeterminate-phase HBV benefit as well. Also, as noted in prior blog posts (see below), the term “immune tolerant” is falling out of favor. In addition, updated expert recommendations on expanding treatment have been published: P Martin et al. Clin Gastroenterol Hepatol 2022; 20: 1766-1775 (post: What’s New in the Treatment of Hepatitis B (2022)
This article offers best practice advice -here are two of them:
#2: A Fibrosis 4 Index score <1.3 is associated with strong negative predictive value for advanced hepatic fibrosis and may be useful for exclusion of advanced hepatic fibrosis in patients with NAFLD.
#8 Patients with NAFLD and NITs (noninvasive tests) results suggestive of advanced fibrosis (F3) or cirrhosis (F4) should be considered for surveillance of liver complications (eg, hepatocellular carcinoma screening and variceal screening per Baveno criteria). Patients with NAFLD and NITs suggestive of advanced hepatic fibrosis (F3) or (F4), should be monitored with serial liver stiffness measurement; vibration controlled transient elastography; or magnetic resonance elastography, given its correlation with clinically significant portal hypertension and clinical decompensation.
In this study from U.S., patients (n=2523) were divided into three categories based on FIB-4 scores: (A) Fibrosis-4 (FIB-4) <1.3 and/or liver-stiffness measurement (LSM) measured by Fibroscan <8 kp, (B) FIB-4 1.31‒2.6 and/or LSM 8.1-12.5 kp, and (C) FIB-4 >2.6 and/or LSM >12.5 kp. However, those in class A with aspartate transaminase:alanine transaminase ratio >1 or platelets <150,000/mm3, or class B with aspartate transaminase:alanine transaminase ratio >1 or platelets <150,000/mm3 were upstaged by one class. The data were reviewed retrospectively from a prospective longitudinal cohort (TARGET-NASH)
Key findings: All adverse outcomes including liver and cardiovascular (see below) were correlated with FIB-4 staging.
Key findings: The prevalence of steatosis, severe steatosis, advanced fibrosis, and cirrhosis was 44.39%, 10.57%, 2.85%, and 0.87%, respectively in Chinese adults
Limitation: This data was derived from a health checkup cohort which could give different results than a random population sampling. Patients at health checkups may be more health conscious and/or be aware of underlying health concerns.
Prevalence of different grades of liver fibrosis in different age groups.
My take: Steatotic liver disease is a huge worldwide problem. The growing prevalence is going to result in extensive health issues.
—————
This year’s pumpkin 910/31/23):
It does not look like I will become a professional pumpkin artist anytime soon!
This review article makes a number of useful points:
Almost all of the IBD medications (Anti-TNF, Vedolizumab, Ustekinumab, Tofacitinib, Ozanimod) should not be used in patients with untreated hepatitis B surface antigen positivity. Antiviral prophylaxis is recommended even patients with inactive disease (HBV DNA <2000 IU/mL/normal ALT) starting 2 weeks prior to immunosuppression up to 12 weeks after immunosuppression discontinuation.
Anti-TNF, Vedolizumab, and Ustekinumab can be safely used in patients with cirrhosis, tofacitinib requires a dose reduction, and ozanimod is NOT recommended
Autoimmune hepatitis may be triggered (rarely) by use of anti-TNFs; however, these agents have been uses off-label as a rescue therapy for AIH as well.
Anti-TNFs do not appear worsen liver function in PSC and may be associated with improvement in MASH (NASH)
Drug-induced liver injury (DILI) is common with anti-TNFs, often seen between the second and fifth doses. It is “generally transient and asymptomatic.” DILI may occur with ustekinumab, tofacitinib and ozanimod.
Tofacitinib may have a favorable effect on PSC. A retrospective study with 5 patients reported a 28% and 39% decrease respectively in total bilirubin and alkaline phosphatase within 6 months of starting therapy, A separate study with 42 patients showed a non-significant drop in alkaline phosphatase from 150 U/L to 132 U/L at 12 month followup.
The authors note that in patients with cirrhosis and posttransplantation, “vedolizumab and ustekinumab should be preferred due to their safer profile linked to infectious risk.”
“Patients with hepatobiliary disorders are often excluded from pivotal trials.” This contributes to a significant knowledge gap for patients with these comorbid conditions which are frequent in patients with IBD
My take: I don’t think I will be too popular if I hand out copies of this article to the kids I see later today –despite the useful advice. (This post was meant to be published on Halloween)
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
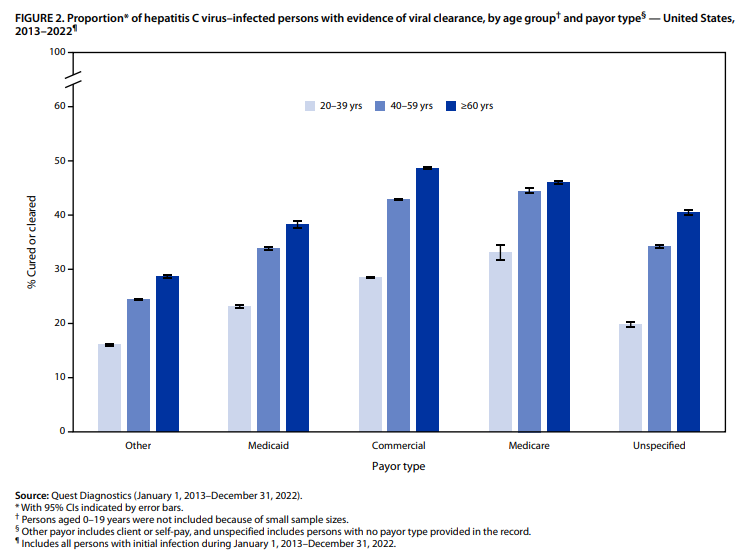
Among the approximately 1.0 million persons in this analysis with initial infection, only 34% had laboratory evidence of viral clearance
Overall, viral clearance was lowest among persons aged 20–39 years (24%). Patients 0-19 were not included in this analysis
To overcome the low cure rate, some have recommended a subscription model for HCV treatment; this was piloted in Louisiana. In this pilot, the state paid a lump sum to make the drug available for free to all patients on Medicaid and federal prisoners. Francis Collins has indicated that a national program, while expensive, would save the government $13 billion in 10 years (Source: Infectious Disease Special Edition, 6/30/23: Most Americans With HCV Not Receiving DAAs)
My take: Improving access to HCV treatment has the potential to save livers, save lives and save money.
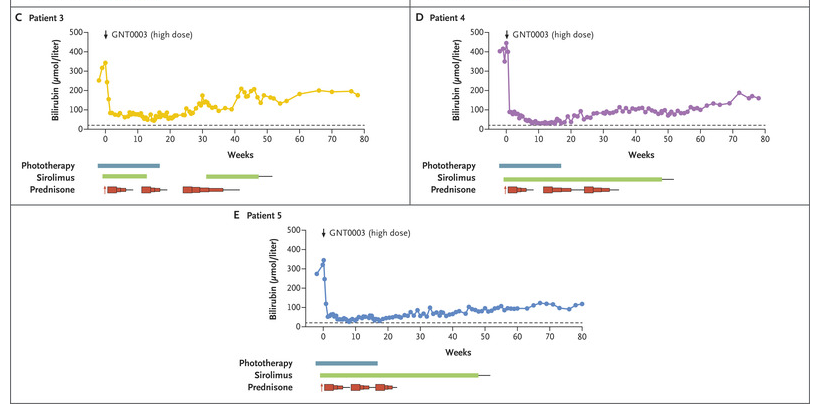
L D’Antiga et al. NEJM; 2023; 389: 620-631. Gene Therapy in Patients with the Crigler–Najjar Syndrome
Methods: Five patients received a single infusion of the gene construct (GNT0003): two received 2×1012 vector genomes (vg) per kilogram of body weight, and three received 5×1012 vg per kilogram. The primary end points were measures of safety and efficacy; efficacy was defined as a serum bilirubin level of 300 μmol per liter or lower measured at 17 weeks, 1 week after discontinuation of phototherapy. The infusion protocol included administration of sirolimus adjusted for a trough of 4-12 mcg/L (starting 1 week prior to infusion) and steroids (IV day prior then oral for 8 weeks). .
Key findings
By week 16, serum bilirubin levels in patients who received the lower dose of GNT0003 exceeded 300 μmol per liter.
The patients who received the higher dose had bilirubin levels below 300 μmol per liter in the absence of phototherapy at the end of follow-up; mean level at the final follow-up visit [week 78 in two patients and week 80 in the other], was149±33 μmol per liter.
No serious adverse events were reported. Mild increase in ALT levels were seen in 4 of 5 patients; this was “potentially related to an immune response against the infused vector; these patients were treated with a course of glucocorticoids.”
This figure shows the response of the serum bilirubin in patients receiving the higher dose of the infusion.
My take: This study shows that the GNT0003 increased UGT1A1 activity to levels that permitted cessation of phototherapy; this persisted for 18 months after treatment. Further studies are needed.