Recently DHS released a website (multiple languages) with resources/information to help with current formula shortages; some of the information links to information from NASPGHAN. The website has links to several new formulas that are being imported, like Kendamil, Nan, and Bubs, and how they are prepared (mL to ounce converter).
The infant formula crisis isn’t simply another case of a one-off event causing pandemic-related supply chain pressures to boil over. Instead, U.S. policy has exacerbated the nation’s infant formula problem by depressing potential supply….all part of our government’s longstanding subsidization and protection of the politically powerful U.S. dairy industry…
[Additionally, there] are strict FDA labeling and nutritional standards that any formula producer wishing to sell here must meet….These regulatory barriers are probably well-intentioned, but that doesn’t make them any less misguided—especially for places like Europe, Canada, or New Zealand that have large dairy industries and strict food regulations
The combination of trade and regulatory barriers to imported infant formula all but ensures that our almost $2 billion U.S. market is effectively captured by a few domestic producers—despite strong demand for foreign brands. What German company, for example, is willing to spend the time and money meeting all the FDA requirements—registration, clinical trials, labeling and nutritional standards, inspections, etc.—only to then face high import taxes that make its product uncompetitive except during emergencies? The answer: almost none…
Meanwhile, Abbott is in full-on crisis mode and has turned to flying in formula produced at an FDA-registered Irish affiliate…
WIC program’s use of sole supplier contracts has created a problem specific to the current crisis because … the big FDA recall just happened to hit the very producer—Abbott—holding most of the WIC contracts.
My take: This article explains why there is not a simple switch to flip to fix the current formula bottlenecks.
This review and meta-analysis examined forty-six studies involving 11 077 participants.
Key findings:
At 6 months, behavior weight management programs (BWMPs) using motivational interviewing (MI) were more effective than no/minimal intervention (−0.88) but were not statistically significantly more effective than lower-intensity (−0.88 ) or similar-intensity (−1.36 ) BWMPs.
“At 1 year, data were too sparse to pool comparisons with no/minimal intervention, but MI did not produce statistically significantly greater weight change compared with lower-intensity”
My take: Several years ago our hospital system strongly encouraged practitioners to learn motivation interviewing techniques. However, based on this review, “there is no evidence that MI increases effectiveness of BWMPs in controlling weight.”
Levine et al provide a good overview of the topic of emulsifiers. Key points:
Emulsifiers allow “the mixing of water and and water-soluble agents with fats and fat-soluble agents that is they possess both hydrophilic and lipophilic properties”
The FDA “has been responsible for approving the use of all direct food additives” (n=~3000) and “for regulatory purposes, [the FDA excluded] some substances that were generally regarded as safe (GRAS) (n=~450)…Precisely how some emulsifiers gained GRAS status is unclear.
“Lecithin” is derived from the Greek name for egg yolk (lekithos). “Over the years the use of the term “lecithin” has been taken to include various mixtures of different phospholipids” (not just phosphatidylcholine).
Lecithin can provide the substrate “for the production of trimethylamine N-oxide (TMAO)…linked to cardiac events and cardiovascular inflammation.”
“The list of emulsifiers that are widely used, but not considered GRAS, most notably include polysorbate 80 (p80), carboxymethylcellulose (CMC) and carrageenan…these emulsifiers have been linked to the disruption of the microbiota and gut mucosal lining…In addition, low-grade inflammation [has been] associated with consumption of emulsifying agents such as CMC and p80” [in mouse models].
The International Organization for the Study of Inflammatory Bowel Disease (IOIBD) has recommended that IBD patients “limit consumption of certain commonly encountered synthetic emulsifiers, specifically carboxymethylcellulose (E466/cellulose gum) and polysorbate 80 (E433) [which] are present in many processed foods, such as ice cream. The group also recommends a decrease in foods containing carrageenan”
In the second study by Chassaing et al with 16 healthy adults, the authors studied the effects of CMC in those with an emulsifier-free diet (n=9) or an identical diet enriched with CMC (n=7).
Key findings:
Relative to control subjects, CMC consumption modestly increased postprandial abdominal discomfort and perturbed gut microbiota composition in a way that reduced its diversity
CMC-fed subjects exhibited changes in the fecal metabolome, particularly reductions in short-chain fatty acids and free amino acids
2 subjects consuming CMC who exhibited increased microbiota encroachment into the normally sterile inner mucus layer, a central feature of gut inflammation, as well as stark alterations in microbiota composition
My take: The dramatic increase in the prevalence of IBD over the past 50 years indicates a strong influence of environment factors, particularly diet. Determining which of these factors are most important will be challenging. These articles indicate that some emulsifiers could be contributing to GI tract inflammation and non-GI tract inflammation as well.
The challenges with identifying dietary factors relate to difficulties with using randomized controlled trials (especially eliminating delicious foods) to assess the impact over a long period of follow-up.
Background: “Processed foods often include many non-natural ingredients and additives such as artificial flavours, sugars, stabilisers, emulsifiers, and preservatives. Detergents and emulsifiers that are added to foods might have a detrimental effect on the gut barrier. Carboxymethylcellulose has been shown to increase bacterial adherence to intestinal epithelium and might lead to bacterial overgrowth and infiltration of bacteria into the spaces between intestinal villi. Polysorbate 80, an emulsifier commonly used in processed foods, increases translocation of bacteria such as Escherichia coli across M cells and Peyer’s patches in people with Crohn’s disease.”
Methods: Using food questionnaires, the authors prospectively followed 116 087 adults aged 35-70 years from 21 low, middle, and high income countries from 2003 to 2016 (median follow-up of 9.7 years).
Key findings:
After adjustment for potential confounding factors, higher intake of ultra-processed food was associated with a higher risk of incident IBD with a hazard ratio of 1.82 for ≥5 servings/day and 1.67 for 1-4 servings/day (compared to <1 serving/day)
Since this is an observational study, this does not prove a causal association between these foods and inflammatory bowel disease. Nevertheless, limiting the consumption of ultraprocessed foods is a good idea as these foods may increase the risk of other health problems as well, including cardiometabolic disease and cancer (Gastroenterol 2022; 162: 652-54). This will be difficult, though, as in the U.S. more than half of calories consumed are from ultraprocessed foods.
My take: This study supports the notion that more fresh foods in our diets is beneficial.
Day-to-day, I find I am focused (?inundated) on problems that are literally right in front of me. Every once in a while, it is important to look more broadly and try to consider/address the larger issues.
Along those lines, I would recommend a series of important articles on adolescent nutrition published by The Lancet. Thanks to William Balistreri for sharing these references.
This is an introduction to the series of articles. “Given these increasingly transnational dimensions of the ultra-processed food industry, it is timely for WHO, the Food and Agriculture Organization of the UN, and their partners to revisit calls for global regulatory frameworks to assist governments in taking action. Given the speed of nutritional change, there is perhaps no greater immediate threat to the health of adolescents. Equally, tackling adolescent nutrition presents an unparalleled opportunity to interrupt intergenerational cycles of malnutrition and respond to the urgent challenges of planetary change”
The review highlights how nutrition in youth/adolescence influences weight, height, BMI as well as the timing of puberty, neurodevelopment, cardiorespiratory fitness, immune function, body composition and bone mass
Adolescents are “growing up at a time of momentous shift—ie, rapid urbanisation, climate change, food systems shifting towards foods with an increased caloric and decreased nutritional value, the COVID-19 pandemic, and growing socioeconomic inequality. The consequences of these changing contexts have profound impacts on adolescent nutrition and development”
“Adolescents have a lot to say about why they eat what they eat, and the factors that might motivate them to change. Adolescents must be active partners in shaping local and global actions that support healthy eating patterns. Efforts to improve food environments and ultimately adolescent food choice should harness widely shared adolescent values and desire for social interaction around food”
The article reviews in depth information from prior surveys including India’s Comprehensive National Nutrition Survey and the Global School-based Student Health Surveys. However, they note that nationally representative detailed dietary intake data are still scarce
Food choices by adolescents in modern communities is more heavily influenced by convenience and autonomy; in more traditional communities, family and community priorities often supersede individual considerations of adolescents
In the setting of the pandemic, more families (worldwide) are being pushed into food insecurity and shifting towards lower-cost, less nutritious non-perishable foods.
“Even in less food-insecure contexts, social isolation is resulting in negative trends among some adolescents, such as reported weight gain, poor eating habits, and stress eating”
“Adolescence (10–24 years of age) is “characterised by transition, exploration, and openness to change [good and bad], offering opportunities for radical shifts in diet, physical activity, and other risks for non-communicable diseases. This same novelty-seeking and openness to change also makes adolescents a vulnerable group to commercial exploitation and other unhealthy influences, with lifelong and intergenerational consequences”
“Despite micronutrient deficiencies and food insecurity persisting in many places, and overweight and obesity rapidly increasing, adolescents have been largely overlooked in global nutritional policy frameworks. Targets should be established for adolescent nutrition in its global tracking and accountability mechanism”
“Greater government fiscal and policy action to both restrict the availability of highly processed foods and enhance healthy and diverse adolescent diets is urgently needed”
Nutrition education needs to be leveraged in schools: “knowledge of dietary diversity, food environment, and practical skills; use opportunity of school curricula to support nutrition and food preparation; improving choice architecture”
Social media has become a huge influence on dietary choices, body image, and psychological well being, both through advertising and marketing to adolescents and subsequent peer interactions
My take: If we truly hope to improve population health, improving diet choices cannot remain the province of only the well-educated wealthy. Adolescence offers a chance to change health trajectories before habits are more rigid and before the development of fixed health consequences.
Personal item: If any blog follower has experience using biologics (eg mepolizumab, benralizumab) in a young child (1 yo) with eosinophilic colitis and marked eosinophilia, please send me a personal email: jjhochman@gmail.com.
“Another series of studies from the University of Texas found that four seconds — yes, seconds — of ferocious bicycle pedaling, repeated several times, was enough to raise adults’ strength and endurance, whatever their age or health when they started.”
“As I wrote in July, the familiar goal of 10,000 daily steps, deeply embedded in our activity trackers and collective consciousness, has little scientific validity. It is a myth that grew out of a marketing accident, and a study published this summer further debunked it, finding that people who took between 7,000 and 8,000 steps a day, or a little more than three miles, generally lived longer than those strolling less or accumulating more than 10,000 steps.”
“Exercise also has a disproportionate impact on our odds of enjoying a long, healthy life. According to one of the most inspiring studies this year, overweight people who started working out lowered their risk of premature death by about 30 percent even if they remained overweight, with exercise providing about twice as much benefit as weight loss might…Exercise enhances our brain power, too, according to other, memorable experiments from this year”
“In the study, which I wrote about in May, active people reported a stronger sense of purpose in their lives than inactive people….In effect, the more people felt their lives had meaning, the more they wound up moving, and the more they moved, the more meaningful they found their lives.
For successful aging, recognize one’s issues and adapt accordingly. “Sooner or later, we all must recognize what is no longer possible and find alternatives,” says Jane Brody (Personal Health columnist) –“Inspired by Steven Petrow’s book, “Stupid Things I Won’t Do When I Get Old.”
Learning from ‘Super-Agers’ — “past research has revealed lifestyle factors that contribute to resilience such as obtaining a high level of quality education; holding occupations that deal with complex facts and data; consuming a Mediterranean-style diet; engaging in leisure activities; socializing with other people; and exercising regularly”
The sweet spot for longevity lies around 7,000 steps a day (or 30 minutes of exercise).
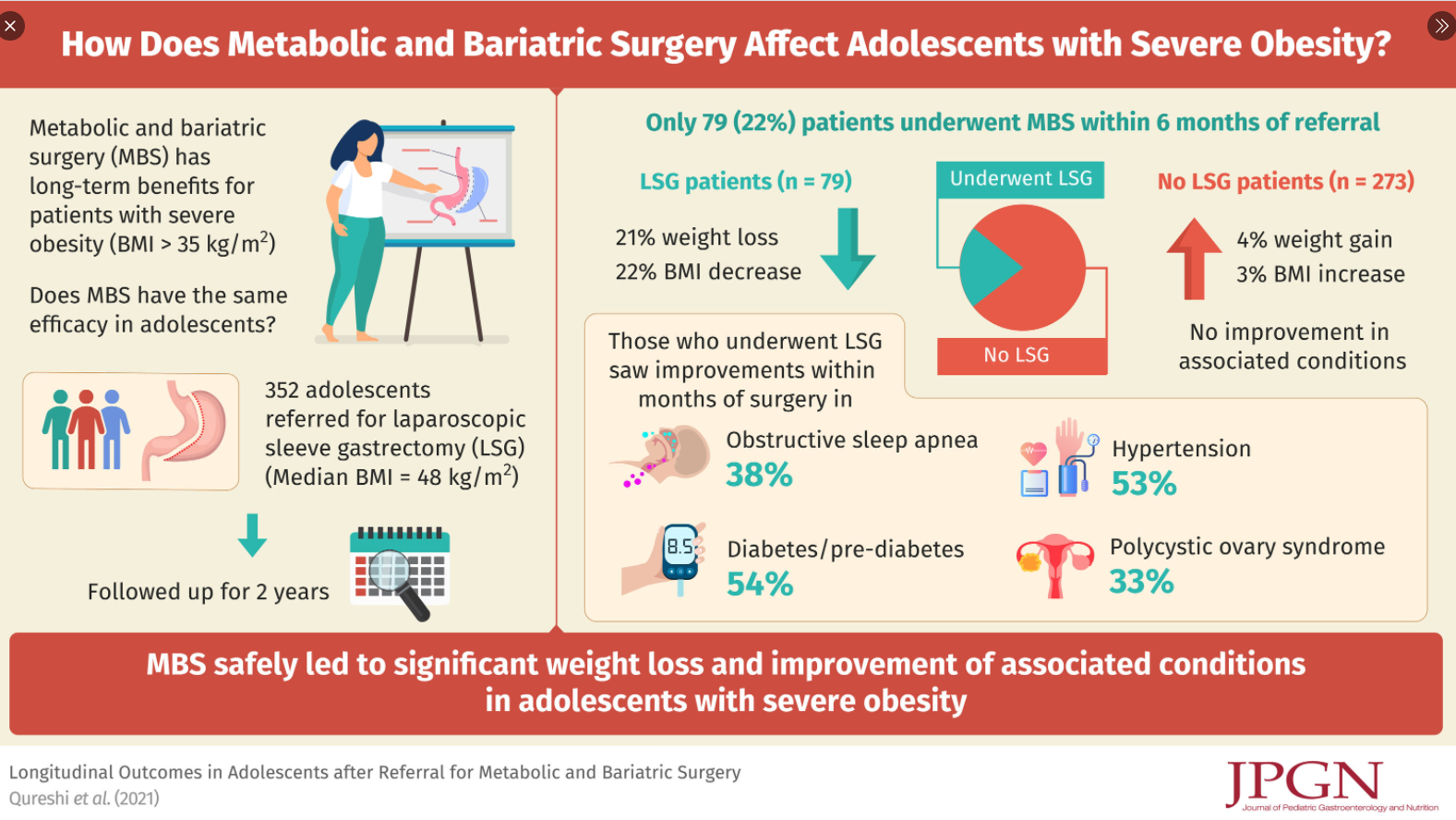
Only 22% underwent bariatric surgery (Laparoscopic sleeve gastrectomy (LSG)), mainly due to lack of interest in those referred
Reasons for NoLSG: 171 (62% of the NoLSG group) did not return for a 2nd visit, 28 (10%) were considered non-adherent to clinical recommendations, 14 (6%) had insurance denials, 16 (6%) had psychological contraindications including recent suicidal ideations, and 29 (11%) are still considering/pursuing LSG
Only 8 (2.3%) of entire cohort were self-pay
LSG patients had 21% total weight loss and 22% total BMI loss at 24 months whereas NoLSG patients had 4% total weight gain and 3% BMI gain (P < 0.01)
LSG group had improvement in obesity-associated conditions compared to group without surgery (P < 0.01)
Follow-up in both groups was poor (40% for LSG group and <20% for the NoLSG group) 1 year after bariatric referral. This is of particular interest in the LSG group b/c for surgery, patients are required to agree to a 5 year f/u period (though this lacks an enforcement mechanism). The authors note some improvement in f/u coincident with recent broader adoption of telemedine
My take: This single-center found that most patients referred for consideration of bariatric surgery did not have this surgery.
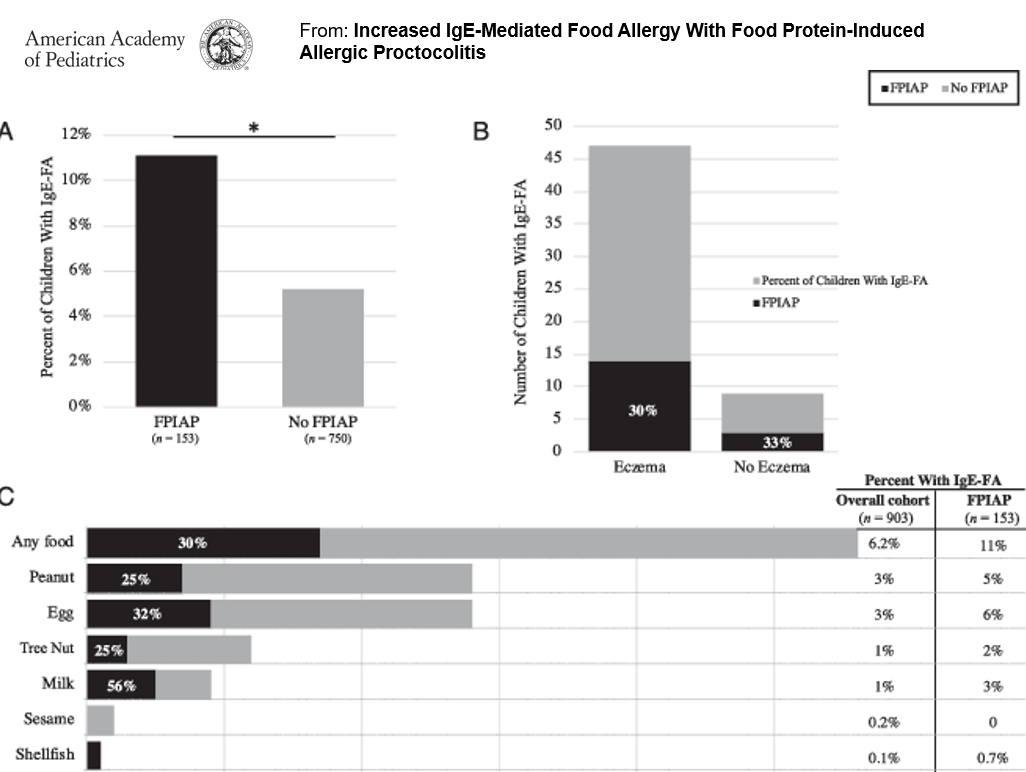
In this study of 153 infants with food protein-induced allergic proctocolitis (FPIAP) with documented blood in the stool, more children with FPIAP developed IgE-Food Allergy (IgE-FA) (11%) compared with healthy children.
Key points (from commentary by MT Kraft and D Stukus):
“Although conventional teaching is to wait until 12 months of age to reintroduce dairy to infants with FPIAP, it can likely be introduced much earlier.”
The diagnosis of FPIAP was associated with with an increased risk of IgE-FA, “although diagnosis was not confirmed through oral food challenges”
My take: Children with FPIAP are more likely to receive a diagnosis of IgE-FA. Prolonged restriction of milk, when no longer required, could contribute to this; in addition, some children are mislabeled as food allergic without appropriate confirmation (based on faulty testing).
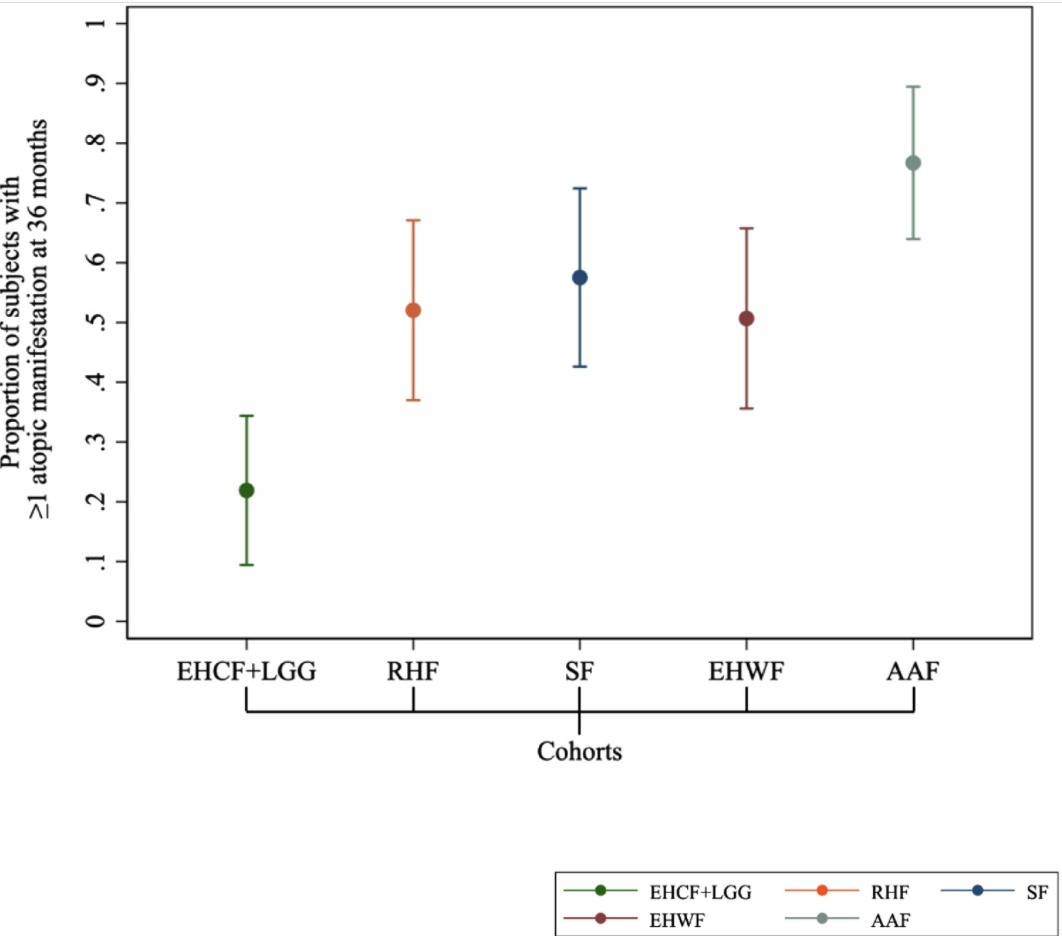
Methods: In a 36-month prospective cohort study (n=365), the occurrence of other atopic manifestations (eczema, urticaria, asthma, and rhinoconjunctivitis) and the time of immune tolerance acquisition were comparatively evaluated in children with oral food challenge-confirmed IgE-mediated cow’s milk allergy (CWA). 5 groups were treated with extensively hydrolyzed casein formula containing the probiotic L. rhamnosus GG (EHCF + LGG), rice hydrolyzed formula, soy formula, extensively hydrolyzed whey formula (EHWF), or amino acid–based formula.
Key finding:
The use of EHCF + LGG for CMA treatment was associated with lower incidence of atopic manifestations and greater rate of immune tolerance acquisition.
The risk ratios:
2.37 (1.46-3.86, P < .001) for rice hydrolyzed formula vs EHCF + LGG
2.62 (1.63-4.22, P < .001) for soy formula vs EHCF + LGG
2.31 (1.42-3.77, P < .001) for EHWF vs EHCF + LGG
3.50 (2.23-5.49, P < .001) for amino acid–based formula vs EHCF + LGG
Limitations: non-blinded study, exclusion of patients with anaphylaxis-CMA