In Pediatrics, supplement 3 summarizes 76 articles: Synopsis Book: Best Articles Relevant to Pediatric Allergy, Asthma and Immunology
Some of the studies that are most relevant to pediatric GI doctors I am reviewing for this blog over the next/past few days.
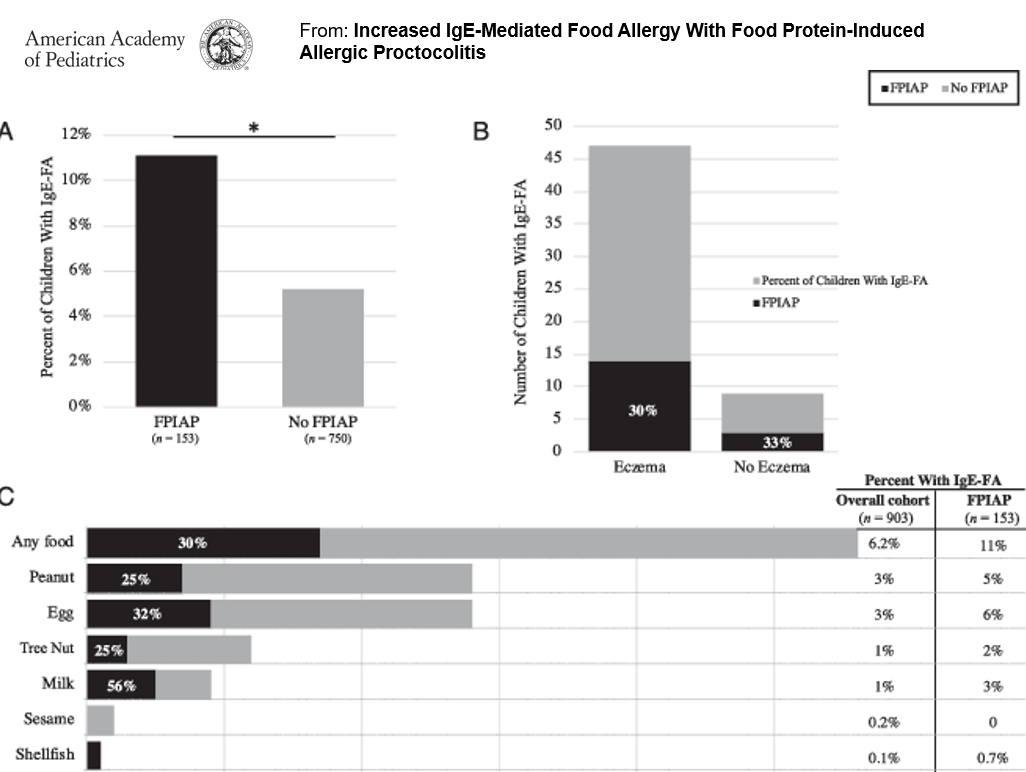
VM Martin et al. Pediatrics 2020; 146: e20200202. Open Access: Increased IgE-Mediated Food Allergy with Food-Protein-Induced Allergic Proctocolitis.
In this study of 153 infants with food protein-induced allergic proctocolitis (FPIAP) with documented blood in the stool, more children with FPIAP developed IgE-Food Allergy (IgE-FA) (11%) compared with healthy children.
Key points (from commentary by MT Kraft and D Stukus):
- “Although conventional teaching is to wait until 12 months of age to reintroduce dairy to infants with FPIAP, it can likely be introduced much earlier.”
- The diagnosis of FPIAP was associated with with an increased risk of IgE-FA, “although diagnosis was not confirmed through oral food challenges”
My take: Children with FPIAP are more likely to receive a diagnosis of IgE-FA. Prolonged restriction of milk, when no longer required, could contribute to this; in addition, some children are mislabeled as food allergic without appropriate confirmation (based on faulty testing).