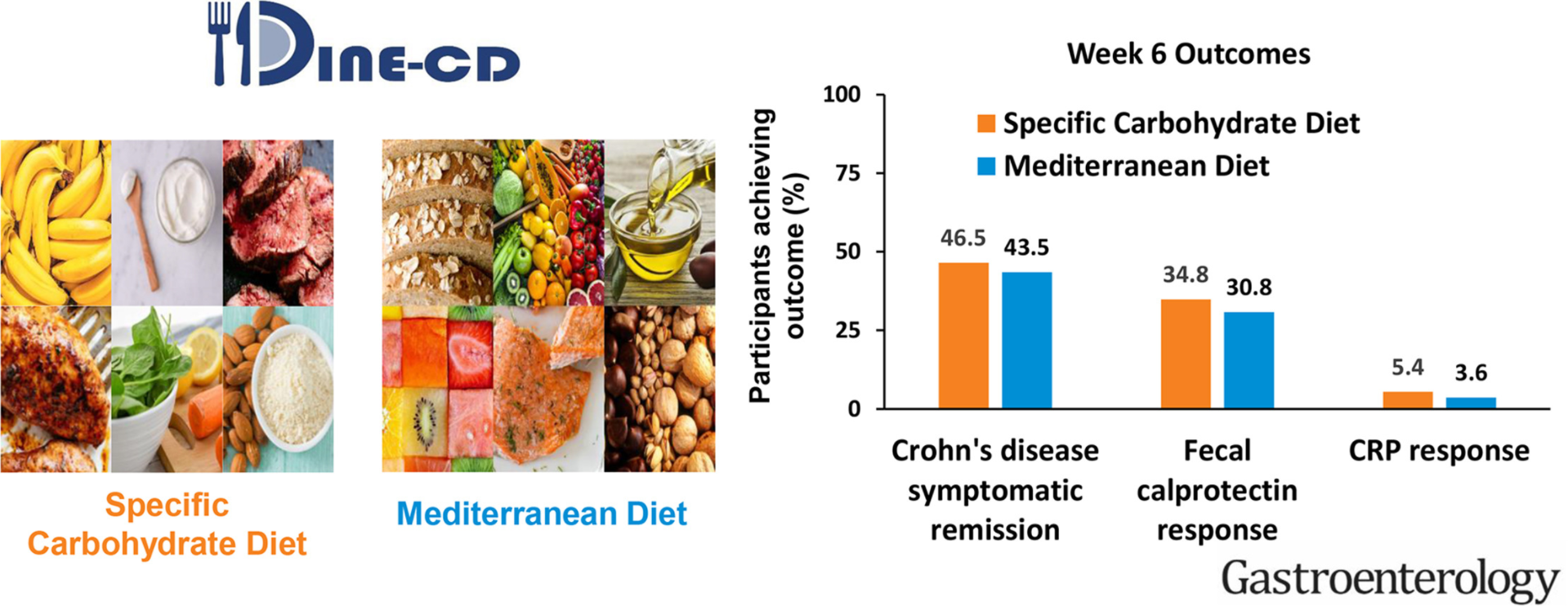
This study compared the effectiveness of the Specific Carbohydrate Diet (SCD) to the Mediterranean Diet (MD) as treatment for Crohn’s disease (CD) with mild to moderate symptoms.
Methods
Adult patients with CD and with mild-moderate symptoms were randomly assigned 1:1 to consume the MD or SCD for 12 weeks. For the first 6-weeks, participants received prepared meals and snacks according to their assigned diet. After 6-weeks, participants were instructed to follow the diet independently. The primary outcome was symptomatic remission at week 6. Key secondary outcomes at week 6 included: fecal calprotectin (FC) response (FC <250 μg/g and reduction by >50% among those with baseline FC >250 μg/g) and C-Reactive Protein (CRP) response (high-sensitivity CRP (hsCRP) <5 mg/L and >50% reduction from baseline among those with hsCRP >5mg/L).
Results
194 patients were randomized, and 191 were included in the efficacy analyses. The percentage of participants who achieved symptomatic remission at week 6 was not superior with SCD (SCD 46.5%, MD 43.5%; P = .77). FC response was achieved in 8/23 participants (34.8%) with SCD and 4/13 participants (30.8%) with MD (P = .83). CRP response was achieved in 2/37 participants (5.4%) with SCD and 1/28 participant (3.6%) with MD (P = .68).
Conclusions
SCD was not superior to MD to achieve symptomatic remission, FC response and CRP response. CRP response was uncommon. Given these results, the greater ease of following the MD, and other health benefits associated with MD, the MD may be preferred to the SCD for most patients with CD with mild to moderate symptoms.
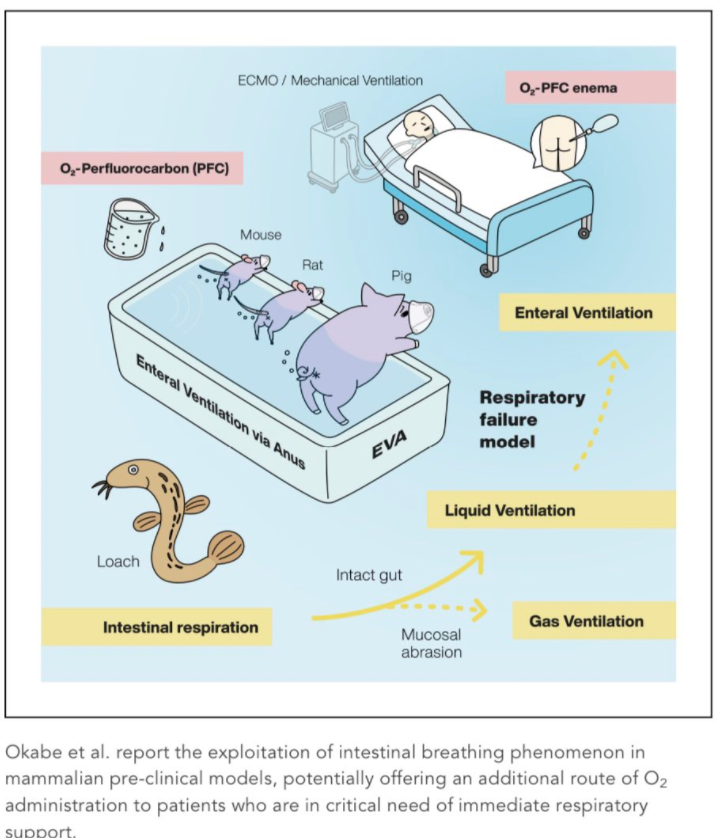
Background: Several aquatic organisms such as loaches have evolved unique intestinal breathing mechanisms to survive under extensive hypoxia. Scientists hope that the approach could one day be used to treat people with low oxygen, without risking the lung damage that can be caused by mechanical ventilators. To date, it is highly controversial whether such capability can be adapted in mammalian species as another site for gas exchange. This study reports the advent of the intestinal breathing phenomenon in mammalians by exploiting EVA (enteral ventilation via anus).
This study showed that administration of oxygen-rich perfluorochemical liquid via the rectum could “increase oxygenation in several mammals including pigs. The level of arterial oxygenation, if scaled for human application, is likely sufficient to alleviate patients with severe respiratory failure. The administration of 200–400 mL PFD to pigs weighing 10–20 kg improved PaO2 by 13 mm Hg (from 57.2 ± 13.5 to 70.8 ± 6.22 mm Hg) and SaO2 by 7% (from 84% to 91%).”
Guideline recommends AGAINST using probiotics for prevention of C difficile infection (CDI)
Guideline cautions AGAINST testing individuals at low risk for CDI (eg. not having diarrhea)
Guideline recommends either vancomycin or fidaxomicin (lower CDI recurrence) for all cases of CDI and consideration of metronidazole for nonsevere cases. Fidaxomicin is recommended for CDI recurrence after vancomycin or metronidazole.
Guideline recommends combination of highly sensitive test and highly specific test for diagnosis of CDI. “CDI-related complications are rare in NAAT-positive, toxin EIA-negative patients, who, even when untreated, may have clinical courses similar to those without CDI…If both are positive, the diagnosis of CDI can be made reliably. If both are negative, CDI is unlikely. Discordant results when NAAT or GDH is positive and toxin EIA is negative require clinical evaluation and consideration of the possibility of colonization or that the patient has CDI but toxin levels are below the limits of detection (see below).
The first study by Bossuyt et al was a substudy (n=36) of the TAILORIX trial. Key findings:
At week 54 of treatment, 36.4% of patients had a radiologic response, 30.3% of patients were in remission, and 71% had endoscopic features of remission
Radiologic remission correlated with infliximab trough level at week 14 (P = .049) when the infliximab trough level cut-off value was set at 7.8 μg/mL (area under the curve, 0.74; 75% sensitivity; 86% specificity; 90% negative predictive value; 57% positive predictive value)
Radiologic response was also associated with continuous infliximab trough levels above 5.0 μg/mL at all time points) (P = .034)
Among patients with both radiologic and endoscopic remission, the median infliximab trough level was 8.5
In this study, one interesting finding was that only half of patients with endoscopic remission achieved radiologic remission, especially since the cohort had a short disease duration at the onset of treatment (median duration of 1.5 months)
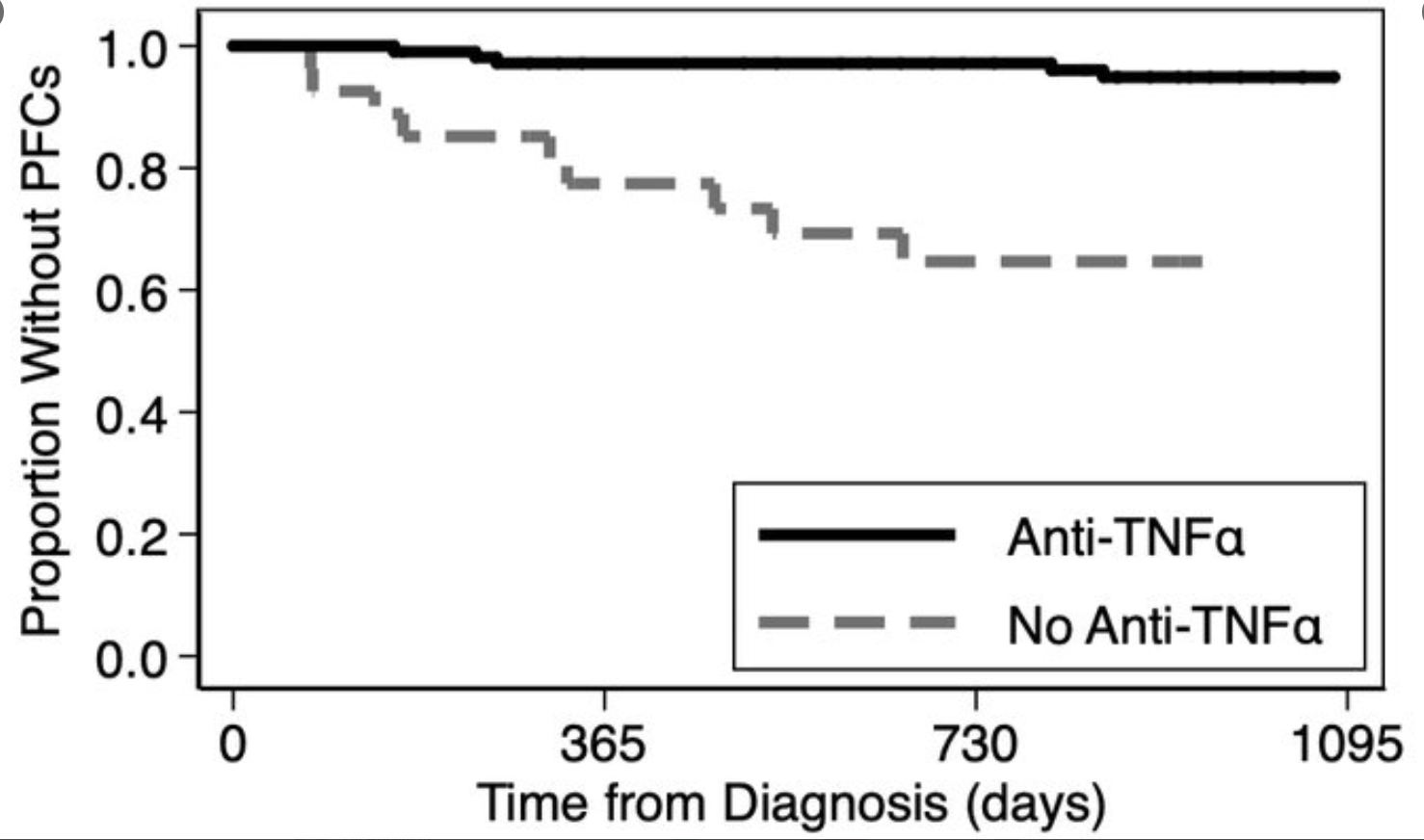
In the second study by Singer et al with 208 pediatric patients with Crohn’s disease, all patients had baseline cross-sectional imaging. Key findings:
26% had perianal fistulas at baseline
14/136 (10%) developed perianal fistulas within 3 years
Non-white race increased the risk of perianal fistula
Non-penetrating perianal lesions (NPLs) increased the risk of perianal fistulas (20% in patients with NPLs vs. 4% in those without NPLs)
Anti-TNF treatment was associated with a decreased risk of perianal fistulas (HR 0.11); this risk reduction was seen in patients with NPLs also (HR =0.14)
My take: Good infliximab levels correlate with better outcomes.
Using a prospective, population-based Swedish cohort (1994-1996) (BAMSE project), the authors analyzed data from 2455 children with complete follow-up evaluation at ages 1, 2, 12, and 16 years.
Key findings:
RAP was reported by 26.2% of children on at least 1 of 3 assessment points, of which 11.3% reported symptoms more than once
Children with RAP at 12 years had persistent symptoms at 16 years in 45% of cases and increased risks for RAP (relative risk, 2.2; 95% CI, 1.7–2.8), any AP-FGID (relative risk, 2.6; 95% CI, 1.9–3.6), and IBS (relative risk, 3.2; 95% CI, 2.0–5.1) at 16 years
Figure 3 summarizes the overlap of RAP at different time points:
**In early childhood (1-2 years of age), 149 (6%) had RAP per parental reports. Only 27 in this group, had RAP noted at 16 years of age which accounted for 7% of the total 16 year old cohort with RAP
**At 12 years of age, 98 (4%) had RAP. 44 (45%) of this group continued with pain at 16 years which accounted for 11% of the total 16 year old cohort with RAP
My take: Most children (84%) with RAP at 16 years of age did NOT report RAP at younger ages; however, in children with RAP at 12 years of age, 45% continued to have RAP at 16 years of age.
This article provides insight into the topic of gastric emptying with a focus on patients with diabetes. A few key points:
Gastric emptying affects glucose homeostasis in patients with diabetes; delayed gastric emptying in patients with type 2 diabetes could have beneficial effects in this regard.
Delayed gastric emptying occurs in 40-47% of adults with diabetes; rapid emptying occurs in 20-22%.
Upper GI symptoms do NOT correlate with gastric emptying. Prevalence of these symptoms is highest in those with normal gastric emptying (43-52% in those with normal emptying compared with 19-28% with delayed emptying, and 20-37% with rapid emptying)
“Functional dyspepsia-like symptoms in gastroparesis may arise not through motility changes but rather through the parallel effects of oxidative stress and inflammation on nocireceptors and on other afferents that produce the symptoms.”
My take: Knowing how quickly the stomach empties rarely helps management. In this review, Dr. Goyal states that “the effective treatment of symptoms in diabetic gastroparesis may be similar to the treatment of functional dyspepsia.”
Also, noted in same issue of NEJM:
TB Corcoran et al.NEJM 2021; 384: 1731-1741. Dexamethasone and Surgical-Site InfectionKey finding: A single dose of dexamathosone (8 mg) did not increase the risk of surgical site infection; this is in contrast to long-term glucocorticoid therapy which is a risk factor for infection and wound dehiscence.
J Salwa et al. NEJM 2021; 384: 1684-6. Designing an Independent Public Health Agency. This article makes compelling arguments for separating health agencies from political influence. The FDA, the CDC, and HHS in the previous administration were pressured and undermined. In contrast, the Federal Reserve Board, which has 14 year terms that require ‘removal only for cause,’ was “reliably [able to] exert federal power because of its institutional features as an independent agency.”
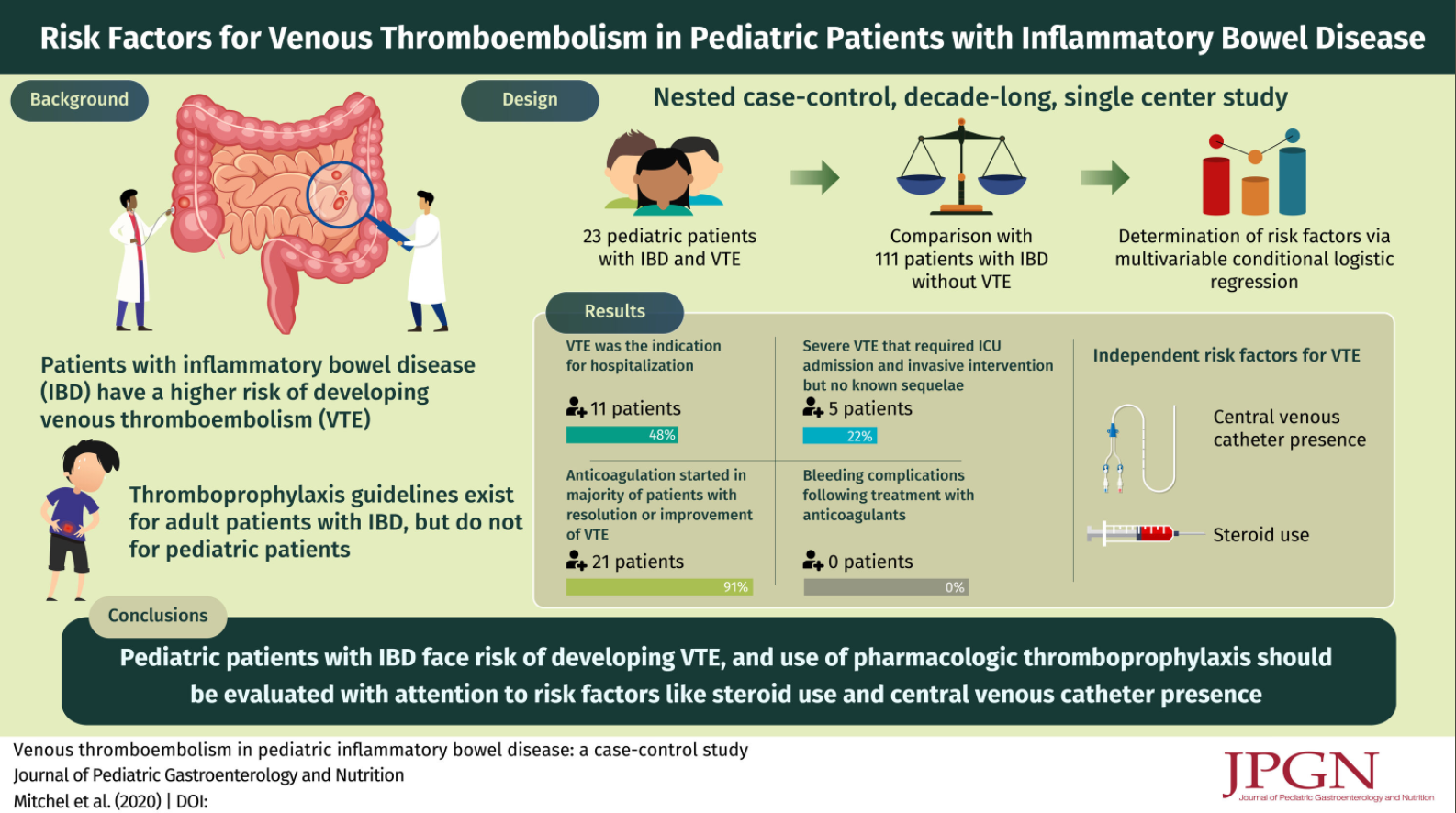
Methods: A nested case-control study comparing hospitalized children with IBD diagnosed with VTE to those without VTE over a decade at a large referral center
Key findings:
Twenty-three cases were identified.
Central venous catheter (CVC) presence (odds ratio [OR] 77.9; 95% confidence interval [CI]: 6.9–880.6; P < 0.001) and steroid use (OR 12.7; 95% CI: 1.3–126.4; P = 0.012) were independent risk factors
Table 2 lists five severe cases which included interventions like balloon angioplasty, stent placement, surgical thrombectomy, and plasmapheresis/subtotal colectomy
The authors note that 1.3% of adolescents/children hospitalized with IBD had VTE
The authors note that ‘inherited prothrombotic disorders are not increased in IBD; “the pathogenesis of VTE in patients with IBD has been associated with increased activation of the coagulation cascade, impaired fibrinolysis, increased platelet count, and dysfunction of the endothelium.”
My take: The absolute risk of VTE is low in the pediatric population; presence of CVC and use of steroids are risk factors and require consideration of, at minimum, nonpharmacologic interventions.