Two recent articles delve into the topic of Pediatric to Adult Care Transition.
M Katz et al. J Pediatr (Epub head of publication) 2021. African American Pediatric Liver Transplant Recipients Have an Increased Risk of Death After Transferring to Adult Healthcare (Thanks to a friend who shared this reference & congratulations to my Emory colleagues and senior author Nitika Gupta on this publication)
This retrospective study examined 101 patients between 1990 and 2015. 64 had long-term followup data available.
Key findings:
African Americans had higher rates of death after transfer than patients of other races (44% mor- tality vs 16%, representing 67% of all cases of death; P = .032)
18 of the 64 (28%) died. Of those 18 deaths, 4 (22%) occurred within the first 2 years after transfer, and 10 (55%) within 5 years of transfer.
There was a high rate of medication nonadherence in patients who died. ” Death in our cohort was typically caused by chronic rejection and graft failure, with a high frequency of severe infections or bleeding events ultimately causing a patient to die.”
The average age of transplant in deceased patients was 15. Transplantation in teenage years could be a risk factor as well.
The authors note that “the years directly after transfer of care from pediatrics to adult medicine are high risk for death and poor patient outcomes. Racial disparities seen in pediatric medicine also hold true after transfer to adulthood.”
This retrospective study with 104 subjects defined suboptimal transition as “either a return to pediatric care or requiring care escalation within 1 year of transfer.
Key findings:
37 (36%) were determined to have a suboptimal transition.
Risk factors: mental health diagnosis (OR 4.15), medication non-adherence (OR 5.15), public insurance (OR 6.60), and higher Physician Global Assessment score at time of transition (OR 6.64).
Comments: This is a small study and included only 26 patients receiving public insurance, which the authors considered as a proxy measure of socioeconomic status.
My take: These studies show the difficulties and potential deadly outcomes that face these young adults during transition from pediatrics to adult care. In many cases, medication non-adherence is a key factor and can be affected by access to care, insurance coverage, and mental health. Most young adults with serious medical problems probably would benefit from keeping their parents actively involved in their care.
Outcomes of VEO-IBD. B Kerur et al. Inflamm Bowel Dis 2021; 27: 295-302.Bowel Disease in North America: A Retrospective Cohort Study The study population included 269 children (105 [39%] Crohn’s disease, 106 [39%] ulcerative colitis, and 58 [22%] IBD unclassified). Key findings:
By the end of follow-up, stricturing/penetrating occurred in 7 (6.6%) children.
Median age at diagnosis was 4.2 years. 71 (26%) were ❤ yrs.
Only 5 (1.7%) had a coexisting immunological disorder.
Over 5 years, cumulative use of an immunomodulator and biologic was 61% and 41% respectively. Exclusive enteral nutrition was used in 10 children (4%).
11.5% (n=19) had a change in diagnosis from UC/IBD-U to Crohn’s disease
The risk of any bowel surgery in Crohn’s disease was 3% by 1 year, 12% by 3 years, and 15% by 5 years and did not differ by age at diagnosis.
The risk of colectomy in ulcerative colitis/IBD unclassified was 0% by 1 year, 3% by 3 years, and 14% by 5 years and did not differ by age of diagnosis.
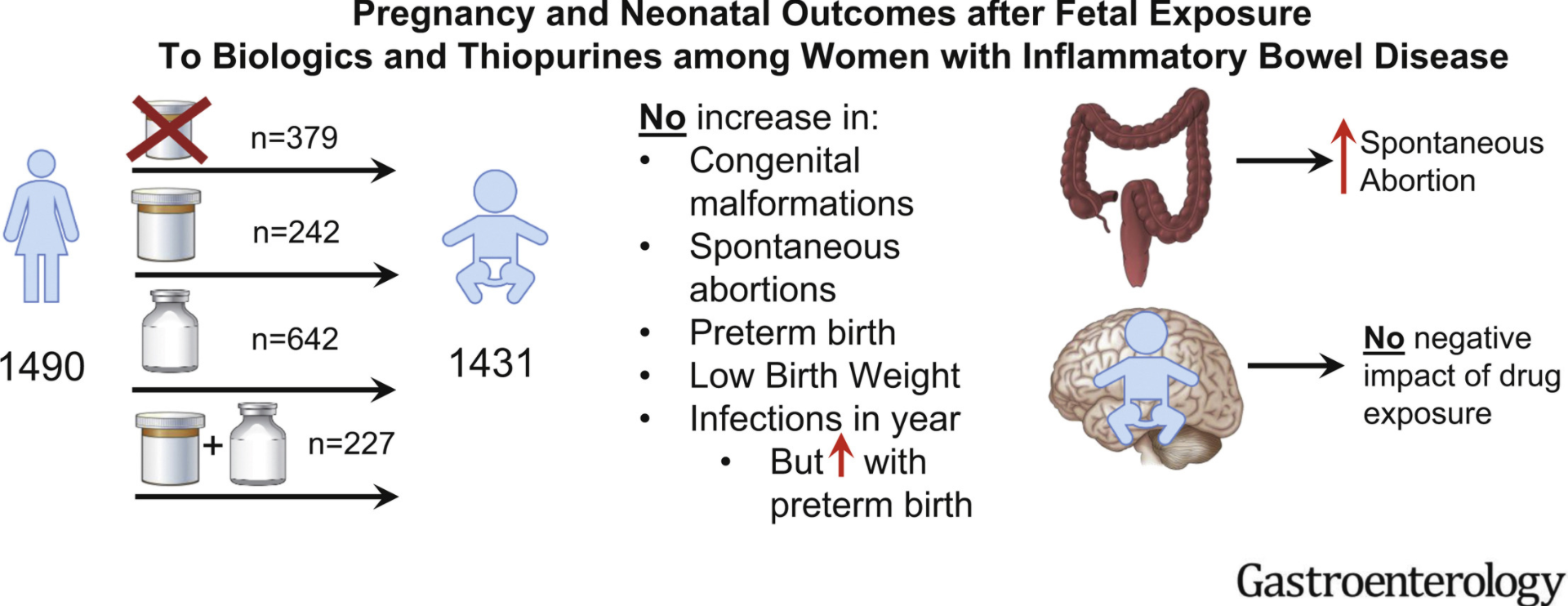
In this PIANO study (2007-2019), pregnant women with IBD were enrolled in a prospective, observational, multicenter study across the United States. PIANO is an acronym for Pregnancy in Inflammatory Bowel Disease and Neonatal Outcomes.
Exposure was to thiopurines (n = 242), biologics (n = 642), or both (n = 227) vs unexposed (n = 379).
In this study, which analyzed Medicaid Analytic eXtract data from 4 states (California, Georgia, North Carolina, and Texas) between 2006 and 2011, the authors identified 14,735 patients with IBD (4672 black [32%]). Key finding: “In patients with Medicaid insurance, where access to IBD-specific therapy should be similar for all individuals, there was no significant disparity by race in the utilization of IBD-specific therapies.”
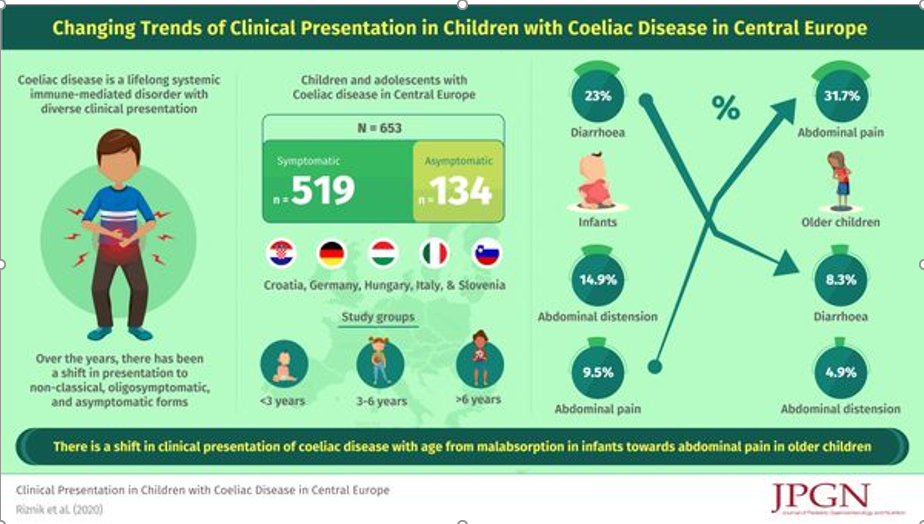
Two recent JPGN articles from the same researchers highlight changes in presentation and deficits of knowledge with celiac disease (CD). Interestingly, the authors chose to spell celiac disease differently in the two articles.
This retrospective study included data from 653 children and adolescents (median age 7 years 2 months; 63.9% girls) from Croatia, Germany, Hungary, Italy, and Slovenia were available for the analysis. Key findings:
One fifth (N = 134) of all children were asymptomatic.
In symptomatic children, the most common leading symptom was abdominal pain (33.3%), followed by growth retardation (13.7%) and diarrhoea (13.3%). Many children (47.6%; N = 247) were polysymptomatic.
Symptoms and signs of malabsorption (eg. diarrhea and distention) were significantly more common in younger (P < 0.001)
This study derived data from a longitudinal cohort; the sample for this study followed women with and without endometriosis who completed extensive surveys (n=323) and excluded women with celiac disease or inflammatory bowel disease. Cases of IBS were based on patient reports of Rome IV criteria, though 81% were confirmed via medical record review.
Key findings:
“More adolescents with endometriosis (54 of 224; 24%) had comorbid IBS compared with adolescents without endometriosis (7 of 99; 7.1%). The odds of IBS was 5.26-fold higher among participants with endometriosis than without (95% CI, 2.13–13.0).”
“For participants with endometriosis, each 1-point increase in acyclic pain severity increased the odds of IBS by 31% (adjusted odds ratio, 1.31; 95% CI, 1.18–1.47).”
The association of endometriosis with IBS was based on Rome IV criteria, as such, the authors assert that this is “not merely a diagnostic bias” However, some of the increase may be related to referral patterns.
Useful points:
“In the adult literature, pain in the pelvis, menstrual-related symptoms, symptoms related to sexual intercourse, ovarian cysts, and subfertility seem to distinguish women with endometriosis from other GI conditions.”
“Chronic pain syndromes were more prevalent in girls with endometriosis and IBS. Rates of migraine headaches, sleep disturbance, and urinary symptoms were higher…[and] had higher prevalence rates of mood disturbance.”
Why is there overlap between these disorders?
The authors speculate that “the inflammatory process likely plays a role…and central pain sensitization may play a crucial role in the two diseases”
My take: Adolescents with endometriosis have a higher likelihood of IBS. Acyclic pain is a strong predictor of IBS.
A recent commentary (JM Zhu et al. NEJM 2021; 384: 11: 981-983. Private Equity and Physician Medical Practices — Navigating a Changing Ecosystem) describes the restructuring of medical practices with a major decline in independent practices due to the growth of hospital-affiliated employees and private-equity investment in medical specialties.
Key points:
Between July 2016-January 2018, “hospitals and health systems acquired more than 8000 practices…Roughly 14,000 physicians left private practice”
Private-equity investment in medical practices has emerged as an alternative source of investment “that allows physicians to continue to hold equity and benefit financially from future transactions.”
Potential consequences of private-equity investment in medical practice:
Reduction in competition
Leverage market power with insurers & possible higher costs
Possible additional pressures on physicians to improve profits and reduction of physician autonomy
Possible improvements in value with operational improvements including sharing industry knowledge with smaller practices, adopting technology infrastructure, and helping practices assume risk with value-based payments
Possible prioritization of patients with better payer mix and lower complexity
My take: Mergers and acquisitions whether through hospitals or private equity make me worried that physicians will be squeezed between delivering profits and providing the best service for our patients.
This was a retrospective cohort study which included 169 patients who never smoked actively, 91 patients (54%) were exposed to passive smoking.
Key finding:
Exposed patients were more likely to undergo intestinal surgery than nonexposed patients (67% vs 30%; P < 0.001). Multivariate Cox regression analysis revealed that passive smoking was an independent risk factor for intestinal surgeries (hazard ratio, 1.7; 95% CI, 1.04–2.9; P = 0.034)
Smoking has long been identified as one of the strongest environmental risk factors for both the development of Crohn disease (CD) and the worsening of the disease course.
Studies in smokers with CD have reported that the risk of flares and complications matches that of nonsmokers with CD after 1 year of abstinence.
It would be reasonable to expect that a similar risk reduction exists for patients who can become passive-smoke-free. In addition, their likelihood of remaining smoke-free themselves is increased if they live in a smoke-free household.
My take (from editorial): “Clinicians should consider widening the scope of smoking cessation counseling to include not just patients but also their cohabitants.”
Using the Inform Diagnostics database, which is a national electronic repository of histopathologic records from patients distributed throughout the entire United States, the authors performed a case-control study among 302,061 patients undergoing bidirectional endoscopy on the same day.
The database contained 3860 ulcerative colitis (UC) patients, 3330 Crohn’s disease (CD) patients, 1476 patients with indeterminate colitis with respect to UC or CD, and 5296 MC (microscopic colitis) patients.
Key findings:
EoE was less common in the overall IBD, CD, and MC case populations than the control population. Adjusted odds ratios (compared to control) :
EoE and IBD aOR 0.64
EoE and Crohn’s aOR 0.41
EoE and UC aOR 0.97
EoE and Indeterminate Colitis aOR 0.29
EoE and MC aOR 0.68
My take: (partly from authors) “Unexpectedly, the present analysis revealed statistically significant inverse relationships between EoE and CD or MC, but not UC.” Because endoscopy is often undertaken in those with a suspicion of IBD, EoE can be identified in the IBD population surreptiously; however, its frequency is likely less than in the general population.
This is a very useful article with recommendations for central venous access in children. The main recommendations are summarized in Table 3 & listed below; however, there is a lot of detailed information in the article on frequent issues like schools, travel (including dealing with TSA), sports, and even swimming. In addition, the article delineates recommendations for management and prevention of line complications.
1. Recommendations for venous access:
Tunneled, single lumen, cuffed silicone catheters should be used for children with IF.
Upper extremity access is the preferred location when available.
2. Recommendations pertaining to routine CVC care:
Proper technique and hygiene surrounding CVC care are of paramount importance in preventing CVC-associated complications. Caregivers should receive directed education regarding CVC care before initial discharge, with subsequent reinforcement education as needed.
CHG impregnated supplies (disk, sponge, or dressing) should be considered for central line dressing in pediatric IF patients.
Routine surveillance of central venous access should be performed by US. MR, CT, or traditional venography should be reserved for when further delineation of access is required.
3. Recommendations regarding general considerations—sports, travel, and emergencies:
All children with IF should be provided with an emergency letter that details the specific needs of the individual child in case of an emergency. (See at bottom for example -Figure 1)
Discuss with families the risks of swimming and sports participation with strategies to protect the dressing and central line.
All travel plans should be discussed with the intestinal rehabilitation team well in advance of travel to facilitate discussion of a plan of care in case of emergency.
4. Recommendations regarding central line-associated bloodstream infections:
All children with IF and CVC who develop a fever (≥38.0°C) should be admitted to the hospital and assessed for bacteremia with central and peripheral blood cultures while receiving broad-spectrum empiric antibiotics through the CVC for at least 48 h, awaiting culture results regardless of other infectious sources.
If clinically stable, discuss with the patient’s IRP before line removal for CLABSI.
Prophylactic lock therapy with ethanol or other nonantibiotic locks should be strongly considered in all children with IF who have had at least one central line-associated bloodstream infection or are at high risk for infection.
5. Recommendations pertaining to central line mechanical complications:
In children with IF, CVC should be repaired whenever possible to preserve central venous access.
Children with IF and a newly identified CRT should be treated with low molecular weight heparin for at least 6 weeks with guidance from a hematologist.
Children with IF who have persistence of at least one chronic thrombus should be maintained on prophylactic anticoagulation with low molecular weight heparin.
Children who have lost multiple sites of central venous access should be considered for referral to an intestinal transplant center for evaluation and management
6. Recommendations for central venous access program management:
All centers following children with IF should, at a minimum, track the number of outpatient CLABSI per 1000 catheter days.
With regard to swimming: “Swimming introduces an incompletely defined but potentially severe risk to those requiring chronic central venous access. Contamination of various chlorine-treated (swimming pools), stagnant (lakes and ponds), and flowing (oceans and rivers) bodies of water with human pathogens has been well documented, though proper maintenance may minimize outbreaks. The potentially fatal risk of such contaminants gaining access to central circulation via the CVC is unclear…Parents seeking guidance are confronted by mixed messaging from support programs, online resources and blogs, and even IRP. These conflicting recommendations and practices reflect the paucity of data to guide a safe and clear approach for swimming with a central line…[in one study of 16 home PN programs] swimming in low-risk situations [was permitted but] recommended immediate site cleaning and dressing change following water exposure and avoidance of submersion for 4–6 weeks after CVC placement. Ultimately, the decision to permit children with IF to swim lies with the parent or guardian.”
For pets (like Charlie), this article notes that “steps should be taken to promote line integrity in the presence of pets. Particularly in the setting of pets that may attempt to chew or play with tubing, adequate physical protection of the insertion site and catheter itself is recommended. Any line or tubing puncture by an animal should prompt immediate evaluation. Family awareness of zoonotic disease risk and advocacy of handwashing before and after animal care should be made clear.”Figure 1 -Emergency Letter Template
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
This small (n=28) retrospective study provides useful information on the persistence of feeding problems in children with short bowel syndrome (SBS). The authors defined a pediatric feeding disorder (PFD) as “reliance on enteral feeds to sustain nutrition, reliance on high-calorie oral supplements to sustain nutrition, or feeding skill dysfunction resulting in not consuming an age-appropriate diet.” Patients who remained on PN were considered to have a PFD as well.
Key findings:
Of the 21 patients (75% of total cohort) who were weaned off parenteral nutrition, 57.1%, 81.0%, 90.5%, and 100.0% achieved this by 12, 24, 36, and 48 months of age, respectively. Median age at time of weaning PN was 10.8 months.
Of the 13 patients who were weaned off enteral nutrition (EN), 30.8%, 69.2%, 76.9%, and 100.0% achieved this by 12, 24, 36, and 48 months, respectively. Median age of weaning EN was 15.7 months. Overall, about a third of patients required EN beyond 2 years of life.
The prevalence of PFD (of entire cohort) was 100.0%, 76.5%, 68.8%, and 70.0% at 1, 2, 3, and 4 years of age, respectively
My take: When parents ask how long it will be before my child is off PN and eating by mouth, this study’s results could be useful.
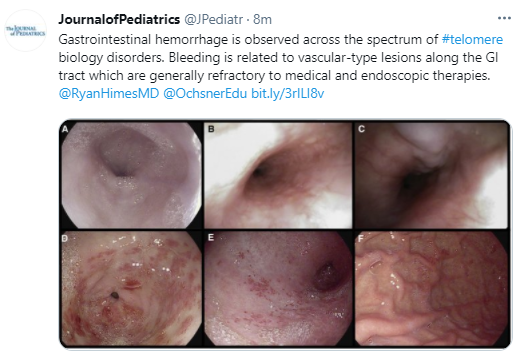
Background: Telomere biology disorders are a complex set of illnesses defined by the presence of very short telomeres; these individuals are at very high risk of bone marrow failure, cancer, and pulmonary fibrosis. There are 15 known genes which can experience damaging mutations, or other abnormalities, that can cause very short telomeres (for example the telomerase genes TERC and TERT). The most widely recognized telomere biology disorder is known as dyskeratosis congenita (DC); others include Hoyeraal-Hreidarsson syndrome, Revesz syndrome, and Coats plus.
Key findings:
Sixteen patients who experienced GI hemorrhage were identified at 11 centers. Ten patients had a history of hematopoietic cell transplantation.
Initial GI bleeding occurred at a median of 12.5 years.
Angiodysplasia of the stomach and/or small bowel was described in 8 of the 12 patients who underwent endoscopy; 4 had esophageal varices. The lesions were often diffuse and widespread (see Figures 1 & 2).
GI bleeding appeared to be more prevalent in those with TINF2, CTC1 or STN1 mutations (12 of 14 with genetic testing).
Recurrence was common, and the overall long-term outcome for affected patients was poor. 12 of 16 were deceased at time of data collection (median age of 16.5 years at time of death), though the proximate cause of death was not reported.
No single intervention was uniformly associated with cessation of bleeding, although 1 patient had a sustained response to treatment with bevacizumab. Other treatments that were tried included endoscopic treatments, thalidomide, octreotide, proton pump inhibitors, sirolimus and hormonal treatments.
My take: GI bleeding in these rare disorders is a difficult clinical problem.