Washington Post: Children Under Fire
Almost two dozen kids are shot every day in the U.S. This 4-year-old was one of them.


Washington Post: Children Under Fire
Almost two dozen kids are shot every day in the U.S. This 4-year-old was one of them.
JE Heubi et al (JPGN 2017; 65: 321-6) performed a phase 3, open-label, nonrandomized trial on the efficacy and safety of oral cholic acid for patients with Zellweger Spectrum disorders (n=20) and patients with bile acid synthesis disorders (BASD) (n=50). Cholic acid dosing: 10-15 mg/kg/day. Most common BASD were 3β-HSD (n=35), and 5β-reductase (n=10). Based on this work, cholic acid is an FDA-approved agent.
Key findings:
My take: Cholic acid helps the liver in these disorders which is particularly important for BASD. It is unclear if this improves outcomes in patients with Zellweger spectrum disorders as it has not been shown to improve extrahepatic disease.
Related blog post:

Eiffel Tower
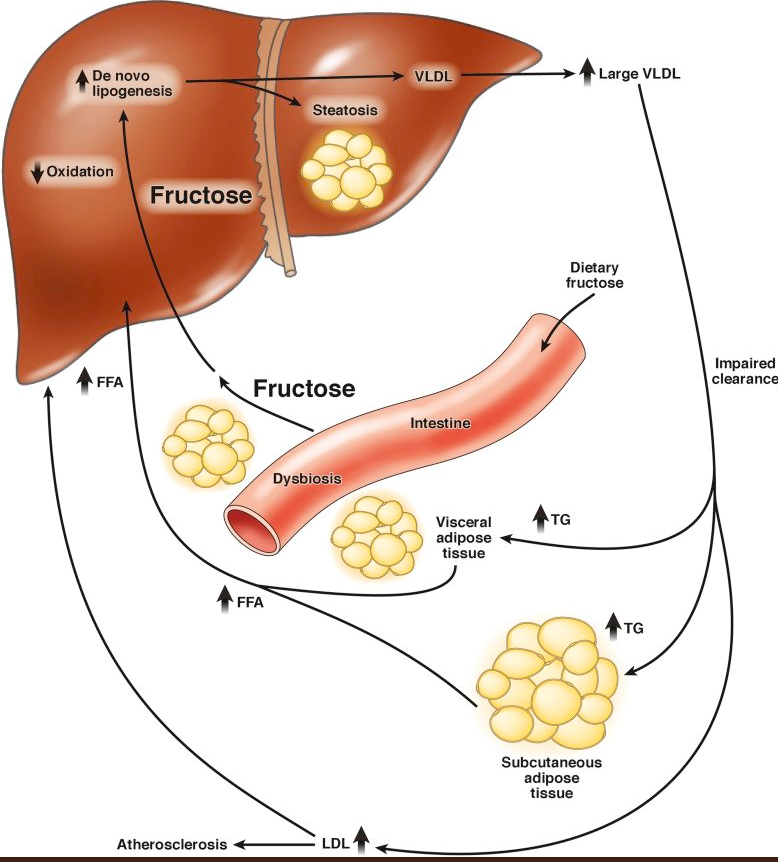
A recent study (J-M Schwarz et al. Gastroenterol 2017; 153: 743-52, editorial MB Vos, IR Goran Gastroenterol 2017; 153: 642-5 ) showed that restriction of fructose quickly improved fatty liver disease.
Several points from the editorial:
The study is summarized in a recent AGA Journals Blog: Can Restricting Fructose Intake Reduce Fatty Liver Disease in Children?
An excerpt:
Jean-Marc Schwarz et al performed a clinical trial to investigate the effects of reducing fructose intake for 9 days in obese Latino and African American children with habitual high sugar consumption (fructose intake >50 g/day). They measured the effects of isocaloric fructose restriction on de novo lipogenesis, liver fat, visceral fat, subcutaneous fat, and insulin kinetics.
In their study, 41 children, 9−18 years old, had all meals provided for 9 days. The meals had the same energy and macronutrient composition as their standard diet, but with starch substituted for sugar, yielding a final fructose content of 4% of total kilocalories. The authors measured metabolic factors before and after fructose restriction. They measured liver fat, visceral fat, and subcutaneous fat by magnetic resonance spectroscopy and imaging.
Schwarz et al found that on day 10 of the diet, liver fat decreased from a median 7.2% at baseline to 3.8%, and visceral fat decreased from 123 cm3 at baseline to 110 cm3. Liver fat decreased in all but 1 of the 38 participants for whom paired data were available…
De novo lipogenesis decreased significantly after 9 days of fructose restriction; the de novo lipogenesis area under the curve value on day 10 decreased from 68% at baseline to 26% after the diet, in childen with low or high baseline levels of liver fat.
Insulin secretion during fasting and in response to an oral glucose tolerance test decreased significantly in children with low and high baseline levels of liver fat…
In an editorial that accompanies the article, Miriam B. Vos and Michael I. Goran say that it will be important to determine whether the effects of fructose reduction are sustained past 9 days…Vos and Goran state that it is important for physicians, nutritionists, schools, and parents to find ways to reduce fructose in the diets of children and patients with NAFLD.
Related posts:

From Gastroenterology & Endoscopy News: New JAK1 Inhibitor Treats Most Challenging Crohn’s Patients
An excerpt:
An experimental oral JAK1 inhibitor, upadacitinib (AbbVie), has been tested in the most clinically challenging patients with Crohn’s and yielded impressive results. The drug led to a clinical response in 61% of these patients and remission in 22%, the new data show…
William Sandborn, MD, chief of gastroenterology at the University of California, San Diego, who led the study. “It seems to be a really effective drug in a very difficult-to-treat patient population, and the oral route of administration is attractive.”
Dr. Sandborn’s group presented the findings at the 2017 Digestive Disease Week (abstract 974h).
The CELEST trial enrolled 220 patients with active, moderate to severe Crohn’s disease. Patients received 16 weeks of induction therapy with one of five dosing regimens of upadacitinib or a placebo…
Dr. Sandborn called the findings particularly impressive given that the study participants are the most refractory patient population ever recruited in a trial for Crohn’s disease. “And this is also one of the first trials to meet new FDA requirements for demonstrating clinical remission using patient-reported outcomes as well as endoscopic improvement,” he noted.
My take: It is exciting that another oral agent may be helpful. Tofacitinib, a different JAK1 inhibitor, has data supporting its use in ulcerative colitis but not with Crohn’s disease.
Related blog posts:

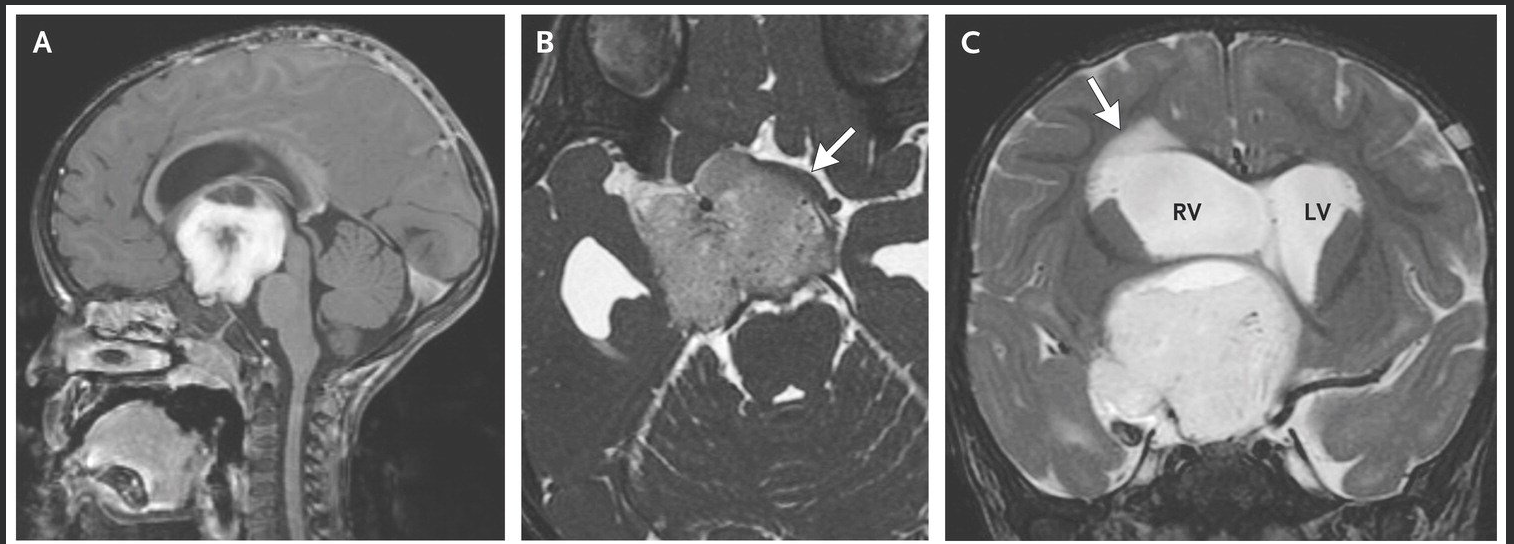
A fascinating case report (MA Curran et al. NEJM 2017; 377: 1468-77) provides a useful exercise in understanding how to evaluate difficult cases of “failure to thrive.”

From NEJM twitter feed
In essence, a 19 month girl with good linear growth had stopped gaining weight around 7 months of age. After exhaustive evaluation, detailed in this report, the patient had an MRI which revealed a brain tumor and she was diagnosed with diencephalic syndrome. Key features include good appetite/caloric intake, happy appearance, and cachexia.
The discussion explains that in most children, poor weight gain results from poor caloric intake, which can be related to social issues including poverty, neglect, parental mental health issues, and lack of understanding by caregivers.
In children with good caloric intake, the potential reasons for poor growth are reviewed:
Despite the numerous potential causes, beyond basic laboratory assessment, “extensive testing is usually not warranted: in one study, only 1.4% of additional laboratory tests were helpful in making the diagnosis.”
In many cases of diencephalic syndrome, symptoms like vomiting may be present on an intermittent basis as well as nystagmus or strabismus; these symptoms develop due to obstructive hydrocephalus.
My take: In children with good caloric intake, diencephalic syndrome is a rare but important etiology.
I wanted to share several tweets from this year’s ACG World Congress that looked helpful.
Topic: SBBO and IBS-D

A positive breath test is the ONLY variable that can predict response to Rifaximin in IBS-D: ACG and Mark Pimenthal. tweet from @AllRezale, MD
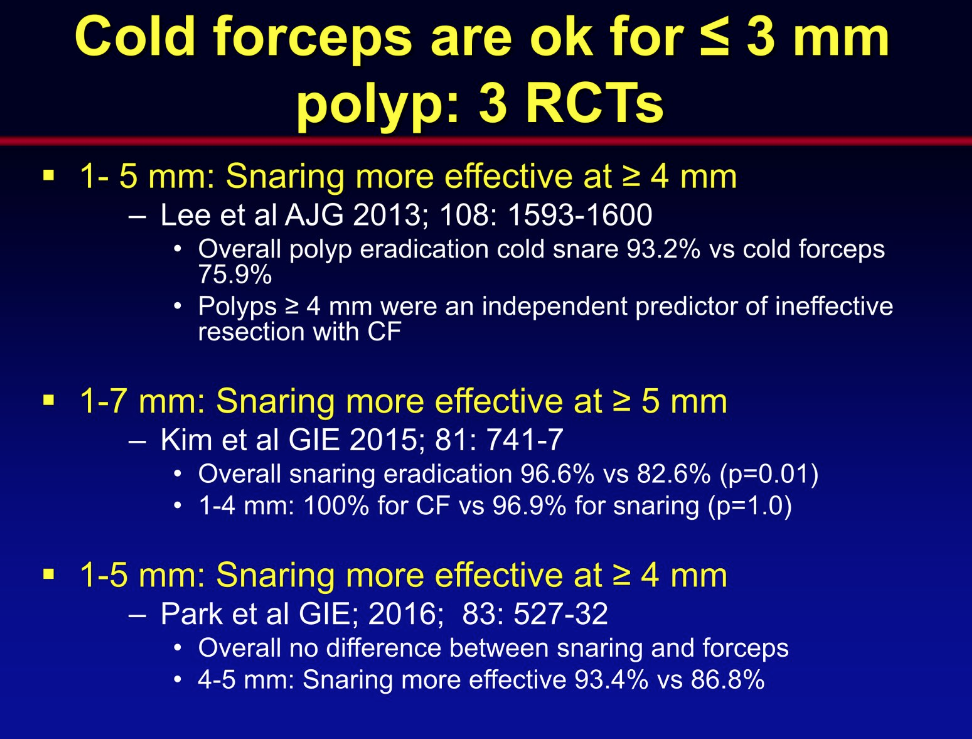
Topic: Polyps -slides recommend cold forceps for polyps 1-3 mm and cold snare for 4-5 mm polyps.


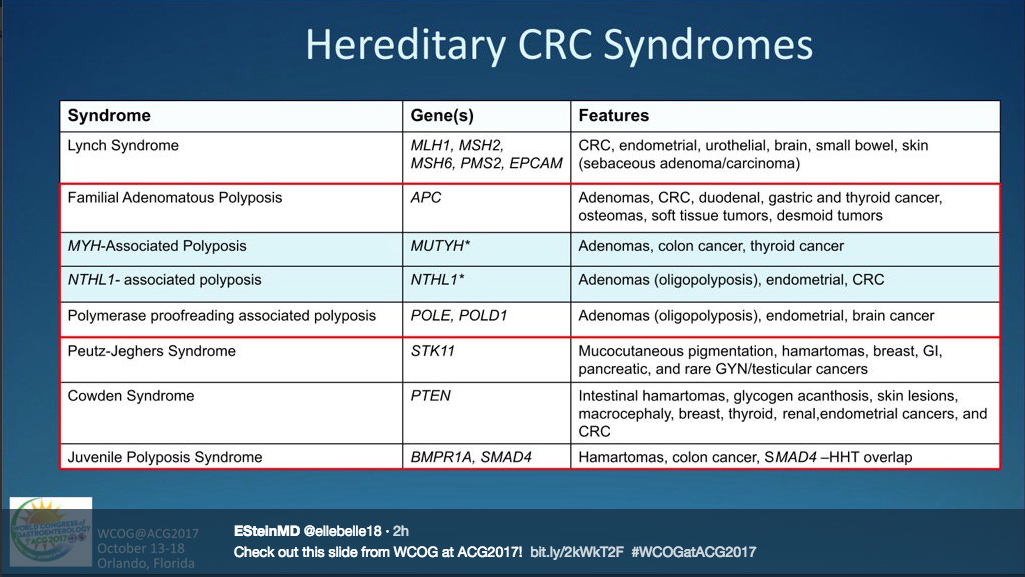
Topic: Hereditary Colorectal Cancer Syndromes
Topic: Aggressive fluids for pancreatitis
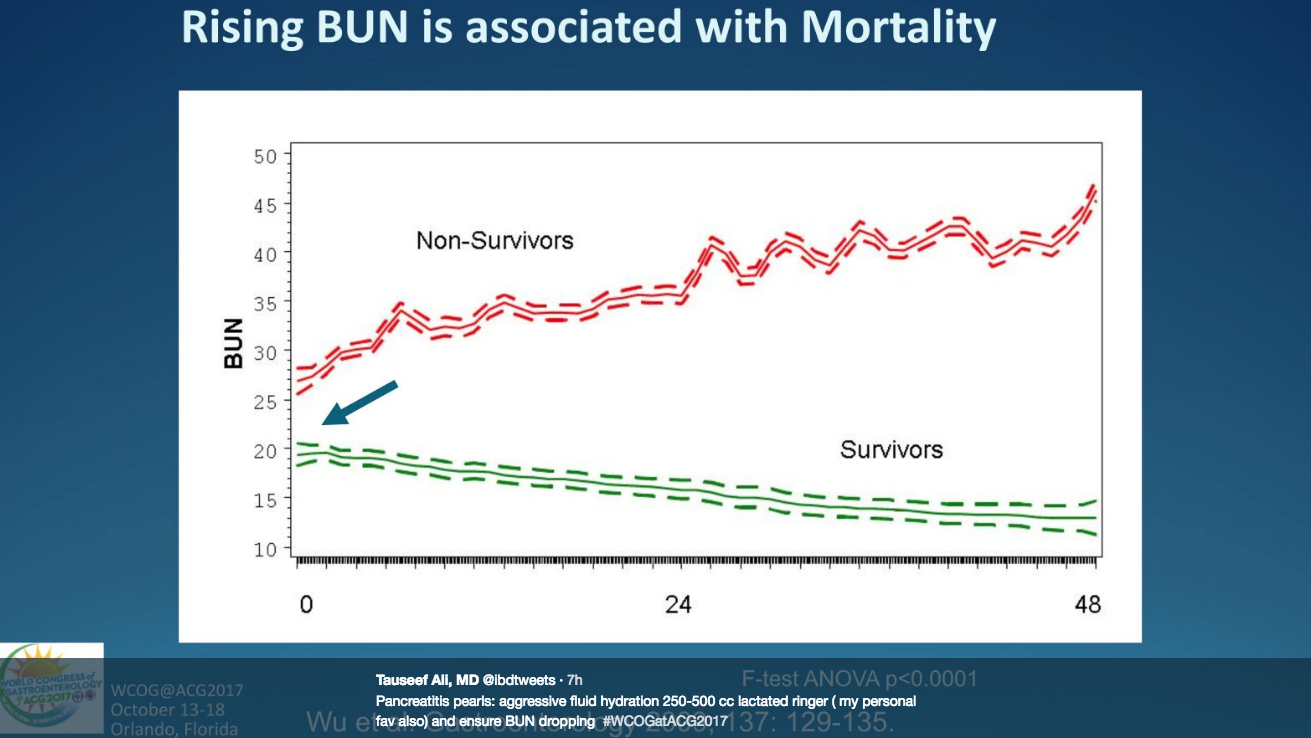
Rising BUN is Associated with mortality with pancreatitis. Tauseef, Ali @ibdtweets: “Pancreatitis pearls: aggressive fluid hydration 250-500 cc lactated ringer’s (my personal favorite also) and ensure BUN dropping #WCOGatACG2017”
IJN Koppen et al. Journal of Pediatric Gastroenterology & Nutrition: October 2017 – Volume 65 – Issue 4 – p 361–363
Abstract:
According to international guidelines, polyethylene glycol (PEG) is the laxative of first choice in the treatment of functional constipation in children, both for disimpaction and for maintenance treatment. PEG acts as an osmotic laxative and its efficacy is dose dependent. PEG is highly effective, has a good safety profile, and is well tolerated by children. Only minor adverse events have been reported. Overall the use of PEG in children has been reported to be safe, although in patients predisposed to water and electrolyte imbalances monitoring of serum electrolytes should be considered.
Because this topic is of great importance to the families that are seen by pediatric gastroenterologists (and pediatricians), I wanted to review this brief article which describes the efficacy and safety of polyethylene glycol (aka miralax).
Key Points:
Safety:
Combatting Myths:
Clinical Pearl: Stimulant Laxatives After Repaired Anorectal Malformations:
My take (borrowed from the authors): “PEG has rapidly become the treatment of first choice for children with functional constipation.”
Related blog posts:

An interesting case report (DL Saly et al. NEJM 2017; 377: 1379-85) describes a 61 year old woman with multiple medical problems who developed numbness and tingling in hands/feed which progressed to unsteady gait and inability to stand.
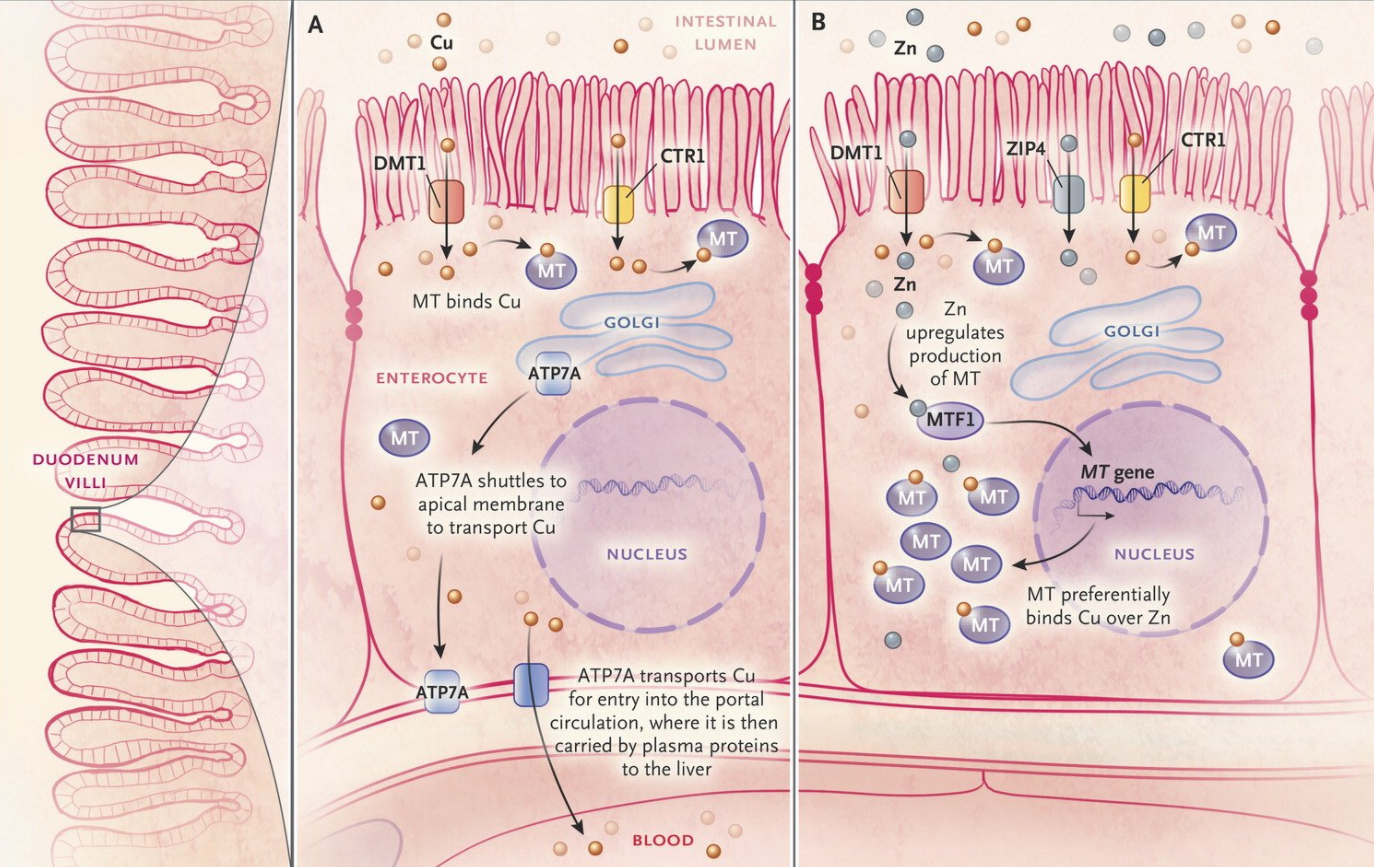
Her medical problems included end-stage renal disease requiring dialysis, COPD, hepatitis C, depression,reflux, breast cancer, hypertension, and chronic back pain. Due to dysgeusia and suspected zinc deficiency associated with dialysis, she had been started on zinc therapy and this was doubled when she did not improve.
Ultimately she was diagnosed with copper deficiency which can result from zinc toxicity, “because zinc upregulates the protein to which copper binds in enterocytes, and an excess of zinc forces copper to be trapped in the enterocyte and unavailable for absorption.”
My take: Too much zinc (as well as other micronutrients/vitamins) can result in adverse effects.

Related blog posts:
A recent commentary (S Woloshin et al. NEJM 2017; 377: 1114-7) examines the fate of FDA postapproval studies.
“Both Congress and the Food and Drug Administration (FDA) have sought to accelerate the “availability of new drugs by allowing sponsors to wait to resolve many questions about safety and benefit until after their drugs receive marketing approval.”
However, this commentary points out that many times these studies are never completed. The authors examined these studies since 2009. Key finding:
The authors note ‘the slow irregular pace of postapproval studies contrasts starkly with the short, rigid deadlines and other shortcuts used to speed marketing approval.” They suggest that the FDA impose fines and establish shorter deadlines. They indicate that the current administrations stated view that the FDA is ‘slow and burdensome’ could necessitate even more reliance on postapproval studies by loosening the evidence for new medication approvals.
In the same issue, the FDA responds that there have been improvements and that since 2015, “88% of postmarketing requirements overall…were progressing according to their original schedules.”
My take: More rapid approvals will inevitably lead to more medications with unrecognized safety signals. These postapproval studies are crucial in identifying infrequent but important adverse effects.
Related blog posts:
While anti-immigrant sentiment has become more widespread among many, in medicine it is clear that immigrant physicians play an important role. This is discussed in a recent NY Times article: Why America Needs Foreign Medical Graduates
The key points:
An excerpt:
The American system relies to a surprising extent on foreign medical graduates, most of whom are citizens of other countries when they arrive. By any objective standard, the United States trains far too few physicians to care for all the patients who need them. We rank toward the bottom of developed nations with respect to medical graduates per population…
A 2015 study found that almost a quarter of residents across all fields, and more than a third of residents in subspecialist programs, were foreign medical graduates…
About a quarter of all doctors in the United States are foreign medical graduates.
My take: Physicians from other countries improve the health of our entire country. In addition, many physicians who train in the U.S. return abroad and help improve health in their home countries.
Related blog posts:


