

Programming for Fatty Liver Disease May Occur Prior to Birth
A recent study (KP Newton et al. J Pediatr 2017; 187: 141-6; associated editorial pg 13-15)) in a multicenter retrospective cross-sectional study of children (n=538) with biopsy-proven nonalcoholic fatty liver disease (NAFLD) showed that birth weight influenced the development of NAFLD. The participants were enrolled in the Nonalcoholic Steatohepatitis Clinical Research Network (NASH CRN).
Key findings:
- There was increased NAFLD among both low birth weight (LBW) and high birth weight (HBW).
- LBW occurred more commonly in the NAFLD cohort 9.3% compared with the general population prevalence 6.1%.
- HBW occurred more commonly in the NAFLD cohort 14.9% compared with the general population prevalence 10.5%
The authors speculate that the explanation/mechanisms for increase in both LBW and HBW are likely to differ. It has been recognized that LBW is associated with higher cardiovascular disease and type 2 diabetes. HBW start bigger and often stay bigger; that is, there are increased risks of more severe obesity.
There are numerous limitations to this study -there is a lot of data that is not available, including gestational age, maternal weight, breastfeeding exposure, and antibiotic administration.
My take: These findings add to the literature that risks for NAFLD along with other metabolic problems may be present at birth. Is there a way to modify this risk?
Related study: ET Jensen et al. J Pediatr 2017; 187: 50-7, editorial pg 10-12. In this study of 535 ten-year-old children, enrolled in a prospective multicenter extremely low gestational age newborn cohort study, the authors found that maternal overnutrition and undernutrition affected the brain health of these children. The authors used neurocognitive assessment tools.
- Children born to women with a pregravid BMI >30 scored “lower on measures of general cognitive ability, executive functioning, fine motor function, and academic achievement.”
- Children born to women with inadequate maternal weight gain during pregnancy had “lower language and academic achievement.”

Hidden Falls, Highlands NC
Likelihood of Genetic Disease with Early-Onset Pancreatitis
Another study (MJ Giefer et al. J Pediatr 2017; 186: 95-100) from the INSPPIRE group provides data on early-onset pancreatitis. Specifically, the group presents clinical information on 342 children with acute recurrent pancreatitis or chronic pancreatitis regarding disease burden and associations with genetic mutations.
Key findings:
Genetic disease is much more common in younger ages:
- In subset younger than 6 years, 72 of 102 had genetic diseases identified: PRSS1 in 42, CFTR in 27, SPINK1 in 12, and CTRC in 8.
- In subset 6-11 years of age, 52 of 90 had genetic diseases identified: PRSS1 in 20, CFTR in 23, SPINK1 in 22, and CTRC in 1.
- In subset greater than 12 years of age, 39 of 72 had genetic diseases identified: PRSS1 in 13, CFTR in 24, SPINK1 in 6, and CTRC in 1.
- Testing for newer susceptibility genes were not evaluated as they had not become commercially available: carboxypeptidase 1, claudin 2, carboxylesterlipase, and carboxyesterlipase-hybrid
- SPINK1 is noted to be present in 1-3% of general population; CTRC mutation occur in 0.7% of healthy controls.
Obstructive causes were common. Pancreas divisum was identified in 38 patients but there was not a great deal of difference among the age groups; similarly, other obstructive causes were identified in about one-third of patients and included sphincter of Oddi dysfunction (n=9), gallstones (n=17), pancreaticobiliary malunion (n=12), biliary cyst (n=11), pancreatic stricture (n=2), annular pancreas (n=3), and duodenal diverticulum.
Disease burden:
- Exocrine insufficiency noted in 52 (no strong age predilection)
- Diabetes in 18 (11 of the cases occurred in those >12 years)
- Constant moderate pain noted in 82 (25 in group <6, 27 in 6-12 group, and 30 in group >12 years)
- Constant severe pain noted in 18 (4 in group <6, 5 in 6-12 group, and 9 in group >12 years)
- Average number of hospitalizations in past year was 1 in those ≤12 and 2 in those older than 12.
My take: PRSS1 and CTRC mutations are associated with early onset pancreatitis.
Related blog posts:
- Pancreatitis Update 1 and Pancreatitis Update 2
- Consensus Pancreatitis Recommendations
- Risk of pancreatitis with celiac disease | gutsandgrowth
- INSPPIRE for pancreatitis | gutsandgrowth
- For the pediatric pancreatologists | gutsandgrowth
- Chronic Pancreatitis in Pediatrics -Descriptive Study | gutsandgrowth
- RECURRENT PANCREATITIS AND GENETIC UNDERPINNINGS | GUTSANDGROWTH
- DOES PANCREAS DIVISUM CAUSE PANCREATITIS? | GUTSANDGROWTH
- HOW HELPFUL ARE ANTIOXIDANTS FOR CHRONIC PANCREATITIS PAIN …
- Why an ERCP Study Matters to Pediatric Care

Rotunda dome at the University of Virginia
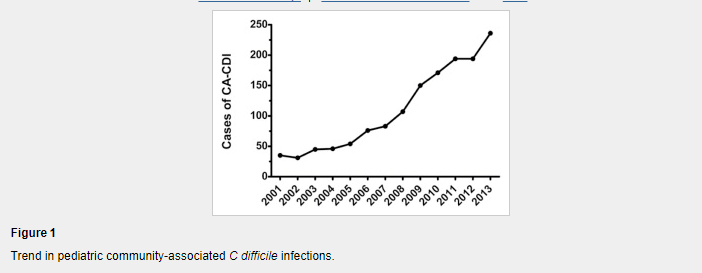
Clostridium difficile Risk Factors in Children
From J Pediatr -full text: Risk Factors for Community-Associated Clostridium difficile Infection in Children (DJ Adams J Pediatr 2017; 186: 105-9)
Methods: We performed a case-control study using billing records from the US military health system database
Results (from abstract):
A total of 1331 children with CA-CDI were identified and 3993 controls were matched successfully. Recent exposure to fluoroquinolones, clindamycin (OR 73.00; 95% CI 13.85-384.68), third-generation cephalosporins (OR 16.32; 95% CI 9.11-29.26), proton pump inhibitors (OR 8.17; 95% CI 2.35-28.38), and to multiple classes of antibiotics, each was associated strongly the subsequent diagnosis of CA-CDI. Recent exposure to outpatient healthcare clinics (OR 1.35; 95% CI 1.31-1.39) or to a family member with CDI also was associated with CA-CDI.
Table 2 lists other medications and their risks; for example, corticosteroids had adjusted OR of 1.22 and H2-receptor antagonists had adjusted OR of 3.33. The OR of fluoroquinolone could not be calculated as 51 cases were exposed compared with 0 controls
In their discussion, the authors note the following:
Our study supports the occurrence of CDI among a population of children who were never hospitalized previously and provides a broad characterization of the medication and epidemiologic exposures associated with pediatric CA-CDI cases. Recent exposure to fluoroquinolones, clindamycin, third-generation cephalosporins, and to multiple classes of antibiotics was associated strongly with the subsequent diagnosis of CA-CDI in children; however, a sizeable minority had no preceding antibiotic exposure.
My take: This large study shows that CDI is more frequent after antibiotic usage and after usage of acid suppression (particularly with proton pump inhibitor) therapy.
Related blog posts:
- 4 Points for C diff in Inflammatory Bowel Disease
- Overdiagnosis of C difficile with PCR Assays
- Clostridium difficile/Fecal Microbiota Transplantation Video …
- Clostridium difficile: Colonization vs. Symptomatic Infection …
- Clostridium difficile Epidemiology | gutsandgrowth
- Precise Identification of C difficile Transmission …
- Clostridium difficile in IBD | gutsandgrowth
- A C difficile two-fer | gutsandgrowth
- Keeping Up with Clostridium Difficile | gutsandgrowth
- How Common are Clostridium difficile infections …
- Predicting Severe Clostridium Difficile | gutsandgrowth
- Consensus Guidelines on FMT | gutsandgrowth
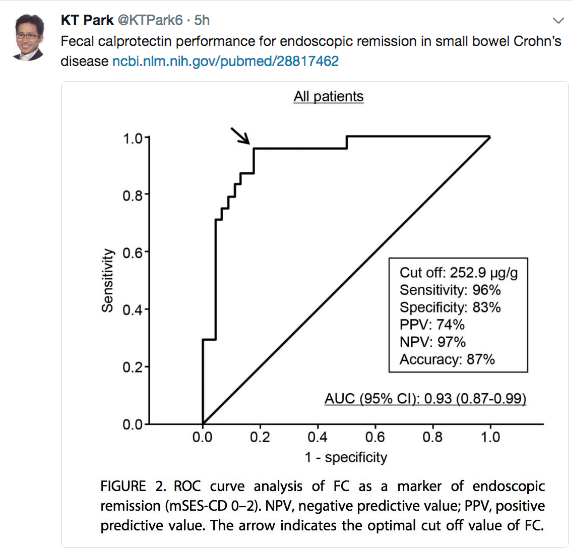
Calprotectin in Triaging Potential Pediatric IBD Cases
Thanks to KT Park’s Twitter feed for this reference: GA Holtman et al.
An excerpt from abstract:
Results Of the 16 eligible studies, authors of 8 studies (n = 1120 patients) provided their data sets. All blood markers and fecal calprotectin individually significantly improved the discrimination between pediatric patients with and those without IBD, when added to evaluation of symptoms. The best marker—fecal calprotectin—improved the area under the curve of symptoms by 0.26 (95% CI, 0.21-0.31). The second best marker—erythrocyte sedimentation rate—improved the area under the curve of symptoms by 0.16 (95% CI, 0.11-0.21). When fecal calprotectin was added to the model, the proportion of patients without IBD correctly classified as low risk of IBD increased from 33% to 91%. The proportion of patients with IBD incorrectly classified as low risk of IBD decreased from 16% to 9%. The proportion of the total number of patients assigned to the intermediate-risk category decreased from 55% to 6%.
Conclusions and Relevance In a hospital setting, fecal calprotectin added the most diagnostic value to symptoms compared with blood markers. Adding fecal calprotectin to the diagnostic workup of pediatric patients with symptoms suggestive of IBD considerably decreased the number of patients in the group in whom challenges in clinical decision making are most prevalent.
From: Inflamm Bowel Dis. 2017 Aug 16. doi: 10.1097/MIB.0000000000001202. [Epub ahead of print]
Vaccination and Inflammatory Bowel Disease -Resources Targeted for Adult Patients
From a recent Gastroenterology & Hepatology –Full Link:
Gastroenterology & Hepatology July 2017 – Volume 13, Issue 7; Vaccination of Patients With Inflammatory Bowel Disease. Francis A. Farraye, MD, MSc
Thanks to John Pohl’s twitter feed for this link that provides recommendations for Adults with IBD.
An excerpt:
G&H What specific resources for vaccinations are available to help gastroenterologists?
FF It is helpful for providers to keep a copy of the Crohn’s and Colitis Foundation’s health maintenance recommendations posted in their office. This 1-page checklist (available at http://www.crohnscolitisfoundation.org/science-and-professionals/programs-materials/ccfa-health-maintenance.pdf) includes all recommended vaccines and also comments on other important health maintenance items, such as screening for cervical and skin cancer, depression, and osteoporosis. In addition, Cornerstones Health has a vaccination checklist (available at http://www.cornerstoneshealth.org/wp-content/uploads/2017/06/Monitoring-and-Prevention-3.10.2017.pdf) that can be downloaded, printed, and placed in each examination room to reinforce the importance of vaccination. Primary care providers as well as gastroenterologists can use these checklists as reminders in their busy practices.
Related blog post:
- Immunization Recommendations from CDC 2013 | gutsandgrowth
- Because It Doesn’t Just Happen to Other People
- Protecting the Most Vulnerable
- Why Rich Kids Get Measles More Often in the U.S.
- The Paradox of Vaccine Resistance
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.

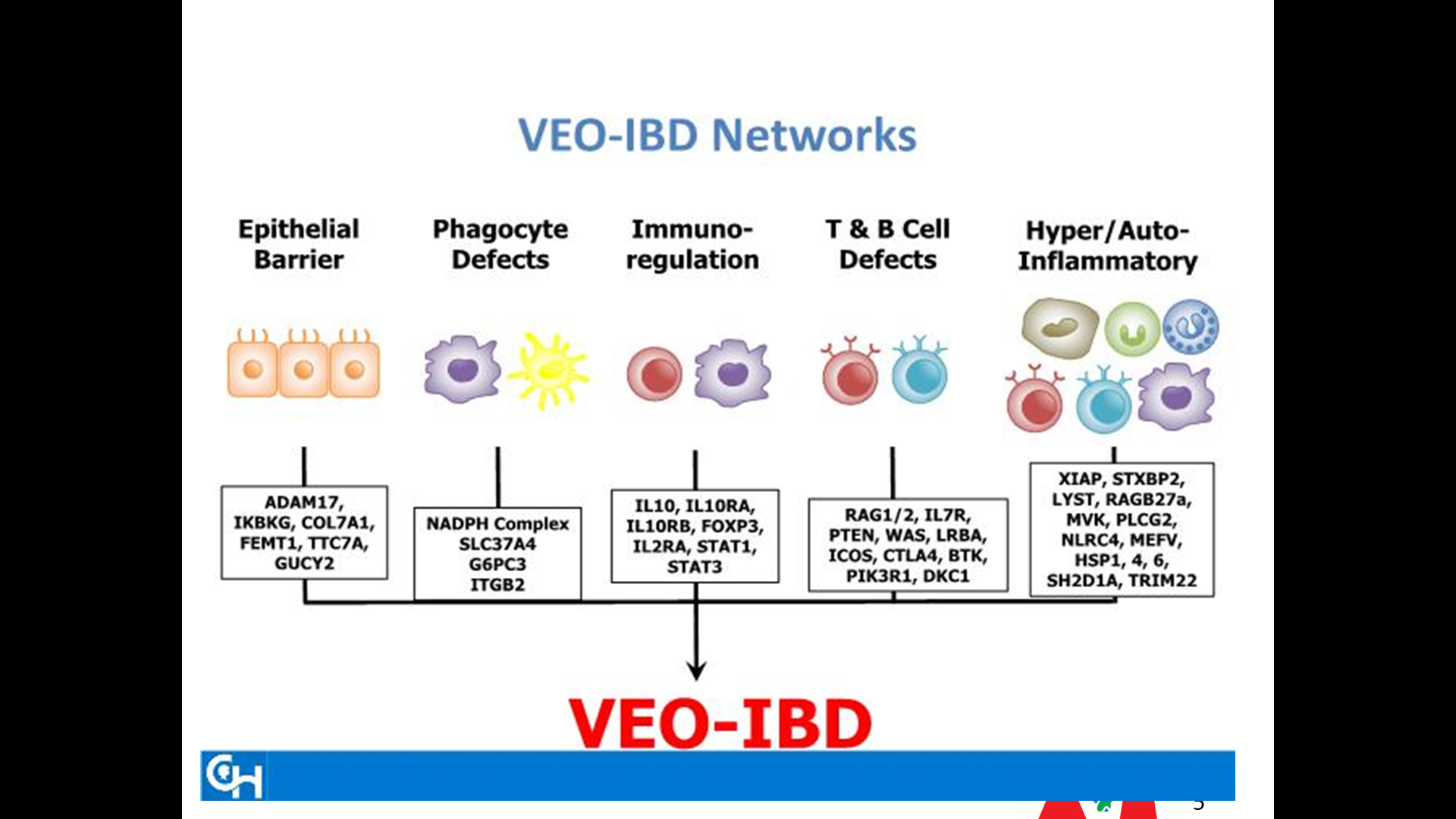
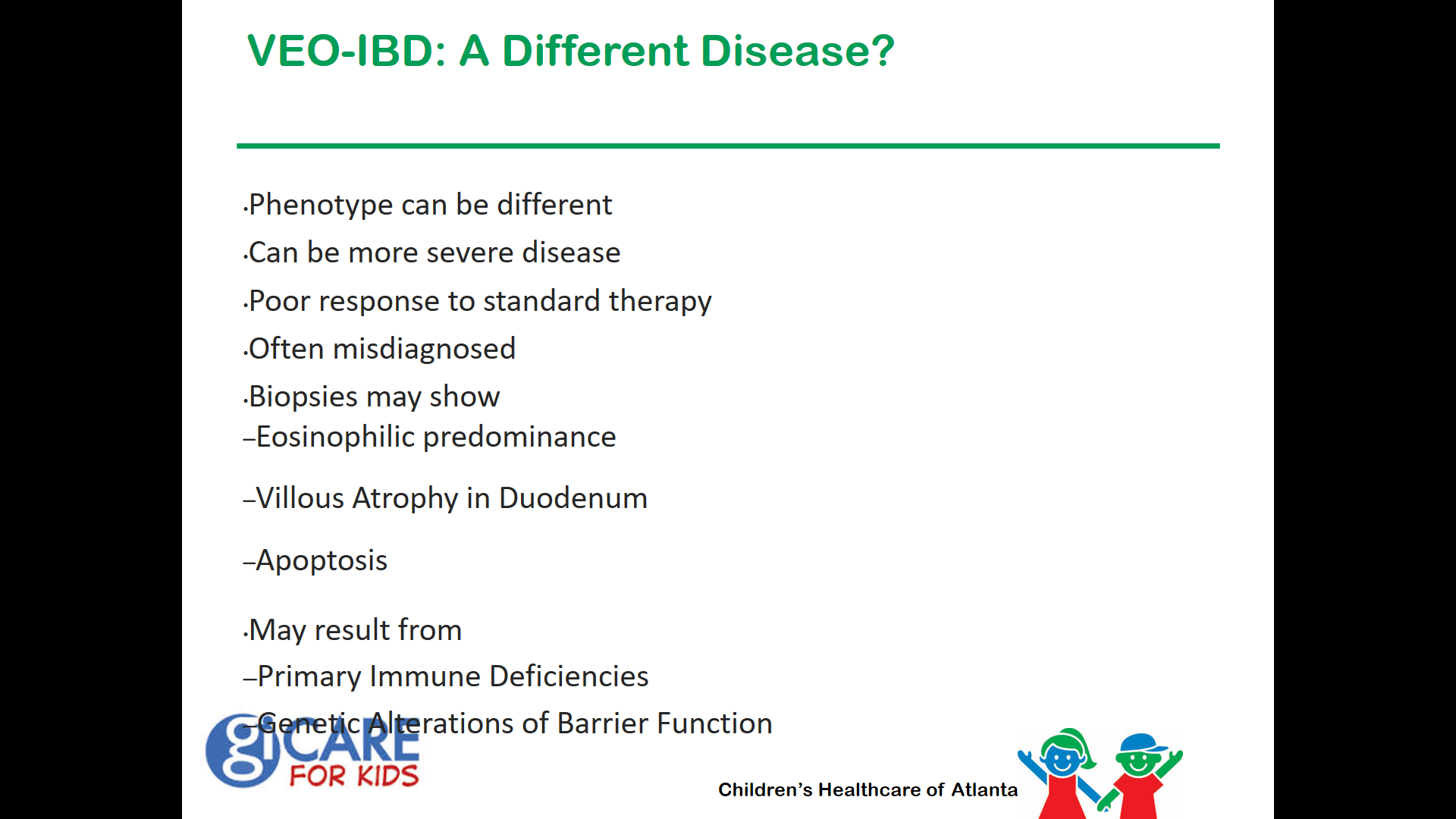
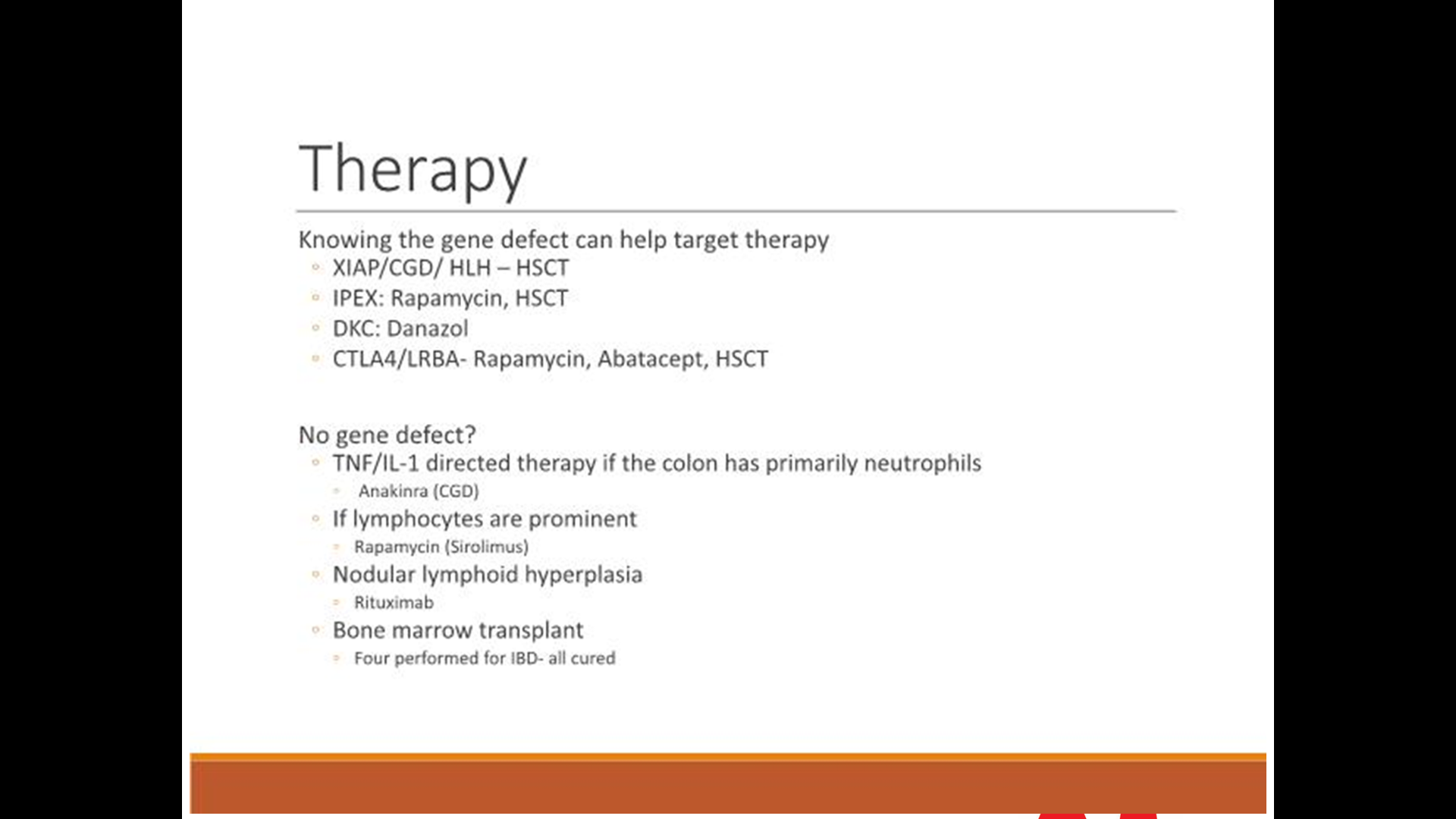
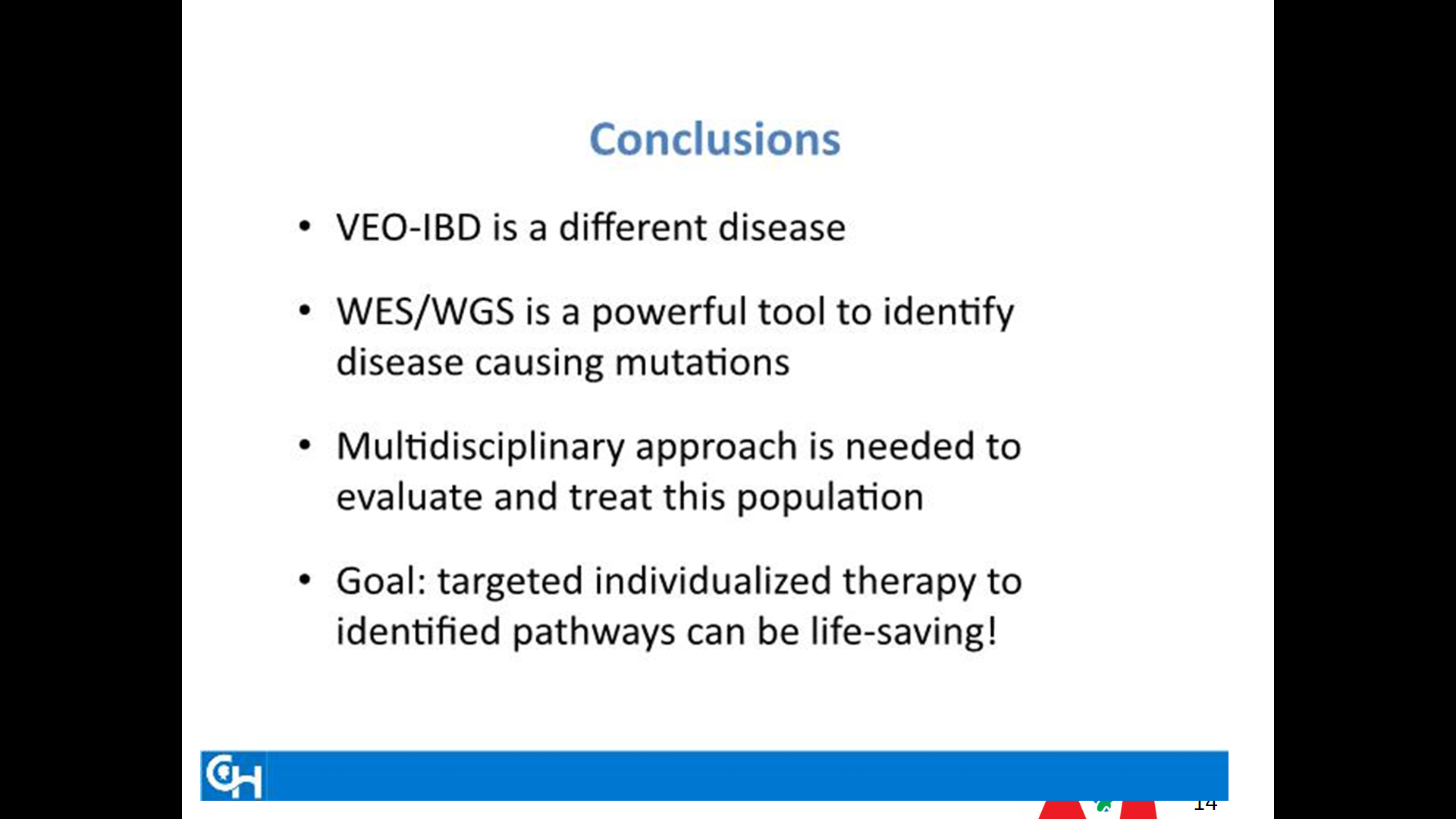
Very Early Onset IBD -Update
Our recent ImproveCareNow group meeting focused on very early onset IBD. Much of the information has been covered on previous posts, including Patterns and Puzzles with very early onset IBD.
Some of the slides -which at the time of presentation were attributed in part to a recent conference in Philadelphia.


Two Viewpoints: Anti-TNF Therapy Shortly After Crohn’s Disease Surgery
A recent AGA perspectives issue provides two viewpoints on when to start/resume anti-TNF therapy after Crohn’s disease surgery:
- Dr. Bressler: Hold The Ant-TNF Therapy
- Dr. Reguieiro: Don’t Delay Anti-TNF Therapy
Dr. Bressler states that he considers anti-TNF therapy for patients with ongoing immune dysfunction after surgery who are at high risk for recurrence. Attributes of high risk disease include the following:
- younger age (<30 years)
- smoker
- two or more surgeries for penetrating disease.
His commentary indicates that a “‘wait and see’ approach is appropriate for most patients. He frequently will measure a calprotectin three months postoperatively and every three months and perform a colonoscopy typically 6-9 months postoperatively. Those with endoscopic recurrence will be placed on anti-TNF therapy.
Dr. Requiero states:
- The most effective way to prevent recurrence is to initiate an anti-TNF within four weeks of surgery. It has been my practice that patients at high risk for postoperative Crohn’s disease recurrence initiate anti-TNF shortly after they are discharged from the hospital.
- If a patient had been on an anti-TNF prior to the surgery, I will usually resume the same anti-TNF after the surgery. In these patients, I do not give a re-induction course unless they had not received the anti-TNF for more than three months prior to surgery.
- Concomitant therapy: “In the majority of patients, I treat with an anti-TNF, I will use a concomitant immunomodulator…One year after surgery, if there is no disease recurrence, I will decrease and often stop the immunomodulator. With the advent of therapeutic drug monitoring, I have a number of postoperative anti-TNF patients on monotherapy without an immunomodulator.
- [In] patients at moderate risk for postoperative recurrence… I perform an ileocolonoscopy six months postoperatively and, if there is evidence of endoscopic recurrence, I add an anti-TNF agent. After finding a high rate of recurrence in these patients, I am beginning to shift my practice to initiating anti-TNFs in this moderate-risk group as well.
My take: I tend to favor Dr. Reguieiro’s approach in my patient population.
Related blog posts:
- AGA 2017 Guidelines for Postoperative Crohn’s Disease
- IBD Shorts and Pediatric Postoperative Crohn’s Disease
- Pediatric Consensus Statement: Perianal Crohn Disease …
- Paris Classification of Pediatric Crohn’s Disease | gutsandgrowth
Image Only: Dappled Crescent Shadows
August 21, 2017 eclipse (2 days ago) caused unusual shadows:

This shadowing was minutes after the peak eclipse with narrow crescents

This shadowing was a few minutes later and with broader crescents
What Happens to Picky Eaters
“Little belly-achers grow up to be big belly-achers and big belly-achers beget little belly-achers” –John Apley
John Apley’s monographThe Child with Abdominal Pains indicates that children with recurrent abdominal pain often grow up to be adults with abdominal pains. A recent study indicates the same type of phenomenon with picky eaters.
A summary of this study in Research Digest: The first study to see if fussy-eating children grow into fussy-eating adults (Thanks to Bonney Reed-Knight for this link.)
An excerpt:
60 per cent of fussy eating children in the study were also fussy eaters at age 23, but fussy eating young adults were no more likely to report signs of eating disorder than their non-fussy peers.
The researchers led by Meredith Van Tine at Stanford University School of Medicine managed to catch up with 61 individuals, now aged 23, who’d participated as children in a long-running study in which their eating habits had been scored by their parents at ages 2, 7, 9.5 and 11, including any signs of fussy eating (being a “selective eater”, having strong likes and dislikes, and only eating a limited variety of foods etc). The participants were now asked to rate themselves on whether they were selective or fussy eaters, and they answered questions about whether they engaged in behaviours related to eating disorders.
Related blog posts:
- Picky Eating and Underlying Psychological Problems
- Afraid to eat -Could be Restrictive Avoidant Restrictive Food Intake Disorder

