Recently, Dr. Laurie Jacobs from CHOA’s palliative care team gave our group a provocative update on communication strategies in children with severe illness. My notes below may contain errors in transcription and in omission. Along with my notes, I have included many of her slides.
Having a pre-meeting with other members of health care team is a key part in setting up an effective meeting with parents
Delivering news: 1) Provide a straightforward Headline: ‘We are here to discuss xyz’ 2)Be clear. ‘To be clear is to be kind’ 3) Then STOP TALKING. This let’s the family process
Sometimes even delivering bad news can be met with relief by families who have been waiting for a diagnosis
Respond to emotion with NURSE mnemonic: Name, Understand, Respect, Support, Explore
What if the ‘family doesn’t get it?’ Do they understand (can they repeat back)? Most often the family has a different perspective; they may think we are wrong
Be careful to avoid offering decisions where there are not actual decisions to be made
Our own values/beliefs are often introduced even though quality of life is in the eye of the beholder
Tube feeds can be considered forms of ‘artificial nutrition.’ There are situations in which families need to know that it is not always required
Parenteral nutrition is more invasive and associated with more active parental decision-making
Decisions may change based on change in patient circumstances
There is not a single right answer with difficult decisions. There are trade-offs between longevity and QOL
Anything that we would allow parents not to start, can be stopped at any time from an ethical standpoint
Background: Nearly two decades ago, the Eight Americas study offered a novel lens for examining health inequities in the USA by partitioning the US population into eight groups based on geography, race, urbanicity, income per capita, and homicide rate. That study found gaps of 12·8 years for females and 15·4 years for males in life expectancy in 2001 across these eight groups. In this study, we aimed to update and expand the original Eight Americas study, examining trends in life expectancy from 2000 to 2021 for ten Americas (analogues to the original eight, plus two additional groups comprising the US Latino population), by year, sex, and age group.
Methods: The authors tabulated deaths from the National Vital Statistics System and population estimates from the US Census Bureau and the National Center for Health Statistics from Jan 1, 2000, to Dec 31, 2021.
Key findings: .
At the beginning of the 21st century, there was already a 12.6-year gap in life expectancy among Americas, but this gap grew even larger during the 2000s and 2010s and accelerated to 20.4 years after the first 2 years of the COVID-19 pandemic.
One’s life expectancy varies dramatically depending on where one lives, the economic conditions in that location, and one’s racial and ethnic identity.
There are limitations with the data that were used. For example, there is known to be substantial misreporting of race and ethnicity on death certificates
My take (borrowed from the authors): “The extent and magnitude of health disparities in the USA are truly alarming. In a country with the wealth and resources of the USA, it is intolerable that so many are living in conditions and with health outcomes akin to those of an entirely different country.”
‘Fistula Foundation which arranges obstetric fistula repair. This restores a woman’s life after this life-altering complication –a corrective surgery that costs just $619 per person
Muso Health helps reduce childhood mortality. In Mali, this organization reduced childhood mortality by 95%. The cost of bringing one more person into the Muso health care network is only $22 per year.
Reach Out and Read. This U.S-based charity allows doctors to “prescribe” reading to the child. This promotes reading as well as childhood well-child visits.
Crisis Text Line is for those who want to volunteer, rather than donate. This organization trains (15-20 hrs) volunteers to help individuals needing mental health support. “More than 90 percent of the volunteers report that their own mental health improves as a result of their participation.”
M Zimmer et al. Pediatrics 2024; 154: e2024067783.
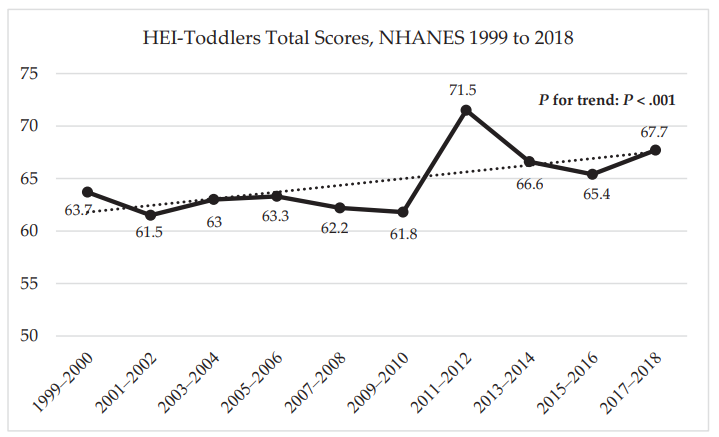
Methods: This serial cross-sectional analysis of National Health and Nutrition Examination Survey (NHANES) data was performed with 2541 toddlers from 10 NHANES cycles from 1999 to 2018.
Key findings:
Toddler diet quality improved significantly from 1999 to 2018 (P < .001), from 63.7 points on average in 1999-2000 to 67.7 points in 2017-2018
A significant positive linear trend in total diet quality was observed for all socioeconomic status groups (P < .05)
HEI-Toddlers -Healthy Eating Index has total score ranging from 0-100 points with higher score indicating healthier diets.
In the discussion, the authors note that other age groups besides toddlers have seen modest improvements in diet. Even small improvements can be consequential on a population-basis. In adults, a 4-point increase in HEI scores has been associated with a reduced risk of cardiovascular disease. The strongest improvement between 1999 and 2018 in toddler diet quality was in scores for added sugars…attributed to declines in added sugars from sweetened beverages. “A heightened awareness of added sugars in sweetened drink products among caregivers themselves may have led to a cultural shift around feeding toddlers less sweetened drinks.”
While in toddlers there was no significant difference in dietary scores based on socioeconomic status, “, the diet quality gap for adults has widened over time by SES,14,15 race and Hispanic origin, and Supplemental Nutrition Assistance Program participation status.”
“Although toddlers do not receive school meals, their diets can be similarly impacted by other large-scale programs like the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) and the Child and Adult Care Food Program. Changes to the WIC food package have been consistently linked to improved child diet quality, and may have contributed to the gains in toddler diet quality observed in this study.”
Study limitations are related to self-reported dietary intake.
My take: It feels like improving diet quality is like swimming against a strong tide. Yet, this study shows improvements can happen. Ongoing efforts are needed to encourage healthier diets.
EP Kirk et al. NEJM 2024; 391: 1877-1889. Nationwide, Couple-Based Genetic Carrier Screening
One of the drawbacks with genetic screening has been identifying too many problems. Everyone has pathogenic mutations but many do not have effective treatments; in addition, many may be inconsequential if your partner does not share a similar genetic mutation (for autosomal recessive conditions). Furthermore, counseling everyone with genetic mutations is time-intensive. With this background, it is easy to see why a couple-based testing approach makes sense. In this study of an Australian genetic carrier screening program, couples had testing of at least 1281 genes with more than 750 serious diseases as part of the Mackenzie’s Mission project. Variants of uncertain significance were not reported.
Key findings:
An estimated 45.9% of those invited to participate underwent reproductive genetic carrier screening
9107 couples completed screening, and 175 (1.9%) were newly identified as having an increased chance of having a child with a genetic condition for which we screened
180 (2.0%) were known, before participation in the study, to have an increased chance of having offspring with at least one genetic condition (due to family history or consanguinity)
Of the 45 couples (25.7%) in which the female partner was pregnant when they received the result, 29 (64%) decided to have the fetus genetically tested, and 24 of these couples received normal test results. Of the 5 couples whose pregnancy was affected, 4 elected to end the pregnancy
Of the 130 couples in which the female partner was not pregnant at the time of genetic testing, 95 (73.1%) indicated an intention to use in vitro fertilization with preimplantation genetic testing for monogenic conditions.
Overall, 134 of 175 couples (76.6%) with a newly identified increased chance chose to alter their reproductive plans
Discussion Points:
“92.7% of participants carried at least one pathogenic or likely pathogenic variant. With this prevalence and in this framework, reporting individual carrier results would be a burden on health systems. For example, one study showed a median time of 64 minutes to provide genetic counseling regarding results of reproductive genetic carrier screening.36“
“Decisional regret was generally low,32 a finding that suggests that most participants valued the information provided by the screening.”
42% of couples had increased risks for diseases that would not have been identified using a previous list of 113 genes recommended by The American College of Medical Genetics and Genomics (ACMG).38 “As genomic testing technology advances, it is becoming possible to screen larger numbers of genes, and thus, any gene that meets criteria for inclusion, such as criteria that pertain to the severity of associated disease and to technical capability,1 can be screened.”
“We limited reporting to variant combinations predicted to result in a serious childhood-onset condition or a condition in which early intervention can improve prognosis…Variants known to result in a mild condition or an adult-onset condition were not generally reported unless early intervention would improve prognosis. This approach aimed to minimize uncertain and ambiguous information and provide results that had high clinical usefulness.”
My take: Given the improvement in cost of genetic screening, this type of approach is quite practical and would not result in every family having to meet with a genetic counselor.
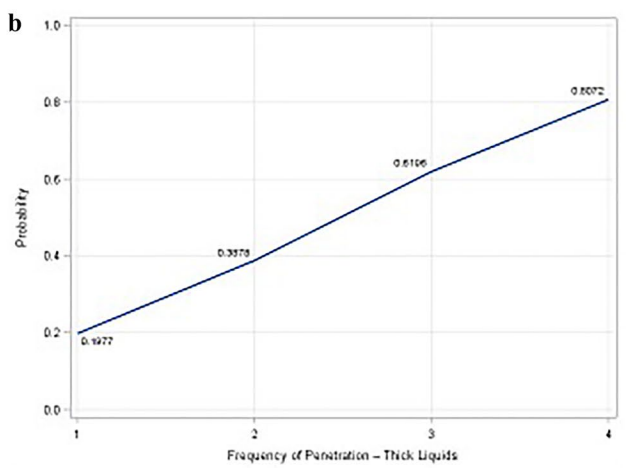
This was a retrospective study with 97 patients over a 6 month period in 2018. The authors note that “there is no universally accepted protocol for pediatric video swallows across ages and conditions.”
Methods: Depth of penetration and/or aspiration and reaction were classified according to the 8-point Penetration–Aspiration scale [JC Rosenbek, et al.Dysphagia11, 93–98 (1996). https://doi.org/10.1007/BF00417897]. The frequency of penetration events and aspiration was grouped into categories: none (1); infrequent or occasional episodes (at least 1 event to less than 30%) (2); intermittent episodes (30–40% of total swallows) (3); frequent episodes (50% or greater of total swallows) (4). Data for all swallowing parameters was stratified by bolus type (thin liquid, thickened liquid, puree solid). All VFSS were independently scored by two speech-language pathologists and two radiologists.
Key findings:
Aspiration was seen in 21% of patients (n=20 of 97).
Penetration events were more frequent and occurred in 64% of participants (n=62 of 97). . Of patients with any penetration events, 30% also had documented aspiration
Frequency of penetration and aspiration: 80% of patients showing frequent penetration [frequency 4] demonstrating aspiration compared to 2.3% of patients with isolated penetration [frequency 1]. There was a higher risk of aspiration at lower frequency penetration if this occurred with thicker liquids (see below)
Depth of penetration and aspiration:. For patients with penetration contacting the vocal folds [depth 5], nearly 95% demonstrated documented aspiration within the same study; however, those with depths 1-3 had minimal risk of aspiration (see below). There was a higher risk of aspiration at shallow depths with thicker liquids.
My take (borrowed from authors): “children with shallow, intermittent penetration events without associated aspiration are likely to be demonstrating clinically insignificant events. Such children are therefore not appropriate candidates for compensatory or alternative feeding strategies such as changes in mode of delivery (e.g., gastrostomy tube), alteration of flow rate, or modification of liquid viscosity, such as thickened feedings.”
There are a lot of interesting recent case reports on the JPGN Reports website. A recent example includes the following:
Mostafavi et al report (JPGN Reports 2024;5:511–513. Open Access! Endoscopic diagnosis of asymptomatic appendicitis in a pediatric patient) on the incidental diagnosis of appendicitis. A followup colonoscopy in a 14 year-old with ulcerative colitis identified purulent fluid from the appendiceal orifice after ileal intubation; subsequently, after MRI imaging, an appendectomy was performed. The appendicitis was thought to be unrelated to the ulcerative colitis.
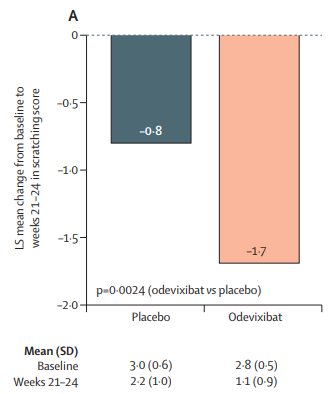
Methods: “The ASSERT study was a phase 3, double-blind, randomised, placebo-controlled trial that enrolled patients at 21 medical centres or hospitals in ten countries” with 52 patients (enrolled 2021-2022). “The primary efficacy endpoint was change in caregiver-reported scratching score (on the PRUCISION instrument; range 0–4) from baseline to weeks 21–24.” The treatment group received odevixibat 120 µg/kg per day.
Key findings:
There were improvements in both scratch scores and bile acid concentrations
There were improvements in sleep parameters including falling asleep and ability to sleep without a caregiver
Adverse events: diarrhea was reported in ten (29%) of 35 patients who received odevixibat and in one (6%) of 17 patients who received placebo; all cases were mild in severity and no cases of diarrhea led to treatment interruption or discontinuation
Scratch Scores:
Bile Acid Levels
Other points:
Overall, 50 (96%) of the 52 patients chose to enter the open-label extension study
The authors note that this is the first randomized placebo-controlled trial for Alagille syndrome
A direct comparison of odevixibat and maralixibat in patients with Alagille syndrome is complicated by differences in study design and endpoints across the their studies
My take (borrowed in part from authors): “As pruritus is a major driver of liver transplantation in patients with Alagille syndrome, these results suggest that odevixibat could have the potential to delay or prevent liver transplantation”
Background: There have been concerns that JAK inhibitors (JAKi), like tofacitinib (Xeljanz) and upadacitinib (Rinvoq) could increase the risk of major adverse cardiovascular events (MACE); as such, the FDA has placed warnings on these medications (see blog post: FDA Slaps Restrictions on JAK Inhibitors Over Serious Safety Risks).
Alsakarneh and colleagues conducted a retrospective cohort study using the TriNetX database to identify adult patients with IBD who were treated with JAKi or anti-TNF therapy after diagnosis. After matching patients in the JAKi cohort [n=3740] with patients in the anti-TNF cohort [n=3740], the research team looked for MACE and VTE within a year of medication initiation…
After excluding those with a history of a prior cardiovascular event, 57 patients (1.76%) in the JAKi cohort developed MACE, compared with 63 patients (1.94%) in the anti-TNF cohort. There weren’t significant differences between the groups in MACE (adjusted hazard ratio [aHR], 0.99) or VTE (aHR, 0.9).
Among patients aged ≥ 65, 25 patients (5.3%) in the JAKi cohort developed MACE, as compared with 30 patients (6.4%) in the anti-TNF cohort.
My take: Several studies now have not identified an increased risk of JAKi compared to other therapies for IBD. Perhaps, this will lead to a change in labeling by the FDA which has stated that JAKi should be used only in those with prior anti-TNF failure.
Methods: VIVID-1 was a global phase 3, randomized, double-blind, double-dummy, placebo-controlled and active-controlled, treat-through study which enrolled 1150 patients with moderate-to-severe Crohn’s disease. There were three treatment groups: mirikizumab group, ustekinumab group, and placebo group. In each group, 48-49%were considered “biologic-failures” including 45-46% who were anti-TNF failures.
Key findings:
Discussion points:
Early treatment effect: “Symptomatic improvement was evident as early as week 4 accompanied by a statistically significant reduction in high-sensitivity CRP and faecal calprotectin, and endoscopic response was seen at week 12.”
Compared to ustekinumab: “Mirikizumab reached non-inferiority versus ustekinumab for clinical remission by CDAI at week 52…mirikizumab showed statistically significantly greater improvements from baseline in fecal calprotectin and CRP compared to ustekinumab. In addition, a greater percentage of patients reached the combination endpoint of endoscopic response and clinical remission by CDAI at week 52.”
Comparison across treatment trials: “. At week 52, 45∙4% of patients treated with mirikizumab met the endpoint of clinical remission by CDAI in the treat-through analysis with composite endpoint, 54∙1% met the endpoint in the treat-through analysis, and 64∙3% met the endpoint in the responder analysis. This example, with a range of nearly 20% percentage points depending on analysis type, shows the profound limitations in comparing unadjusted outcomes across phase 3 trials.” The authors note other differences in trial design between VIVID-1 and SEQUENCE (risankizimab) and state “no conclusions on relative efficacy can be drawn.”
My take: This study shows that mirikizumab is effective in adults with moderate-to-severe Crohn’s disease with and without prior biologic treatments. Pediatric studies are underway.
Background: The exposure–response relationship for the intravenous (IV) formulation of infliximab is well established, with multiple studies demonstrating that higher trough concentrations (C-trough) are associated with improved patient outcomes…However, the 2-week cycle of subcutaneous administration showed many-fold higher C-trough than the 8-week cycle of IV-IFX. Direct comparison of C-trough between SC- and IV-IFX is not appropriate because of different bioavailability and concentration–time profile. It is also not appropriate to apply the C-trough thresholds that predict achieving the therapeutic targets for IV.
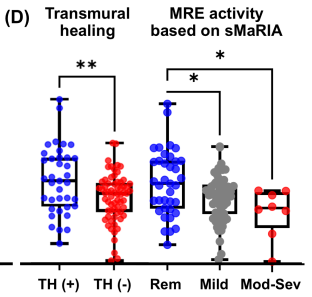
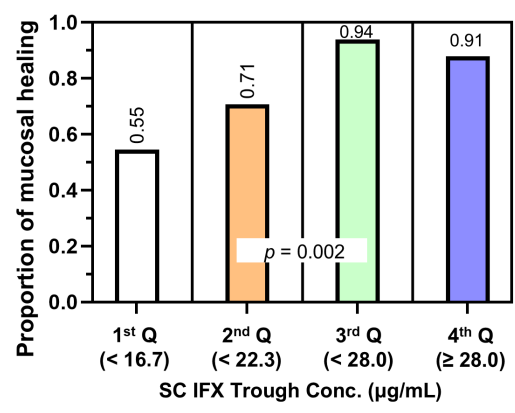
This was a cross-sectional retrospective study with 124 patients with Crohn’s disease (CD) who had received SC-IFX maintenance therapy for ≥6 months. SC-IFX C-trough was measured immediately before SC-IFX injection. Key findings:
Mucosal healing (MH) was noted in 77.9% (74/95) and transmural healing (TH) in 36.3% (37/102).
SC-IFX C-trough was significantly higher in patients with MH (24.1 vs.16.9 μg/mL; p=0.001) and TH (26.0 vs. 20.5 μg/mL; p=0.007) than in those without.
Discussion:
Target trough levels: In this study, the authors found that “the C-trough thresholds for clinical remission, biochemical remission, MH and TH were 12, 16, 18 and 30 μg/mL, respectively, based on ROC analysis. The C-trough of SC-IFX increased with the depth of remission.”
Why trough level targets may differ between IV administration and SC: Administration via the IV route results in early and rapid peak concentration followed by a steady decline to trough, whereas administration via the SC route has slower absorption, lower bioavailability, lower peak concentration and smaller differences between peak and trough concentrations.
The authors note that a study by Ye et al (United European Gastroenterology Journal; 2020: 8: 385–386) with 55 patients found that a C-trough >26.6 mcg/mL achieved clinical remission and fecal calprotectin levels <250 mcg/g at week 54 in 79% and 91% respectively compared to 46% and 62% in those with with C-trough <16.4 mcg/g.
These C-trough levels are significantly higher that the median C-trough levels of standard dosing (120 mg biweekly) in a phase 1 dosing RCT which was only 13.3 mcg/mL (S Schreiber et al. Gastroenterology 2018; 154: 1371). The dosing of 180 mg and 240 mg biweekly resulted in C-trough levels of 19.9 mcg/mL and 26.5 mcg/mL respectively.
My take: This study suggests that therapeutic drug monitoring will have different targets with SC-IFX than with IV-SC. SC formulations will offer more convenience. However, more effort will be needed to make sure patients are adherent with therapy in order to achieve optimal outcomes.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.